Vol. 10, No. 1, 65-70, 2007
책임저자:전 욱, 서울시 영등포구 영등포동 2가 94-200
}150-719, 한강성심병원 화상외과 Tel: 02-2639-5793, Fax: 02-2678-4386 E-mail: [email protected]
화상에서 메디폼-실버(메디폼-S)의 임상적 유용성
하태순ㆍ조용석ㆍ김도헌ㆍ허 준ㆍ전 욱ㆍ김종현ㆍ신현선
1ㆍ김애심
1ㆍ노순예
1한림대학교 의과대학 한강성심병원 화상외과학교실, 1화상센터
The Clinical Effectiveness of Medifoam-silver in Burns
Tae Soon Ha, M.D., Yong-suk Cho, M.D., Do-hern Kim, M.D., Jun Hur, M.D., Wook Chun, M.D., Jong Hyun Kim, M.D., Hyun Sun Shin, R.N.1, Ae Sim Kim, R.N.1, and Soon Ye Noh, R.N.1 Department of Burn Surgery, 1Burn Center, Hangang Sacred Heart Hospital, College of Medicine, Hallym University, Seoul, Korea
Backgrounds: The polyurethane foam dressing has shown
outstanding effectiveness in treating superficial second and mid-second degree burns. Yet its clinical usage in treating deep second and third degree burns has been limited be- cause pathogens can proliferate during eschar separation due to lack of antibacterial property in conventional polyur- ethane foams. Medifoam-silver (Biopol, Korea) is newly de- veloped polyurethane foam dressing with the silver ions im- pregnated to prevent proliferation of pathogens and enhance the clinical effectiveness compare to conventional polyur- ethane foam dressing available in current market. The study has been conducted to discover the effectiveness of polyur- ethane foam dressing with silver ions impregnated.Methods: The clinical study was performed on second and
third degree burn areas including donor sites.Results: Medifoam-S was applied on donor sites of 24
patients. The mean age was 42.3 (4∼87) years and the mean burn area was 37.5 (5∼72)% of TBSA. Most donor sites were larger than 1,000 cm2. All donor sites of 24 patients were successfully re-epithelialized at the mean time of 9.5 (7∼15) days from the first date of skin grafts taken. Medifoam-S was applied on burn areas of 31 patients. The mean age was 30.6 (1∼77) years and the mean burn area was 12.6 (1∼
38)% of TBSA. The area of Medifoam-S application was var- ied from 1∼18% of total body surface area. Re-epithelializa- tion occurred in the mean of 18.6 (5∼29) days in 27 patients.
Eschar separation occurred in the mean of 14.3 (12∼18) days in 4 patients and skin grafts were immediately applied
since granulation tissue formed underneath the eschar. No complication and side effect were noted in all patients and all exudates were well absorbed.
Conclusions: Our study has shown successful clinical usage
of Medifoam-S in all types of burns including deep dermal burns as primary dressing materials. (Journal of KoreanBurn Society 2007;10:65-70)
Key Words:
Polyurethane foam dressing, Burns서 론
2도 화상의 치유 기전은 진피 내에 위치한 피부부속기나 창상 연에서의 상피세포의 이동에 의하게 된다. 이러한 상 피세포의 이동은 상처 표면이 습윤 환경을 유지하고 상처 에서 나오는 삼출액이 없을 때 가장 빨리 일어나게 된다.
이를 위해 개발된 드레싱이 폴리우레탄 폼 드레싱이다.
1-3)이들은 상처에서 나오는 섬유소성 삼출액을 흡수하고 상처
표면은 습윤 상태를 유지하게 하여, 딱지 생성을 예방하고
재상피화를 아주 빨리 일으키게 한다.
4-6)이러한 폼 드레싱
재는 표재성 2도 화상 및 중간성 2도 화상까지는 아주 뛰어
난 재상피화 치료 효과를 볼 수가 있다(Fig. 1). 하지만 심재
성 2도 이상의 깊은 화상이나, 오염이 동반된 찰과상에서는
그 사용이 제한되어왔다. 그 이유는 이러한 폴리우레탄 폼
드레싱 자체가 항균 성분을 가지고 있지는 않기 때문에 비
교적 두꺼운 가피가 있는 경우나 감염의 증거가 있을 시에
는 사용이 제한될 수밖에 없다. 즉, 가피 분리 시에는 균이
상처에 자라게 되며 이는 상처 감염으로 연결될 수 있기
때문이다. 또한 중증화상의 경우 혹은 환자의 전신상태가
좋지 않은 경우 기존의 폼 드레싱으로 드레싱을 하여도 피
부 공여부 감염이 종종 관찰되게 되는데, 이런 상황에서도
역시 그 사용이 제한되어왔다. 이러한 단점을 보완하기 위
해 기존의 폼 드레싱(메디폼, 바이오폴)에 은 입자를 첨가
한 메디폼-S가 개발되었기에 이의 임상 실험 결과를 보고하
는 바이다.
Table 1. Results. Medifoam-S on Donor Sites of 24 Patients Sex/ Mode of Burn% Duration of Specific Case age burns (TBSA) epithelization findings
1 M/33 Scalding 43% 7
2 M/21 Flame 31% 8
3 M/53 Flame 47% 9
4 M/50 Flame 33% 13 Malnutrition
5 M/37 Electric 30% 8
6 M/45 Flame 37% 9
7 M/30 Chemical 21% 8
8 M/27 Flame 41% 8
9 F/4 Flame 24% 8
10 M/49 Flame 50% 12 Renal failure
11 F/72 Flame 30% 13
12 M/61 Flame 57% 10
13 F/87 Flame 18% 15
14 M/51 Chemical 60% 11
15 F/41 Flame 37% 9
16 M/21 Chemical 70% 10
17 M/37 Flame 36% 8
18 M/68 Flame 44% 10
19 M/46 Flame 72% 10
20 M/49 Flame 29% 9
21 M/32 Scalding 5% 8
22 M/50 Flame 30% 9
23 F/6 Flame 20% 8
24 M/45 Flame 36% 8
Fig. 1. Advantage of conventional polyurethane foam dressing. (A) very easy to use, (B) outstanding effectiveness in treating superficial 2nd and mid 2nd degree burns.
대상 및 방법
한강성심병원 화상센터에 입원한 중증화상환자 중 피부 이식을 위한 피부 공여부와 2도, 3도 화상 부위를 대상으로 하였다. 메디폼-S는 경우에 따라 1∼2일마다 한번 씩 교체 하였고, 모든 환부는 한강성심병원 화상센터 전임간호사에 의해 디지털카메라로 매 드레싱마다 촬영되었다. 결과판독 은 두 명의 화상외과 전문의에 의해 이루어졌다.
결 과
24명의 환자의 피부이식술을 위한 공여부에 메디폼-S 드 레싱을 하였다. 저자는 피부의 두께를 Zimmer air derma- tome으로 8∼10/1,000인치로 채취하여 사용한다. 24명 화 상환자의 평균 연령은 42.3 (4∼87)세였으며, 평균 화상 면 적은 체표면적의 37.5 (5∼72)%였다. 공여부의 면적은 대부 분 1000 cm
2이상이었다. 24명 모두에서 재상피화가 성공적 으로 일어났으며, 그 기간은 피부이식술 시행일로부터 평 균 9.5 (7∼15)일 소요되었다. 환자의 나이가 젊을수록 빨리 치유되었으며 고 연령, 패혈증, 광범위화상 혹은 심각한 영 양부족 상태를 보이는 환자 군에서는 상대적으로 치유가 지연되었다. 기존의 폼 드레싱으로 공여부 감염이 발생한 경우에도 메디폼-S 드레싱을 하면 바로 호전되었다(7예에 서). 만일 모든 예에서 처음부터 메디폼-S를 적용하였더라 면 재상피화 기간이 더욱 단축되었을 수 있다(Table 1).
31명의 환자에서는 화상부위에 직접 메디폼-S를 사용하 였다. 31명 환자의 평균 연령은 30.6 (1∼77)세였으며, 평균 화상 면적은 체표면적의 12.6 (1∼38)%였다. 메디폼-S의 적 용면적은 체표면적의 1∼18%까지 다양하였다. 원인별로 분류하면 화염화상이 8예, 열탕화상이 19예, 전기 스파크에 의한 섬광화상이 2예, 전기화상이 1예, 접촉화상이 1예였 다. 27명의 환자에서 평균 18.6 (5∼29)일만에 재상피화가 이루어졌으며, 4명의 환자에서는 평균 14.3 (12∼18)일째에
가피 분리가 성공적으로 일어났으며 그 밑에 육아조직이 보여 바로 식피술을 시행하였다. 수술 없이 치료한 27예 중 에서 5예에서는 심재성 2도에 3도 화상이 약간 섞여져 있었 으나 그 부위의 크기가 아주 작어 그냥 메디폼-S 드레싱으 로만 치료하였다(Table 2).
모든 예에서 과민반응과 같은 부작용은 없었으며 삼출액
흡수는 아주 잘되어 삼출액이 상처에 남아있지는 않았다.
Table 2. Results. Medifoam-S on Burn Wounds of 31 Patients
Duration (day) of
Case Sex/age Mode of burns Burn% (TBSA) Specific findings
epithelization
1 M/31 Flame 16% 14
2 M/50 Flame 18% 27
3 M/34 Flame 15% 18 ES*, 3rd degree, STSG
4 F/1 Scalding 22% 25
5 M/43 Flame 14% 25
6 M/44 Flame 38% 28
7 M/51 Flame 21% 29
8 M/27 Flash 7% 13
9 M/44 Scalding 18% 15
10 F/2 Scalding 20% 16
11 M/36 Flash 18% 20
12 F/1 Scalding 5% 5 Superficial 2nd degree
13 M/33 Scalding 6% 13 Mid 2nd degree
14 F/29 Scalding 6% 14 Deep 2nd degree
15 F/35 Scalding 1% 22 Deep 2nd degree
16 M/50 Flame 15% 13 ES*, 3rd degree, STSG
17 F/1 Scalding 5% 12 ES*, 3rd degree, STSG
18 F/54 Scalding 7% 10 Mid 2nd degree
19 M/38 Scalding 29% 13 Deep 2nd degree
20 M/73 Scalding 2% 27 3rd degree
21 M/30 Contact 1% 29 3rd degree
22 M/47 Scalding 4% 11 Mid 2nd degree
23 M/32 Electrical 31% 14 3rd degree, STSG
24 M/3 Scalding 3% 26 3rd degree, granulation tissue formation
25 M/1 Scalding 4% 11 Deep 2nd degree
26 M/22 Scalding 20% 27 Deep 2nd degree, 3rd degree
27 F/77 Scalding 2% 17 Deep 2nd degree
28 F/1 Scalding 3% 16 Deep 2nd degree, 3rd degree
29 M/5 Scalding 18% 11 Mid 2nd degree
30 M/46 Scalding 2% 23 Deep 2nd degree
31 M/8 Flame 19% 15 Mid 2nd degree
ES*: eschar seperation
Fig. 2. Structure of Medifoam-S (A) composed by 2 layers (protection, absorption layer) and wound contact site contains silver sulfadiazine, (B) SEM of Medifoam-S. It shows small and homogeneous pore (50∼100 um). So it can possess high absorp- tion power (1.2 g/1 cm2).
고 찰
기존의 폴리우레탄 폼 드레싱의 단점은 심재성 2도 및 3도 화상에서는 오히려 치료기간이 길어져 사용이 불가능하였
으며, 중증화상 환자의 피부 공여부에 사용할 때에도 이따
금씩 발생하는 얇은 층을 가지는 neo-eschar의 생성도 문제
가 되었었다. 이는 기존의 폼 드레싱이 상처 표면을 젖어있
도록 하는 습윤드레싱이면서, 또한 상처에서 나오는 삼출
액을 흡수하여 상피세포의 이동이 아주 빠르게 한다는 장
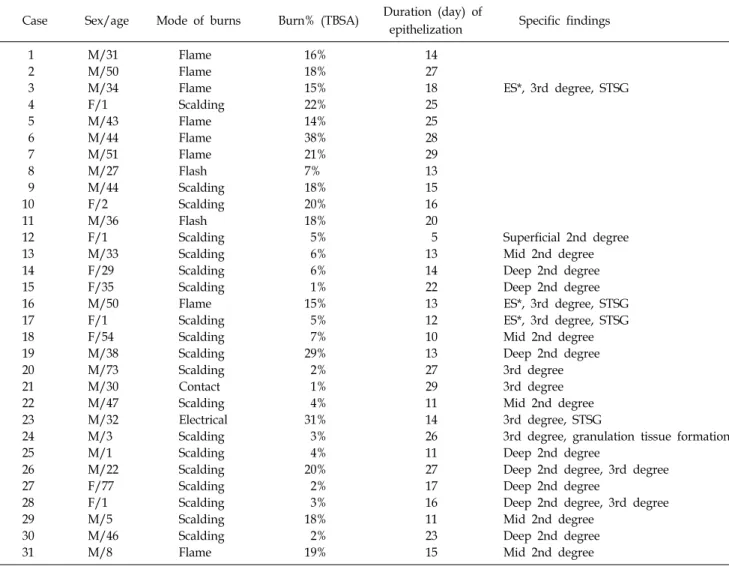
Fig. 3. Clinical cases (donor site for skin graft), flame burn 20% TBSA, F/6. (A) post op. 3 day, (B) post op. 4 day, (C) post op.
5 day, (D) post op. 6 day, (E) post op. 7 day, (F) post op. 8 day, it shows complete reepithelialization.
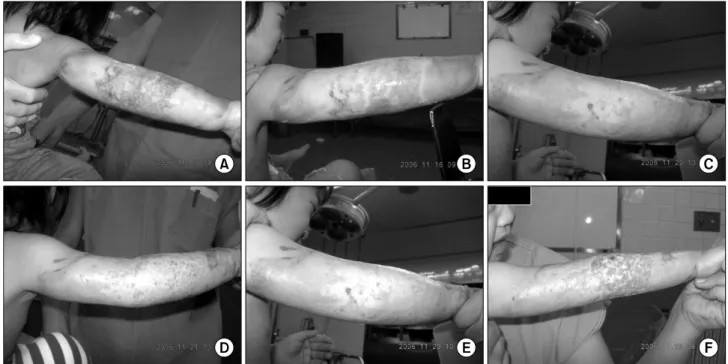
Fig. 4. Clinical cases (donor site for skin graft), flame burn 33% TBSA, F/50, with renal failure. (A) post op. 3 day, (B) post op.
6 day, (C) post op. 7 day, (D) post op. 8 day, (E) post op. 10 day, (F) post op. 12 day, it shows complete reepithelialization.
점이 있지만, 항생 물질이 포함되어있지 않아 가피의 분해 및 분리를 빠르게 진행시키지 못한다는 단점이 있기 때문 이었다. 메디폼-S는 전세계적으로 가장 일반적으로 사용되 는 화상 연고인 silver sulfadiazine을 환부 접촉면에 도포하
여 기존의 장점은 모두 가지면서 심재성 2도 화상이나 감염
이 의심되는 찰과상에서도 사용이 가능하게끔 만든 제품이
다. 물론 silver sulfadiazine의 농도를 높이면 감염 예방에
는 좋겠지만 흡수력이 떨어지면 안 되기에 흡수력을 기존
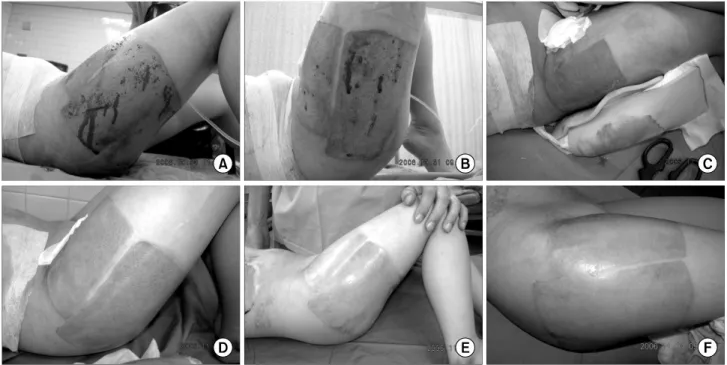
Fig. 5. Clinical cases (2nd degree burn wound), electric flash burn 18% TBSA, M/36. (A) post burn 2 day, (B) post burn 2 day, (C) post burn 6 day, (D) post burn 6 day, (E) post burn 7 day, (F) post burn 13 day, it shows complete healing state.
Fig. 6. Clinical cases (2nd degree burn wound), scalding burn 2% TBSA, F/77, with Diabetes Mellitus. (A) post burn 6 day, (B) post burn 7 day, (C) post burn 8 day, (D) post burn 11 day, (E) post burn 14 day, (F) post burn 17 day, it shows complete healing state.
제품처럼 유지할 수 있는 한에서, silver sulfadiazine의 농 도를 조절하였다. 즉 기존의 메디폼이 환부와 접촉하는 접 촉 층, 발포 폴리우레탄으로 구성되어 흡수력을 극대화시
킨 흡수 층 그리고 그 밖을 싸고 있는 보호 층으로 구성되
었는데 메디폼-S는 흡수력을 높이기 위해 접촉 층을 없애고
흡수 층과 보호 층으로 구성되게 하였다. 접촉 층을 없앤
Fig. 7. Clinical cases (3rd degree burn wound), Scalding burn 6% TBSA, F/1. (A) post burn 3 day, (B) post burn 4 day, (C) post burn 8 day, (D) post burn 10 day, (E) post burn 11 day, (F) post burn 12 day, it shows eschar separation and skin graft was immediately performed.
대신 흡수 층에 존재하는 폴리우레탄 미세 구멍(pore)의 크 기를 50∼100 um 정도로 아주 작게 하여 상피세포가 가능 하면 미세 구멍 안으로 자라 들어가지 못하게 하였으며, 흡 수력은 극대화 하였다(1.2 g/1 cm
2). 따라서 접촉 층이 없지 만 메디폼-S는 상처에 붙지 않게 설계되었다(Fig. 2). 또한 silver sulfadiazine은 미세 구멍 안에 녹여넣어 흡수력에는 큰 지장을 주지 않게 하였다. 특별히 감염, 과민 반응과 같 은 부작용은 발생하지 않았으며, 피부 공여부 드레싱에서 는 아주 뛰어난 효과를 보여주었다(Fig. 3, 4). 상처드레싱에 서도 얇은 가피 정도는 쉽게 분리를 시킬 수 있었으며 특별 히 감염이 발생하지는 않았다(Fig. 5∼7). 본 예의 경우처럼 환자의 상태가 좋지 않아 피부 공여부에 염증이 생겼거나 치유가 지연된 경우에도 메디폼-S를 사용하면 100% 치유가 되었다. 또한 화상 부위에 사용한 경우 기존의 화상 연고로 치료한 경우보다 빠르고 미끈하게 치유시킬 수 있었다.
최근에 저자들은 2도 화상에서 재상피화 기간을 최대한 단축시키기 위해 메디폼에 상피세포성장인자(Easyef, 대웅 제약)를 같이 사용하고 있으며, 특히 소아화상에서 좋은 결 과를 경험하고 있다.
결 론
메디폼-S는 중증 화상 환자의 피부 공여부(감염될 가능성
이 많은)나 심재성 2도 화상 모두에서 첫 번째 드레싱으로 적당하다고 할 수 있겠다.
REFERENCES
1) Price RD, Das-Gupta V, Frame JD, Navsaria HA: A study to evaluate primary dressings for the application of cultured keratinocytes. Br J Plast Surg 54: 687-696, 2001
2) Persson K, Salemark L: How to dress donor sites of split thickness skin grafts: a prospective, randomised study of four dressings. Scand J Plast Reconstr Surg Hand Surg 34:
55-59, 2000
3) Banks V, Bale S, Harding K, Harding EF: Evaluation of a new polyurethane foam dressing. J Wound Care 6: 266-269, 1997
4) Weber RS, Hankins P, Limitone E, et al: Split-thickness skin graft donor site management. A randomized prospective trial comparing a hydrophilic polyurethane absorbent foam dressing with a petrolatum gauze dressing. Arch Otola- ryngol Head Neck Surg 121: 1145-9, 1995
5) Wells MD, Kirn DS: A new method of skin-graft stabili- zation: the Reston technique. Ann Plast Surg 34: 554-556, 1995
6) Salisbury RE, Bevin AG, Dingeldein GP, Grisham J: A clini- cal and laboratory evaluation of a polyurethane foam: a new donor site dressing. Arch Surg 114: 1188-92, 1979