서론
복부 패혈증은 복강 내 감염이나 후복막 감염의 결과로 발 생하며, 감염원인을 조기에 확인하여 적절한 치료가 지연되 지 않고 시행되는 것이 환자의 예후에 있어 매우 중요하다[1]. 정규시간 이후에 시행되는 복부 응급수술이 주로 복부 패혈 증과 관련되며, 수술 후 환자는 대부분 중환자실 치료를 요비외상성 복부 응급환자를 위한 급성치료수술
시스템 소개: 권역외상센터를 운영 중인 일개 대학
병원 자료분석
장 지 영1·심 홍 진1·김 재 훈2·홍 석 경3·배 금 석1 | 1연세대학교 원주의과대학 원주세브란스기독병원 권역외상센터, 2부산대학교 의 과대학 부산대학교병원 외상중환자외과, 3울산대학교 의과대학 서울아산병원 외상 및 중환자외과Current status of the Korean acute care surgery
system for non-traumatic abdominal emergency
surgery: a single-regional trauma center study
Ji Young Jang, MD1·Hongjin Shim, MD1·Jae Hun Kim, MD2·Suk-Kyung Hong, MD3·Keum Seok Bae, MD1
1Regional Trauma Center, Department of Surgery, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju; 2Department of Trauma Surgery, Pusan National University Hospital, Pusan National University School of Medicine, Busan; 3Division of Acute Care Surgery, Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Received: January 10, 2019 Accepted: February 8, 2019 Corresponding author: Keum Seok Bae
E-mail: [email protected]
Presented at the 37th Korean Society of Critical Care Medicine Annual
Congress, Seoul, Korea, 2018. © Korean Medical Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons. org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abdominal sepsis is mainly caused by intra-abdominal or retroperitoneal infection; therefore, early detection of the source of infection and adequate, prompt treatment are the most important contributors to patient outcomes. Because patients with sepsis often receive emergency abdominal surgery after regular hours, and most patients need critical care postoperatively, the need for personnel to specialize in these areas has emerged. The concept of acute care surgery (ACS), which includes trauma care, emergency general surgery, and surgical critical care, has been discussed since the early 2000s, and ACS fellowships were launched in the United States in 2008. ACS teams have been found to reduce mortality and complication rates, to decrease the time to surgery, and to lower financial costs in comparison to the traditional surgical model. In Korea, a regional trauma center project was started in 2012, and the government provided funding for each trauma center as part of this project. In the ACS field, the system for non-trauma emergency surgery is currently in the early stages of discussion. The need for such a system has been accelerated by the reduction of working hours per week of residents, as well as the shortage of manpower for emergency general surgery and surgical critical care on the night shift. In this review, we discuss the manpower problems that impact the treatment of abdominal emergency patients, and consider ways in which the Korean ACS system can treat these patients professionally.
하게 되므로 이러한 분야를 전문적으로 담당할 인력의 필요 성이 대두되어 왔다. 원가의 70% 정도로 낮은 보험수가와 전공의 주 80시간 근무제의 시행으로 인한 병원 내 진료인 력 부족과, 외과전문의들의 세부분과 전문진료화는 응급 중 환자의 치료를 적절히 시행하는데 어려움을 주고 있다. 이러 한 이유로 최근 국내에서 외과응급수술과 중환자 관리를 담 당하는 acute care surgery (ACS) 분과에 대한 관심이 높아 지고 있다. 이에, 저자는 복부 응급환자의 치료에서 발생하 는 인력적 문제점들에 대해 살펴보고, 이러한 환자들을 전문 적으로 치료하기 위한 한국형 ACS 시스템에 대하여 이야기 하고자 한다.
한국의 Acute Care Surgery의 현황
지난 십수 년 동안 외과의 세부전문화가 진행됨에 따라, 계 획수술, 비외상 응급수술, 외상수술을 모두 시행 가능한 일 반외과 의사의 수는 지속적으로 감소하였다. 이러한 변화에 따라 미국과 유럽의 여러 나라에서는 응급수술과 외상환자 치료를 전문적으로 담당할 분과로 ACS라는 개념이 2000년 대 초부터 논의되기 시작하였다[2,3]. 각 나라의 사회경제 적 여건과 외과의사의 수련과정이 다르기 때문에 조금씩 다 른 형태로 발전하였으나, 외과응급수술, 외상수술, 그리고 이러한 환자들의 외과중환자관리를 포함하는 것이 일반적 인 ACS의 영역으로 받아들여 지고 있다[2-6] (Figure 1).
미국에서는 미국외상학회(American Association for the Surgery of Trauma)를 중심으로 ACS 위원회가 구성되어 2008년부터 ACS 펠로우쉽 제도가 시작되었으며, 현재 21개 기관에서 ACS 프로그램이 운영되고 있다[7]. ACS 프로그램 에 대한 여러 연구들이 발표되고 있으며, 최근 한 체계적 문 헌고찰은 ACS 모델이 전통적인 외과 모델에 비해 사망률과 합병증 발생률을 낮추고, 수술까지의 시간과 재정적 비용을 감소시킨다고 보고하였다[8]. 최근 미국의 한 전국 연구에서 는 level 1 외상센터에서 운영되는 인증된 ACS 프로그램이, 그런 프로그램이 없는 외상센터나 비외상센터와 비교했을 때, 응급외과수술을 받은 환자의 재원기간, 합병증 발생률, 그리고 전체입원비용을 낮춘다고 보고하였다[9]. 국내에서는, 2011년 삼호주얼리호 피랍사건에서 총상을 입은 석해균 선장의 치료를 통해 국내 외상센터 도입의 필 요성이 공론화된 이후, 17개 병원이 권역외상센터 사업자로 선정되었으며 현재 12개 권역외상센터가 설립되어 운영되 고 있다[10]. 각 권역외상센터는 외상환자의 치료에 필요한 시설 및 장비를 위한 자금을 초기에 지원받았고, 외상전담 전문의들의 인건비를 정부로부터 지속적으로 지원받고 있 다. 외상사업단은 정기적인 센터 평가를 통해 외상센터의 질 증진과 예산지원을 차등화하고 있다. 권역외상센터 사업 을 통해 중증외상 환자의 신속하고 전문적인 치료가 가능하 게 되었고, 권역외상센터를 중심으로 각 권역 내의 외상 시 스템이 점차 구축되고 있다[11-13]. 특징적인 점으로는 한 외상센터당 23명까지, 외상전담 전문의의 인건비를 정부에 Figure 1. The concept of acute care surgery.
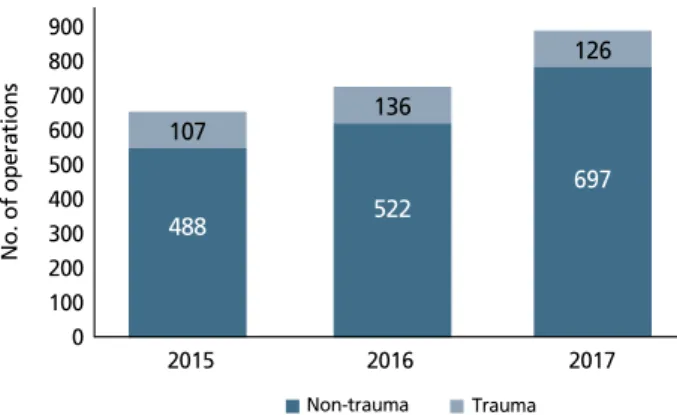
Trauma surgery Emergency surgery Surgical critical care Acute care surgery 900 800 700 600 500 400 300 200 100 0 2015 2016 2017 Non-trauma Trauma 107 488 136 522 126 697 No. of operations
Figure 2. Emergency abdominal operations at our center. Since the
establish-ment of the regional trauma center in 2015, there has been a slight increase in the number of abdominal trauma operations and a steep increase in the num-ber of non-trauma abdominal operations.
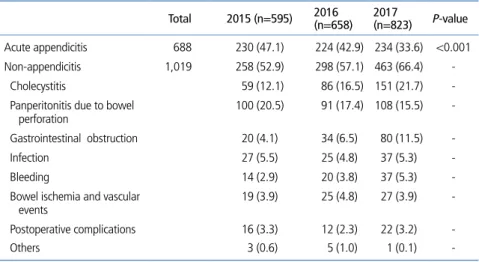
서 전액 지급하고 있다는 점이며, 이를 통하여 외상센터를 운영하는 병원들의 수익성을 보장하고 있다. 그러나 이러 한 지원을 받는 대신, 외상전담 전문의들이 외상환자 치료 를 위한 활동 외에 비외상 환자의 진료를 할 수 없도록 제 한하고 있다. 반면, ACS 분야 중 외상수술을 제외한 국내의 비외상 응 급수술에 대한 시스템은 논의가 시작되는 단계이다. 최근, 전공의의 주당근무시간을 80시간 이내로 제한하는 전공의 특별법이 시행되면서, 야간의 외과응급수술과 외과중환자관 리에 인력공백 증가는 이러한 논의를 가속화하고 있다. 실제 로 비외상 응급수술 분야는 이전부터 대부분의 외과가 있는 병원에서 야간 당직의 형태로 시행되고 있던 분야이나, 이에 대한 구체적인 통계 보고는 부족한 실정이다. 저자들의 병원은 삼차 대학병원으로, 2012년에 강원권 역 외상센터로 지정되었으며 2015년에 정식 운영을 시작하 였다. 본원의 응급수술 건수를 분석해 보면, 전체 외과 복부 응급수술은 2015년의 595건에서 2016 년 658건, 2017년 823건으로 지속적으 로 증가 추세에 있었고, 이중 비외상 응 급수술은 같은 기간 동안 2015년 488건 에서 2016년의 522건, 2017년의 697건 으로 가파른 증가를 보였다(Figure 2). 이를 수술종류별로 분석하였을 때, 급성 충수돌기염 수술은 약 230건으로 3년 간 일정한 건수를 보였으나, 비충수돌기 염 수술, 특히 급성담낭염과 위장관 폐 색 등의 수술이 큰 폭으로 증가한 것을 알 수 있었고(Table 1), 이렇게 증가된 수술을 외과의 5-7명의 외과전문의가 나누어 시행하였다. 이에 비해, 외상수 술 건수는 2015년 107건, 2016년 136 건, 2017년 126건으로 2016년에 증가 한 후 비슷한 건수가 유지되고 있다. 외 상환자의 치료에 있어 수술적 치료는 약 5-10%의 환자에서 시행되며, 외상 전 담전문의들은 주로 외상 중환자실에서 의 보존적 치료와 수술가능성이 있는 환자의 외과적 관찰을 주로 시행한다. 2015년 이후로 외상 전담전문의의 수가 증 가하면서, 전담의 한 명당 1년간 응급으로 집도한 복부외상 수술건수는 2017년에 약 20건 정도로 크게 감소한 것을 볼 수 있다(Table 2). 본원의 수술건수 통계를 통해 비외상 응 급수술을 수행하는 외과전문의들의 업무량은 그들의 계획수 술 건수를 고려할 때 과중함을 알 수 있었으며, 외상전담 외 과전문의들은 연간 적은 수술건수로 인해 수술술기의 유지 에 어려움이 있을 것으로 보인다. 미국의 미시간 대학 병원 의 연구에서도, 비외상 응급수술의 건수가 2008년의 575명 에서 2009년에 627명으로 증가하였고, 같은 기간 동안 118 명의 외상환자에서 개복 또는 개흉수술이 필요하였다는 결 과를 보여주었으며, 비외상 응급수술의 구성도 본원과 유사 한 패턴을 보였다. 이 연구의 저자들은 외상수술이 감소하 고 있는 환경에서 비외상 응급수술 서비스가 ACS 스텝들의 수술기술을 유지시키는데 도움이 되며 일반외과와 ACS 전 Table 1. The number of emergency abdominal operations at our center by year
Total 2015 (n=595) 2016 (n=658) 2017 (n=823) P-value Acute appendicitis 688 230 (47.1) 224 (42.9) 234 (33.6) <0.001 Non-appendicitis 1,019 258 (52.9) 298 (57.1) 463 (66.4) Cholecystitis 59 (12.1) 86 (16.5) 151 (21.7) Panperitonitis due to bowel
perforation 100 (20.5) 91 (17.4) 108 (15.5) Gastrointestinal obstruction 20 (4.1) 34 (6.5) 80 (11.5)
Infection 27 (5.5) 25 (4.8) 37 (5.3)
Bleeding 14 (2.9) 20 (3.8) 37 (5.3)
Bowel ischemia and vascular
events 19 (3.9) 25 (4.8) 27 (3.9)
Postoperative complications 16 (3.3) 12 (2.3) 22 (3.2)
Others 3 (0.6) 5 (1.0) 1 (0.1)
-The number of acute appendicitis operations remained roughly constant during the study period, but the number of non-appendicitis operations significantly increased. Values are presented as number (%).
Table 2. The number of trauma operations at our center
Surgeon A Surgeon B Surgeon C Surgeon D Surgeon E Surgeon F Surgeon G Total operations 2015 61 28 6 8 4 - - 107 2016 32 33 27 15 16 13 - 136 2017 24 19 25 24 26 5 3 126
The second operations after damage control surgery, surgery under local anesthesia, and tracheostomy were ex-cluded. As the number of trauma surgeons at our center has increased since 2015, the number of abdominal op-erations performed by each surgeon decreased to approximately 20 in 2017.
공의 트레이닝을 보조하는데도 도움이 된다고 하였다[14]. 현재 보건복지부의 지원 하에 외과 입원전담전문의 사업 의 일환으로 권역외상센터가 아닌 1개 대학병원에서 비외상 응급수술팀을 운영하고 있으며, 국내에서는 주로 외상수술 을 제외한 외과 응급수술과 외과 중환자관리를 묶어서 ACS 로 정의 명명하고 있다. 국내의 한 연구에서 복부 응급수술 을 받은 이차성 복막염 환자의 사망률을 11.2%로 보고 하 였으며, 또 다른 연구에서는 복부 응급수술 후 패혈증이 있 는 경우에 26.3%의 사망률을 보고하였다[15,16]. 복부패혈 증의 치료에 있어 가장 중요한 요소는 원인제거를 위한 수술 이 지연되지 않고 적절하게 시행되는 것과 수술 후 중환자 실에서 패혈증에 대한 치료가 적절하게 이루어지는 것이다 [1]. 이를 위해 응급수술에 대한 충분한 경험을 갖춘 전담의 사의 원내 당직이 필수적인데, 이러한 인력양성을 위한 적절 한 교육이 필요하며 인력운영을 위한 재원이 필요하다. 또한 응급실에서의 초기진단과 수술, 그리고 중환자실 입원이 지 연되지 않기 위한 수술실과 중환자실 등의 시설이 상시 구비 되어야 하나 계획수술이 삼차 대학병원으로 집중되는 국내 의 상황에서는 수술실이나 외과계 중환자실을 이러한 환자 들을 위해 비워놓는 것이 현실적으로 어렵다. 국내 의료체계 하에서 삼차의료기관에서 이러한 비외상 응급수술 시스템의 운영은 병원의 수익성을 악화시키기 때문에 최소한의 인력 으로 운영되고 있으며, 이차 의료기관에서는 환자의 수술 후 관리에 어려움이 있기 때문에 운영에 소극적일 수밖에 없다. 이러한 현실을 고려할 때, 비외상 응급수술 시스템도 외상 시스템과 같은 사회안전망으로서 국가재원 투입이 고려되어 야 할 것이다. 또한, 국내 외상 시스템이 어느 정도 체계화되 고 완성된 시점에는, 외상환자 진료에 지장을 주지 않는 선 에서 외상전담전문의가 비외상 응급수술을 제한된 범위에서 시행할 수 있도록 허용하는 것에 대한 논의도 가능할 것으로 보인다. 이것은 기존 외상전담전문의들의 술기를 유지하는 데 도움이 될 것이며 신규 수련 중인 외상 전임의들의 교육 에도 도움이 될 것이다[14]. 또한, ACS 분야의 부족한 인력 을 운영하는데 있어 인력배치의 유연성을 높일 수 있을 것이 므로, 결과적으로는 병원들의 ACS팀 운영을 촉진하게 될 것 이다. 이러한 노력들을 통해 외상 시스템에 비해 상대적으로 열악한 국내 비외상 응급수술 분야의 발전을 촉진시킬 것이 며, 결과적으로 국내 ACS 시스템의 성공적인 확립은 또 하 나의 사회안전망으로 기능할 것으로 기대된다.
결론
본 기고는 권역외상센터를 운영중인 일개 대학병원의 자 료만을 분석하였기 때문에 국내 전체의 상황을 대변하기는 어렵다는 제한점이 있으나, ACS 시스템의 태동기인 현 시점 에서 이에 대한 국내 연구는 전무하며 또한 권역외상센터의 외상전담 외과전문의의 수술건수에 대한 문헌이 부족한 상 황에서 어느 정도 의미를 가진다고 생각된다. 추후 국내 권 역외상센터들을 대상으로 한 다기관 연구를 통해 본 주제에 대한 확인이 필요할 것으로 보인다. 찾아보기말: 외과; 응급; 급성복증; 패혈증; 복부손상 ORCIDJi Young Jang, https://orcid.org/0000-0001-6372-4194 Hongjin Shim, https://orcid.org/0000-0003-3073-3806 Jae Hun Kim, https://orcid.org/0000-0002-8704-0579 Suk-Kyung Hong, https://orcid.org/0000-0001-5698-0122 Keum Seok Bae, https://orcid.org/0000-0003-4728-3047
REFERENCES
1. Sartelli M, Viale P, Catena F, Ansaloni L, Moore E, Malangoni M, Moore FA, Velmahos G, Coimbra R, Ivatury R, Peitzman A, Koike K, Leppaniemi A, Biffl W, Burlew CC, Balogh ZJ, Boffard K, Bendinelli C, Gupta S, Kluger Y, Agresta F, Di Saverio S, Wani I, Escalona A, Ordonez C, Fraga GP, Junior GA, Bala M, Cui Y, Marwah S, Sakakushev B, Kong V, Naidoo N, Ahmed A, Abbas A, Guercioni G, Vettoretto N, Díaz-Nieto R, Gerych I, Tranà C, Faro MP, Yuan KC, Kok KY, Mefire AC, Lee JG, Hong SK, Ghnnam W, Siribumrungwong B, Sato N, Murata K, Irahara T, Coccolini F, Segovia Lohse HA, Verni A, Shoko T. 2013 WSES guidelines for management of intra-abdominal infections. World J Emerg Surg 2013;8:3.
2. Hoyt DB, Kim HD, Barrios C. Acute care surgery: a new train-ing and practice model in the United States. World J Surg 2008;32:1630-1635.
3. Uranues S, Lamont E. Acute care surgery: the European model. World J Surg 2008;32:1605-1612.
4. Goslings JC, Ponsen KJ, Luitse JS, Jurkovich GJ. Trauma surgery in the era of nonoperative management: the Dutch model. J Trauma 2006;61:111-114.
5. Handolin L, Leppaniemi A, Vihtonen K, Lakovaara M, Lin-dahl J. Finnish Trauma Audit 2004: current state of trauma management in Finnish hospitals. Injury 2006;37:622-625. 6. Goosen J, Veller M. Trauma and emergency surgery: South
African model. World J Surg 2008;32:1622-1625.
7. American Association for the Surgery of Trauma. Acute care surgery [Internet]. Chicago: American Association for the Surgery of Trauma; 2014 [cited 2019 Jan 29]. Available from: http://www.aast.org/AcuteCareSurgery.aspx.
8. Chana P, Burns EM, Arora S, Darzi AW, Faiz OD. A syste-matic review of the impact of dedicated emergency surgical services on patient outcomes. Ann Surg 2016;263:20-27. 9. Khalil M, Pandit V, Rhee P, Kulvatunyou N, Orouji T, Tang
A, O'Keeffe T, Gries L, Vercruysse G, Friese RS, Joseph B. Certified acute care surgery programs improve outcomes in patients undergoing emergency surgery: a nationwide analy-sis. J Trauma Acute Care Surg 2015;79:60-63.
10. Park DJ, Park CY, Cho HM, Lee KH, Han HS. Current status and future prospects of trauma centers in Korea. J Korean Med Assoc 2017;60:530-532.
11. Jang JY, Shim H, Kwon HY, Chung H, Jung PY, Kim S, Ryu
H, Bae KS. Improvement of outcomes in patients with pelvic fractures and hemodynamic instability after the establishment of a Korean regional trauma center. Eur J Trauma Emerg Surg 2017 Dec 27 [Epub]. https://doi.org/10.1007/s00068-017-0886-3.
12. Jung K, Matsumoto S, Smith A, Hwang K, Lee JC, Coimbra R. Comparison of outcomes in severely injured patients between a South Korean trauma center and matched patients treated in the United States. Surgery 2018;164:482-488.
13. Kim OH, Roh YI, Kim HI, Cha YS, Cha KC, Kim H, Hwang SO, Lee KH. Reduced mortality in severely injured patients using hospital-based helicopter emergency medical services in interhospital transport. J Korean Med Sci 2017;32:1187-1194. 14. Cherry-Bukowiec JR, Miller BS, Doherty GM, Brunsvold
ME, Hemmila MR, Park PK, Raghavendran K, Sihler KC, Wahl WL, Wang SC, Napolitano LM. Nontrauma emergency surgery: optimal case mix for general surgery and acute care surgery training. J Trauma 2011;71:1422-1426.
15. Jang JY, Lee SH, Shim H, Choi JY, Yong D, Lee JG. Epide-miology and microbiology of secondary peritonitis caused by viscus perforation: a single-center retrospective study. Surg Infect (Larchmt) 2015;16:436-442.
16. Kim JW, Park JH, Kim DJ, Choi WH, Cheong JC, Kim JY. The delta neutrophil index is a prognostic factor for postoperative mortality in patients with sepsis caused by peritonitis. PLoS One 2017;12:e0182325.