Arthroscopic treatment of heterotopic ossification of the hip after hip arthroscopy
Jung-Mo Hwang
1, Deuk-Soo Hwang
2, Chan Kang
2, Byung-Kon Shin
21Department of Orthopaedic Surgery, Soonchunhyang University College of Medicine, Gumi, 2Department of Orthopaedic Surgery, Chungnam National University School of Medicine, Daejeon, Korea
INTRODUCTION
Arthroscopic treatment of the hip is regarded in large as a safe, effective, and usually complicationfree procedure [1]. However, recent developments in surgical techniques and tools that now expand to treat lesions of the soft tissue and the bone as well as the hip have unexpectedly led to increases in the occurrence of complications [2].
Heterotopic ossification is one example of the reportedly increased complications. In heterotopic ossification is a reactive disease where mature lamellar bone forms in the soft tissue. It usually occurs as a complication after open trauma or arthroplasty of the hip. It has been shown after open reduction or total hip arthroplasty of the acetabular fracture, the occurrence of heterotopic ossification ranges between 5% to 90% [3,4], and after hip arthroscopy the occurrence is between 1.0% to 6.3% [1,2,5]. The diagnosis of heterotopic ossification is accidental through radiograph analyses are taken for other purposes, because in most cases the heterotopic ossification is asymptomatic [3,6]. Mild symptoms of heterotopic ossification such as articular disability, joint stiffness, pain, and crepitation have been reported in some cases, but reports of severe
symptoms such as ankylosis are uncommon [7]. Here the authors report pain and limitations in normal walking in a patient who developed heterotopic ossification after arthroscopic treatment of femoroacetabular impingement of the hip.
CASE REPORT
A previous amateur soccer player, now serving in the military service, complained of worsen pain in the right inguinal region and deteriorated disability in activity.
The 20yearold male has a history of femoroacetabular impingement, labral tear, and internal snapping hip that were treated through arthroscopic labral refixation, femoroplasty, and iliopsoas tenotomy 35 months earlier (Fig. 1). Although the postoperative pain in the inguinal region was improved after surgery, at the 4th postoperative month when the patient returned to sports activity, the pain began to worsen up to a visual analogue scale (VAS) of pain of 8 points and a modified harris hip score (mHHS) of 62 points last month. Even light daily activities induce discomfort and pain. Physiological tests such as the anterior impingement test (Flexion, ADduction, Internal Heterotopic ossification is a reactive disease where mature lamellar bone forms in the soft tissue. It usually occurs as a complication after open trauma or arthroplasty of the hip. In rare cases, it even occurs after hip arthroscopy with an occurrence rate of 1.0% to 6.3%. Here, the authors report a case of an arthroscopic removal of heterotopic ossification that had caused pain and limitation in daily activities. Heterotopic ossification was a postoperative complication after arthroscopic treatment of a femoroacetabular impingement combined with an internal snapping hip.
Keywords: Hip; Heterotopic ossification; Arthroscopy
Copyright © 2014 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received December 9, 2013; Revised March 13, 2014; Accepted March 20, 2014
Correspondence to: Deuk-Soo Hwang, Department of Orthopaedic Surgery, Chungnam National University Hospital, 282 Munhwa- ro, Jung-gu, Daejeon 301-721, Korea. Tel: +82-42-280-7350, Fax: +82-42-252-7098, E-mail: dshwang@cnu.ac.kr
Arthroscopy and Orthopedic Sports Medicine
AOSM
Fig. 1. Plain radiograph prior to hip arthroscopy. Heterotopic ossification cannot be seen in preoperative (A) and postoperative (B) Xrays.
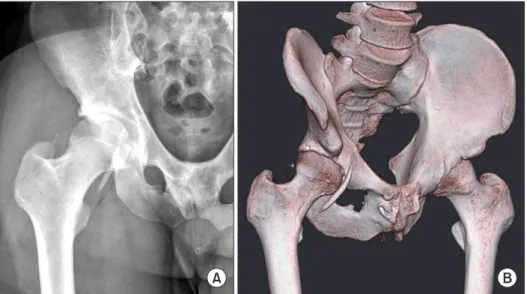
Fig. 2. Preoprerative plain radiography (A) and threedimentional computed tomography scan (B) show Brooker grade II heterotopic ossification.
Fig. 3. (A) During arthroscopic surgery, the exact location of the heterotopic ossification was confirmed by Carm.
(B, C) The heterotopic ossification was removed using a radiofrequency probe and a grasper. (D) Gross photo shows the removed heterotopic ossification.
Rotation [FADIR] test) and the Patrick test (Flexion, ABduction, Exernal Rotation [FABER] test) are positive, despite the range of motion of the hip being normal. Plain radiographs and computed tomography showed presence of bony islands around the anterior capsule (×2) and the iliopsoas attachment site (×1), therefore classifying the patient’s heterotopic ossification into Brooker’s grade II, a classification system for heterotopic ossification (Fig. 2) [8].
The patient was placed in a supine position on the fracture table under general anesthesia. The surgery to remove the heterotopic ossification was performed using the anterolateral portal and the anterior portal techniques.
The position of the heterotopic ossification was identified using Carm intensifier, and then radiofrequency and a shaver was used to desquamate the ossification from the soft tissue and lastly, a burr and grasper was used for the removal (Fig. 3). We chose to arthroscopically remove the heterotopic ossification by fragmenting the bone using the burr and then using a grasper to remove the fragments as the size of the ossification was large. The 2 bony islands in the anterior capsule was largely removed, however, a bony island at the iliopsoas attachment site was not, as this was situated near the femoral artery and nerve, as any perturbation may induce greater pain in the patient (Fig. 4). Total duration of the surgery was 140 minutes, and no postoperative complication existed. On the next day, radiotherapy (10 Gy) and indomethacin prescription (100 mg/day, for 6 weeks) were commenced, as well as pendulum and weightbearing exercises of the hip.
The patient was released after a week postsurgery when radiotherapy was completed, and at release, the patient’s
VAS score decreased to 4 points.
At oneyear followup, the patient showed restored ability to execute daily activities and light exercise without any discomfort. Other than a slight pain of the inguinal region when climbing a steep slope, the patient did not make any complaints of pain. The VAS score improved to 1 point, and similarly the mHHS improved to 96 points.
Plain radiographs followup was negative for a recurrence (Fig. 5).
DISCUSSION
Heterotopic ossification occurs after hip surgery, spinal Fig. 4. Postoperative plain radiograph (A) and threedimensional computed tomo
graphy scan (B) show a near complete removal of heterotopic ossification.
Fig. 5. Plain radiograph at 12 months postoperation shows no evidence of recurrence.
nerve injury, burns, head trauma, and fractures etc. Risk factors include sex (male), a past history of heterotopic ossification, ankylosing spondylitis, obesity, oldage, and arthritis [3,9]. The occurrence of heterotopic ossification is highest after open reduction or hip arthroplasty of acetabular fractures, the likelihood of developing the ossification being 5%-90% [3,4]. In comparison, the likelihood of developing heterotopic ossification after open reduction of femoroacetabular impingement is around 37% according to Ganz et al. [10], the most common site of development being the tip of the greater trochanteric. And according to recent reports by several clinicians, the incidence of heterotopic ossification is around 1.0%-6.3% greater after hip arthroscopy than in the shoulder or elbow arthroscopy [1,2,5]. The reason why the incidence of heterotopic ossification after arthroscopic treatment of femoroacetabular impingement over the open approach is lower is thought to be because of the continual irrigation by detergents during the surgical process in the arthroscopic approach.
This continual irrigation may remove the known precursor of heterotopic ossification, hematoma and bone fragments surrounding the joints [9]. However, despite this, the reason why after hip arthroscopy the incidence of heterotopic ossification is greater than in arthroscopy in any other joints is suggested by McCarthy et al. [11] to be differences in the surgical process such as having relatively more osteotomy, inaccessibility of the joint, structural differences, and muscle coverage. In our 10 years of experience in arthroscopic treatment of over 400 cases of femoroacetabular impingement, we describe our first experience of heterotopic ossification associated with pain and limitation in daily activities.
Symptoms of heterotopic ossification include articular disability, stiffness, pain, and crepitation, but in most cases, it forms asymptomatically. Moreover, in around 64%
the ectopic ossification is a selflimited naturally retracting entity that does not require surgical intervention [12].
Nevertheless, if persistent pain or limitation in articular activity is seen, then it is important to suspect an ectopic ossification. Pain from the ectopic ossification is induced during hip flexion, adduction, and internal rotation if the ossification is located in the hip articular capsule, the rectus femoris, or the anterior iliopsoas. Conversely, pain is induced during external rotation if the ossification is located in the lateral hip. The current case report shows through radiographs that the heterotopic ossification is located anterior to the iliopsoas and anterolateral to the capsule, and physiological examination indeed shows severe pain is induced during hip flexion, adduction, and internal rotation.
Prophylactic treatment includes taking nonsteroidal antiinflammatory drugs and periodic radiological tests.
Bedi et al. [2] found that taking indomethacin after hip arthroscopy is effective in preventing heterotopic ossification, its effectiveness showing especially in males who received osteoplasty. However, the prophylactic ability of radiotherapy against heterotopic ossification after hip arthroscopy is unknown, but this has been shown for artificial arthroplasty of the hip and open reduction of acetabular fracture [13,14]. In this report, the authors performed arthroscopic removal of the ectopic bone in patients with severe pain or limitation in daily activities.
To prevent a recurrent ossification, indomethacin prescription and radiotherapy was given to the patient in parallel. In summary, complication of heterotopic ossification can occur even after arthroscopic treatment of the hip, and thus in highrisk groups, prophylactic measures to prevent formation of heterotopic ossification subsequent to arthroscopic treatment should be taken.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
1. Ilizaliturri VM Jr. Complications of arthroscopic femoroacetabular impingement treatment: a review. Clin Orthop Relat Res 2009;467:760-8.
2. Bedi A, Zbeda RM, Bueno VF, Downie B, Dolan M, Kelly BT. The incidence of heterotopic ossification after hip arthroscopy. Am J Sports Med 2012;40:854-63.
3. Board TN, Karva A, Board RE, Gambhir AK, Porter ML. The
prophylaxis and treatment of heterotopic ossification following lower limb arthroplasty. J Bone Joint Surg Br 2007;89:434-40.
4. Karunakar MA, Sen A, Bosse MJ, Sims SH, Goulet JA, Kellam JF.
Indometacin as prophylaxis for heterotopic ossification after the operative treatment of fractures of the acetabulum. J Bone Joint Surg Br 2006;88:1613-7.
5. Randelli F, Pierannunzii L, Banci L, Ragone V, Aliprandi A, Buly
REFERENCES
R. Heterotopic ossifications after arthroscopic management of femoroacetabular impingement: the role of NSAID prophylaxis. J Orthop Traumatol 2010;11:245-50.
6. Fransen M, Neal B. Non-steroidal anti-inflammatory drugs for preventing heterotopic bone formation after hip arthroplasty.
Cochrane Database Syst Rev 2004;(3):CD001160.
7. Iorio R, Healy WL. Heterotopic ossification after hip and knee arthroplasty: risk factors, prevention, and treatment. J Am Acad Orthop Surg 2002;10:409-16.
8. Brooker AF, Bowerman JW, Robinson RA, Riley LH Jr. Ectopic ossification following total hip replacement. Incidence and a method of classification. J Bone Joint Surg Am 1973;55:1629- 32.
9. Bal BS, Lowe JA, E Gietler A, Aleto TJ. Heterotopic ossification after 2-incision total hip arthroplasty. J Arthroplasty 2010;25:538- 40.
10. Ganz R, Gill TJ, Gautier E, Ganz K, Krügel N, Berlemann U.
Surgical dislocation of the adult hip a technique with full access
to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-24.
11. McCarthy JC, Puri L, Lee JA, et al. Pathology amenable to arthroscopy of the hip. In: McGinty JB, Burkhart SS, Jackson RW, et al., editors. Operative arthroscopy. Philadelphia, PA: Lippincott Williams & Wilkins; 2003. p.866.
12. Toyoda T, Matsumoto H, Tsuji T, Kinouchi J, Fujikawa K. Hetero- topic ossification after total knee arthroplasty. J Arthroplasty 2003;18:760-4.
13. Burd TA, Lowry KJ, Anglen JO. Indomethacin compared with localized irradiation for the prevention of heterotopic ossification following surgical treatment of acetabular fractures. J Bone Joint Surg Am 2001;83:1783-8.
14. Kienapfel H, Koller M, Wüst A, et al. Prevention of heterotopic bone formation after total hip arthroplasty: a prospective randomised study comparing postoperative radiation therapy with indomethacin medication. Arch Orthop Trauma Surg 1999;119:296-302.