비판막성 심방세동 환자에서의 항응고 치료의 최신 요법
국민건강보험 일산병원 심장내과
양주영
Current Antithrombotic Therapy for Patients with Nonvalvular Atrial Fibrillation
Joo Young Yang
Department of Internal Medicine, National Health Insurance Service Ilsan Hospital, Goyang, Korea
In patients with nonvalvular atrial fibrillation (AF), the risk of stroke varies considerably according to individual clinical status.
The CHA2DS2-VASc score is better than the CHADS2 score for identifying truly lower risk patients with AF.
With the advent of novel oral anticoagulants (NOACs), the strategy for antithrombotic therapy has undergone significant changes due to its superior efficacy, safety and convenience compared with warfarin.
Furthermore, new aspects of antithrombotic therapy and risk assessment of stroke have been revealed: the efficacy of stroke prevention with aspirin is weak, while the risk of major bleeding is not significantly different from that of oral anticoagulant (OAC) therapy, especially in the elderly. Reflecting these pivotal aspects, previous guidelines have been updated in recent years by overseas societies and associations. This author has summarized the new evidence and updated recommendations for stroke prevention of patients with nonvalvular AF. First of all, antithrombotic therapy must be considered carefully and incorporate the clinical characteristics and circumstances of each individual patient, especially with regards to balancing the benefits of stroke prevention with the risk of bleeding, recommending the CHA2DS2-VASc score rather than the CHA2DS2 score for assessing the risk of stroke, and employing the HAS-BLED score to validate bleeding risk. In patients with truly low risk (lone AF, CHA2DS2-VASc score of 0), no antithrombotic therapy is recommended, whereas OAC therapy, including warfarin (international normalized ratio 2-3) or NOACs, is recommended for patients with a CHA2DS2-VASc score ≥2 unless contraindicated. In patients with a CHA2DS2- VASc score of 1, OAC therapy should be preferentially considered, but depending on bleeding risk or patient preferences, antiplatelet therapy or no therapy could be permitted.
Key Words: Nonvalvular atrial fibrillation, Oral anticoagulant, Antithrombotic therapy
책임저자 : 양주영
10444 경기도 고양시 일산동구 일산로 100 국민건강보험 일산병원 심장내과 전화 : (031)900-0630, 팩스 : (031)900-0343 E-mail : jooyy@nhimc.or.kr
서 론
심방세동(AF)은 선진국에서 일반 인구의 대략 1.5-2%의 빈도로 발견되며, 나이에 따라 점차 증가하는 경향을 보여, 80세 이상 인구의 약 10%로 추산된다. AF는 뇌졸중이 5배, 심부전증이 3배의 위험도를 가지고 있으며, 높은 사망률을 가진다.1 특히 심방세동 환자는 뇌졸중 발현시 좀더 넓은 범위 를 침범하는 경향이 있어 다른 원인에 의한 뇌졸중보다 심한
신경학인 장애를 초래한다. 여기에 AF에 대한 항응고 치료의 중요성이 강조되어 왔다.2
2003년부터 AF 환자에서 뇌졸중예방에 대한 new oral anti- coagulants (NOACs)의 효능성과 안전성에 대하여 중요한 논문 이 지속적으로 발표되었다. aspirin, clopidogrel 또는 warfarin 과 같은 전통적인 항응고제와는 달리 NOACs는 두 개의 군으 로 나눠지는 다른 작용기전을 가지며, 두 군은 다음과 같다:
1) Oral direct thrombin inhibitor (ximelagatran, dabigatran), 2) Oral direct factor Xa inhibitor (rivaroxaban, apixaban, edo-
xaban).3-8
Ximelagatran은 제일 먼저 개발되었으나, 연구 중반 심한 간독성으로 퇴출되었고, 다른 NOACs은 warfarin에 비하여 뇌졸중예방, 뇌 내출혈(intracranial hemorrhage: ICH), 사망
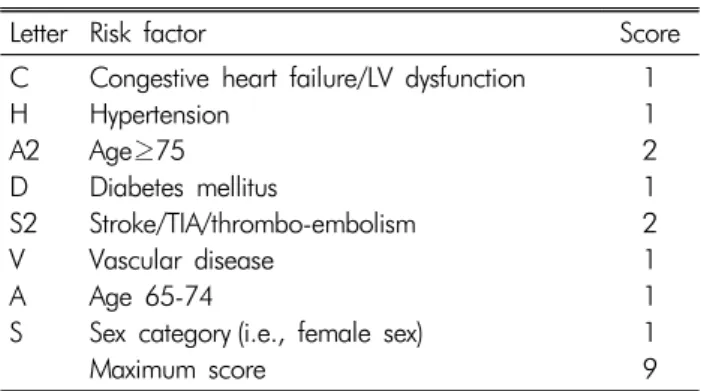
Table 1. The CHA2DS2-VASc score
Letter Risk factor Score
C H A2 D S2 V A S
Congestive heart failure/LV dysfunction Hypertension
Age≥75 Diabetes mellitus
Stroke/TIA/thrombo-embolism Vascular disease
Age 65-74
Sex category (i.e., female sex) Maximum score
1 1 2 1 2 1 1 1 9 률면에서 비열등성이거나 월등한 감소를 보여 지속적으로 연
구되었다. 이러한 결과로 NOACs은 2010년도부터 아시아, 서구의료계에서 갱신된 권고사항으로 비판막성 심방세동의 항응고 치료로 권고되었다.
이에 본 저자는 아시아, 유럽, 북미의료계에서 최근에 제기 된 개정된 권고사항을 중심으로 비판막성 심방세동 환자의 뇌졸중 예방에 대한 갱신된 권고사항을 제공코자 한다.
한국에서는 비판막성 심방세동의 뇌졸중 예방에 대한 임 상적인 권고사항이 2009년도에 발표되었으며, 그 권고사항 의 요약은 다음과 같다.9
1) 항응고치료(warfarin 또는 aspirin)은 비판막성 심방세동 환자에서 뇌졸중의 예방을 위하여 권고하며, 이때 뇌졸 중위험도, 출혈위험도, 환자의 선호도, 높은 수준의 항 응고 감시 장치의 접근성이 고려되야 한다.
2) Warfarin (INR 2-3)이 고위험군 환자(연간 뇌졸중 위험 도 4%)에서 그리고 중등도 위험군의 대부분 환자에서 권고된다. 단 경구용 항응고제(OAC)에 임상적으로 심 각한 비적응증이 없어야 한다.
3) Randomized studies가 없지만, 75세가 넘는 환자에서는 심방세동에서 뇌졸중을 예방하기 위해 warfarin (INR 2-3)이 사용될 수도 있다.
그러므로 비판막성 심방세동 환자에서 NOACs의 탁월한 항응고 효과 덕분과 해외의 권고사항의 갱신덕분에 2012년 도에 한국에서도 갱신하는 것에 대한 문제가 제기되었다. 그 러나, 실제 임상에서 aspirin이 뇌졸중의 저위험군에서 선호 되고, 고위험군이 아닌 비판막성 심방세동환자(단독의 심방 세동, CHA2DS2-VASc score가 0)에서 항응고 치료가 얻는 이 득이 없음에도 과사용되었다. 반면에 warfarin (oral vitamin K antagonist)이 aspirin이나 clopidogrel같은 항혈소판제제에 비 하여 뇌졸중예방에 뛰어난 효능이 있음에도 불구하고 자주 INR를 검사하는 불편, 심각한 출혈부작용, 병용하는 약제, 음식, 한약과의 상호작용으로 인하여 warfarin이 부적절하게 적게 사용되었다.
1. 최근에 갱신된 해외의 권유사항과 증거
CHADS2 score는 오랫동안 심방세동 환자에서 뇌졸중의 위험도 측정에 사용되어왔다.
뇌졸중 위험인자에 1점씩 부여했는데 이는 다음과 같다;
즉, 심부전, 고혈압, 나이(75세 이상), 당뇨는 1점, 뇌졸중 이나 TIA는 2점이 주어졌다.
그러나, 항응고 치료가 필요치 않은 “진정한 환자”(CHADS2
score가 0)를 구별하는데 제한 점이 있었다. 이러한 문제를 극 복하기 위하여 유럽심장학회(ESC) 2010 권고안은 CHA2DS2- VASc score를 제안하였는바 이는 나이(75세 이상 2점, 65-74 세 1점), 성별(여성 1점), 혈관질환(1점)(Table 1)10의 추가적 인 점수를 주었다. 그래서, 캐나다심장학회(CCS) AF 2012 권고 안, APHRS 2013 권고안, AHA/ACC/Heart Rhythm Society (HRS) 2014 권고안 모두 뇌졸중의 위험을 평가하는데, CHADS2
score 보다는 CHA2DS2-VASc score를 사용키로 갱신하였
다.11-13 그러나, 위험인자가 전무한 여성 환자에서 항응고 치
료는 권고되지 않았다.
전의 권고사항에는 CHADS2 1점이 항응고 치료하는 결정 요소였으나, 증거가 쌓임에 따라 심방세동 환자에서 CHA2DS2- VASc score가 “truly low risk” 환자를 구별해 내는데 유용하 므로 뇌졸중이나 혈전이 생길 환자를 예측하는데 CHADS2
score보다 나은 것으로 생각된다.14
그래서 한국에서도 저위험군 환자에서 불필요한 항응고 치 료를 피하고, 심방세동 환자에서 좀더 정확한 뇌졸중의 위험도 를 예측하기 위하여 CHA2DS2-VASc score를 적용해야 한다고 생각되었다. 뇌졸중예방을 위한 항응고 치료는 뇌졸중의 위험 성과 가장 위험한 합병증인 ICH같은 심각한 출혈, 2 pints의 이상 수혈을 요하는 심한 출혈과의 형평이 고려되야만 한다.
일반적으로 출혈의 위험성은 다음과 같은 순서로 항응고 치료에 비례하여 증가된다; (1) aspirin (75-325 mg/day) 또는 clopidogrel (75 mg/day), (2) asprin과 clopidorel의 병합치료, (3) 저용량의 dabigatran (110 mg bid), (4) 고용량의 dabigatran (150 mg bid), ribaroxaban, apixaban 그리고 warfarin (INR 2-3)이 비슷한 위험도를 가진다.11
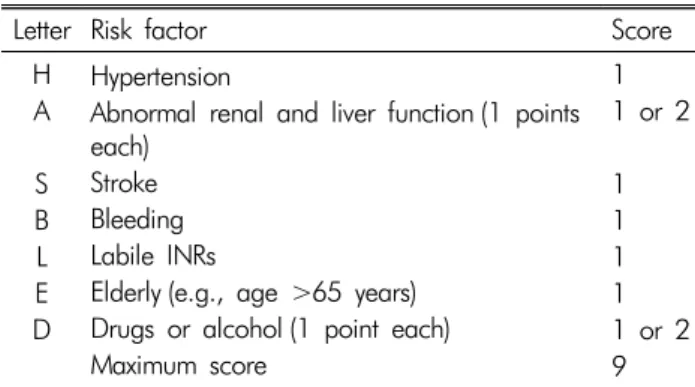
ESC 2010 과 CCS AF 2012 권고안 모두 실제 임상에서 출혈위험도를 평가하는데, HAS-BLED bleeding risk score를 사용토록 권하고 있다(Table 2). HAS-BLED bleeding risk score는 다음과 같은 것들을 출혈위험군으로 생각하고 있은
Table 2. The HAS-BLED bleeding risk score
Letter Risk factor Score
H A S B L E D
Hypertension
Abnormal renal and liver function (1 points each)
Stroke Bleeding Labile INRs
Elderly (e.g., age >65 years) Drugs or alcohol (1 point each) Maximum score
1 1 or 2 1 1 1 1 1 or 2 9
데, 고혈압, 신장/간장 기능 이상, 뇌졸중, 출혈의 과거력이나 경향, INR이 labile한 경우, 고령층(65세 이상), 약물/알코올 이 점수 체계에 따르면 HAS-BLED score가 0-1인 경우 연간 출혈위험도가 약 1%, score가 5인 경우 위험도가 연간 약 12.5% 된다고 하였다.15
HAS-BLED score가 3인 환자에서 심각한 출혈의 위험도는 약 3.74%이며, 심방세동 환자의 고위험도와 일치한다. 그래 서, 출혈합병증을 최소화하기 위하여 철저한 주의와 정기적 인 검토가 필요하며, HAS-BLED score가 3 이상인 환자에서 출혈을 줄이기 위해 가역적인 위험인자를 줄이기 위한 노력 을 기울여야 한다. 높은 HAS-BLED score 자체로 인하여 OAC 치료를 배제해서는 안된다. NOACs은 INR monitoring 없이 도 치료 효과가 예측되기 때문에 labile INRs 환자에 추천되 고, 또한 음식이나 약물에 상호작용이 없기 때문이다. 고혈압, 뇌졸중의 과거력이나 TIA, 고령이 뇌졸중의 위험인자가 출혈 합병증의 위험인자가 된다. 실제 임상에서 출혈의 위험성이 CHA2DS2-VASc score의 증가에 따라 비례적으로 증폭된다.
2. New Oral anticoagulants을 이용한 중요한 임상 실험 1) Dabigatran 대 Warfarin: The Randomized Evaluation
of Long-Term Anticoagulation (RE-LY)4
RE-LY 연구는 전향적이고 무작위적이고 개방표지 시험이 고 3상 임상실험으로 warfarin (INR 2-3)과 dabigatran 두 용량 (110 mg bid :D110 또는 150 mg bid: D150)을 비교한 임상 연구로 primary outcome은 뇌졸중 또는 전신 혈전으로 하였다.
Primary outcome rates은 warfarin군에서 1년에 1.69% 이 었고, 이에 비해 D110군은 1년에 1.53% {상대위험도(RR), 0.91; 95% CI, 0.74 to 1.11; p<0.001 for 비열등성} 그리고 D150군은 1년에 1.11% {RR, 0.66; 95% confidence interval (CI), 0.53 to 0.82; p<0.001 for superiority}였다. 심각한 출
혈의 발생빈도는 warfarin군은 1년에 3.36%였고, 이에 비해 D110군은 2.71%(p=0.003)였고, D150군은 3.11%(p=0.31) 였다.
출혈성 뇌졸중의 발생빈도는 warfarin군에서 1년에 0.38%
였으며, 이에 비해 D110군은 1년에 0.12% (p<0.001) 그리고 D150군은 1년에 0.10% (p<0.001)였다. 사망률은 warfarin 군은 1년에 4.13% 였고, 이에 비해 D110군은 1년에 3.75%
(p=0.13) 그리고 D150군은 1년에 3.64% (p=0.051)였다. 출 혈성 뇌졸중과 ICH은 dabigatran 양군에서 낮게 나타났으나, 위장관계 출혈은 D150군에서 의미있게 높았다.
심방세동의 환자에서 warfarin과 관계있는 뇌졸중과 전신 혈전이 D110군과도 관련이 있고, 심각한 출혈의 저빈도와 관 계 있었고, D150군은 warfarin에 비해 뇌졸중과 전신 혈전의 저빈도와 관계가 있고, 심각한 출혈은 비슷한 빈도를 보였다.
2) Rivaroxaban versus Warfarin: Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for the Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET AF)5
ROCKET AF는 임상 연구로 randomized, double-blind and double-dummy trial로서 rivaroxaban 매일 20 mg (creatinine clearance 30-49 mL/min이면 매일 15 mg), 또는 뇌졸중의 발 생위험이 높은 비판막성 심방세동 환자에서 적절히 용량조절 된 warfarin과 비교하였다. Primary end point는 뇌졸중 또는 전신 혈전으로 하였고, rivaroxaban군은 188명(1년에 1.7%) 이 발생하였고, warfarin군은 241명(1년에 2.2%)이 발생되었 다{hazard ratio (HR), 0.79; 95% CI, 0.66 to 0.96; p<0.001 for noninferiority}. Intention-to-treat 분석에서는 primary end point가 rivaroxaban군에서 269명(1년에 2.1%)이 발생했 고, warfarin군은 306명(1년에 2.4%)(HR, 0.88; 95% CI, 0.74 to 1.03; p<0.001 for noninferiority; p=0.12 for superiority) 이 발생되었다. 심각한 그리고 임상적으로 의미있는 출혈이 rivaroxaban군에서 1,475명(1년에 14.9%)이 발생하였고, war- farin군에서 1,449명(1년에 14.5%)(HR, 1.03; 95% CI, 0.96 to 1.11; p=0.44)이 발생되었고, ICH는 의미있게 낮게 (0.5%
vs. 0.7%, p=0.02) 그리고 치명적인 출혈은 rivaroxaban군에 서 낮았다(0.2% vs. 0.5%, p=0.003). 그러나, 위장관계 출혈 은 warfarin군보다 rivaroxaban군에서 높았다(3.3% vs. 2.2%, p<0.001).
심방세동이 있는 환자에서 뇌졸중이나 전신 혈전 예방에 warfarin보다 열등하지 않으며 ravaroxaban군이 뇌내출혈이
나 치명적인 출혈이 적게 나타나긴 했지만, 심각한 출혈의 발생빈도는 비슷하였다.
3) Apixaban versus Aspirin: Apixaban versus Acetyl- salicylic Acid to Prevent Stroke in Atrial Fibrillation Patients Who Have Failed or Are Unsuitable for Vitamin K Antagonist Treatment (AVERROES)6 AVERROES 연구는 심방세동이 있는 환자에서 warfarin을 쓸 수 없는 경우에 환자에서 뇌졸중과 전신 혈전예방을 위해 apixaban과 aspirin의 효용성을 비교한 randomized, double- blind 그리고 double-dummy 임상 연구이다. Apixaban군에서 primary event가 51명(1년에 1.6%) 발생하였고, aspirin군에 서 113명(1년에 3.7%)이 발생하였다(HR, 0.45; 95% CI, 0.32 to 0.62; p<0.001). 사망률은 apixaban군에서 1년에 3.5% 그 리고 aspirin군은 1년에 4.4%였다(HR, 0.79; 95% CI, 0.62 to 1.02; p=0.07). Apixaban군에서 심각한 출혈은 44예(1년 에 1.4%)가 있었고, aspirin군은 39예(1년에 1.2% )가 있었다 (HR, 1.13; 95% CI, 0.74 to 1.75; p=0.57). 뇌 내출혈은 apixa- ban군에서 11예, aspirin군에서 13예 있었다. Apixaban은 aspi- rin에 비해 심혈관계 원인에 의한 첫 입원의 위험을 줄였다(1 년에 12.6% 대 1년에 15.9%, p<0.001).
Warfarin을 쓸 수 없는 심방세동 환자에서 apixaban은 심각 한 출혈이나 ICH의 위험도를 임상적으로 증가시키지 않고, 뇌졸중이나 전신 혈전의 위험을 감소시켰다.
4) Apixaban versus Warfarin: Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE)7
The ARISTOTLE 연구는 비판막성 심방세동환자에서 api- xaban (하루 두 번 5 mg ,또는 80세 이상, 체중 60 kg 이하 또는 serum creatinine ≥1.5 mg/dL 인 환자는 하루 2.5 mg 두 번)과 용량조절된 warfarin을 비교한 실험으로 randomized, double-blind, double-dummy, III상 임상 연구이다.
Primary outcome은 허혈성 또는 출혈성 뇌졸중 또는 전신 혈전으로 하였다. Primary outcome의 빈도는 apixaban군에서 1년에 1.27% 였고, 이에 비하여 warfarin군은 1년에 1.60%
였다(HR, 0.79; 95% CI, 0.66 to 0.95; p<0.001 for noninferi- ority; p=0.01 for superiority). Major bleeding 발생빈도는 apixaban군이 1년에 2.13% per year, 이에 비해 warfarin군은 1년에 3.09% 였고(HR, 0.69; 95% CI, 0.60 to 0.80; p<0.001), 어떤 원인이든 사망률은 각각 3.52% 그리고 3.94% 였다(HR, 0.89; 95% CI, 0.80 to 0.99; p=0.047). 출혈성 뇌졸중의 발생
빈도는 apixabav군이 1년에 0.24%였고, 이에 비해 warfarin 군은 1년에 0.47%였고(HR, 0.51; 95% CI, 0.35 to 0.75; p<
0.001), 허혈성 그리고 원인불명의 뇌졸중 발생이 apixaban 군이 1년에 0.97% 그리고 warfarin군이 1년에 1.05%로 나타 났다(HR, 0.92; 95% CI, 0.74 to 1.13; p=0.42). 심방세동 환자 에서 apixaban은 warfarin 보다 뇌졸중 또는 전신 혈전의 예방 에 우수하며, 출혈이 적고 사망률이 적은 것으로 나타났다.
5) Edoxaban versus Warfarin: The Effective Anticoa- gula tion with Factor Xa Next Generation in Atrial Fibrillation-Thrombolysis in Myocardial Infarction 48 (ENGAGE AF-TIMI 48)8
ENGAGE AF-TIMI 48 임상 연구는 warfarin과 edoxaban 두용량{고용량: 60 mg/일 (E60), 저용량: 30 mg/일 (E30)}을 비교한 것으로 randomized, double-blind, double-dummy 연 구이다. Primary end point는 중등도와 고위험 심방세동환자 에서의 뇌졸중 또는 전신혈전이다. Primary end point는 war- farin군은 1년에 1.50% 발생하였고, 이에 비해 E60은 1.18%
(HR, 0.79; 97.5% CI, 0.63 to 0.99; p<0.001 for noninferi- ority) 그리고 E30은 1.61% 였다(HR, 1.07; 97.5% CI, 0.87 to 1.31; p=0.005 for noninferiority). Intention-to-treat 분석 에서, E60은 warfarin에 비하여 좋은 결과를 보여주는 경향을 보였으나(HR, 0.87; 97.5% CI, 0.73 to 1.04; p=0.08), E30은 warfarin군에 비하여 좋지 않은 경향을 보였다(HR, 1.13; 97.5
% CI, 0.96 to 1.34; p=0.10). 심각한 출혈의 발생빈도는 war- farin군에서 1년에 3.43% 대 E60은 1년에 2.75% (HR, 0.80;
95% CI, 0.71 to 0.91; p<0.001) 그리고 E30은 1년에 1.61%
이었다(HR, 0.47; 95% CI, 0.41 to 0.55; p<0.001). 심혈관계 원인에 의한 매년 사망률은 3.17% 대 2.74%(warfarin 대 E30;
HR, 0.86; 95% CI, 0.77 to 0.97; p=0.01), 그리고 2.71%이다 (warfarin 대 E60; HR, 0.85; 95% CI, 0.76 to 0.96; p=0.008).
Key secondary end point (a composite of stroke, systemic embolism, 또는 심혈계 원인에 의한 사망)는 4.43% 대 3.85%
(warfarin 대 E30; HR, 0.87; 95% CI, 0.78 to 0.96; p=0.005), 그리고 4.23% (warfarin 대 E60; HR, 0.95; 95% CI, 0.86 to 1.05; p=0.32)이다.
Edoxaban을 하루 한 번 투여한 양군 모두 warfarin에 비하 여 출혈이 임상적으로 낮은 빈도와 심혈관계 원인에 의한 사 망률을 낮추면서 뇌졸중 또는 전신 혈전 예방에 열등하지 않 은 것으로 나타났다.
NOACs을 투여한 임상연구를 요약하면 다음과 같다: 뇌졸 중을 예방하는데 있어, NOACs은 잘 용량조절된 warfarin에
Table 3. 비판막성 심방세동 환자의 권고사항
1. The selection of antithrombotic therapy should be considered using the same criteria irrespective of the pattern of AF such as paroxysmal, persistent, and permanent.
2. The CHA2DS2-VASc score is recommended for the assessment of stroke risk.
2-1. The CHA2DS2-VASc score should be used for the appropriate antithrombotic therapy.
2-2. NOACs or anticoagulant therapy using warfarin should be recommended for antithrombotic therapy when the CHA2DS2-VASc score is 1 or greater.
2-3. Antithromboatic therapy is not recommended when the CHA2DS2-VASc score is 0.
2-4. The CHA2DS2-VASc score is considered as 0 when being female is the only risk factor.
3. Warfarin is recommended in the following cases:
3-1. Patients with valve replacement or rheumatic valve disease.
3-2. Patients with nonvalvular FA in whom INR is well controlled and no significant bleeding is present.
4. Optimal INR during warfarin treatment.
4-1. Optimal INR range is 2-3.
4-2. Time in therapeutic range should be at leaset over 60% to maximize the benefit of warfarin.
5. Aspirin monotherapy or combination therapy with aspirin and clopidogrel can be considered when oral anticoagulation therapy is not suitable or patients refuse the use of oral anticoagulants.
6. Oral anticoagulation therapy may be judiciously combined with antiplatelet therapy in the following cases:
6-1. Recurrence of thromboembolism despite adequate oral anticoagulation therapy.
6-2. Concomitant antiplatelet therapy may be considered for the treatment of nonembolic cerebral infarction or TIA.
6-3. Presence of concemitant ischemic heart disease.
6-4. Coronary artery stenting.
7. Switch from warfarin to NOACs, and cautions for the administration of NOACs.
7-1. NOACs may not be used in place of warfarin in patients with stable anticoagulation control without bleeding complications.
7-2. NOACs are recommended in place of warfarin for patients requiring anticoagulation therapy who have hypersensitivity or contraindication against warfarin, cannot maintain an INR within the optimal range, or have cerebral hemorrhage despite an INR that is adequately maintained.
7-3. For the administration of dabigatran, 150 mg twice daily is recommended as a standard regimen. Dose reduction (110 mg twice daily) should be considered in the following cases:
- Elderly patients (≥80 years old), concomitant administration of interacting drugs (e.g., verapamil), high bleeding risk (HAS-BLED score ≥3), or moderate renal dysfunction(CiCl 30-49 mL/min).
7-4. For the administration of rivaroxaban, 20 mg once daily is recommended as a standard regimen. Dose reduction (15 mg once daily) should be considered in the following case:
- High bleeding risk (HAS-BLED score≥3) or moderate renal dysfunction (CrCl 30-49 mL/min).
7-5. For the administration of apixaban, 5mg twice daily is recommended as a standard regimen. Dose reduction (2.5 mg twice daily) should be considered for the following cases:
- Renal dysfunction (CrCl 30-49 mL/min)
- Patients who have 2 or more of the fololwing 3 factors:
Elderly patients (≥80 years old), body weight ≤60 kg, or serum creatinine level ≥15 mg/dL)
7-6. The assessment of renal function should be carried out prior to the use of NOACs and annually monitored in patients with normal (CrCl
≥80 mL/min)
7-7. NOACs are not recommended in patients with severe renal dysfunction (CrCl<30 mL/min).
8. Anticoagulant therapy for patients who are scheduled for an invasive procedure or a surgery with the possibility of bleeding complications.
8-1. For patients with warfaring therapy, INR should be measured within 24 hours before an invasive procedure or a surgery, and an INR of
≤1.5 is generally considered safe with regard to the risk of periprocedural or perioperative bleeding. Warfarin can be reintroduced 24 hours later when hemostasis is confirmed and the patient is under a stable condition.
8-2. For patients with CrCl≥50 mL/min, dabigatran should be ceased 1 day prior to procedures with low bleeding risk, and 2-3 days for high bleeding risk procedures. For patients with CrCl 30-49 mL/min, dabigatran should be ceased 2 days prior to procedures with low bleeding risk, and 3-4 days prior to procedures with high bleeding risk.
8-3. For patients with CrCl≥30 mL/min, rivaroxaban should be ceased 1 day prior to procedures with low bleeding risk, and more than 2 days prior to procedures with high bleeding risk.
8-4. For patients with CrCl≥30 ml/min, apixaban should be ceased 1 day prior to procedures with low bleeding risk, and 2 days prior to procedure with high bleeding risk. For patients with <30 mL/min, apixaban should be ceased 2 days prior to procedures with low bleeding risk, and more than 2 days prior to procedures with high bleeding risk.
9. Anticoagulation therapy for conducting an elective cardioversion or radiofrequency catheter ablation
9-1. To conduct elective direct current cardioversion for patients with AF of ≥48 hours duration or unknown time of occurrence, anticoagulant therapy with warfarin (INR 2.0-3.0) is recommended for ≥3 weeks prior to and ≥4 weeks after cardioversion to reduce the risk of thromboembolism.
9-2. To conduct radiofrequency catheter ablation for patients with AF of ≥48 hours duration or unknown time of occurrence, anticoagulant therapy with warfarin (INR 2.0-3.0) is recommended for ≥3 weeks prior to and 2 months after cardioversion to reduce the risk of thromboembolism.
9-3. For the application fo NOACs prior to or after elective cardioversion, supporting evidence is currently insufficient and limited.
10. For patients with atrial flutter, antithrombotic therapy is recommended according to the same criteria apolied for AF.
비하여 우수하거나 비열등하며, 출혈이 비슷하거나, 적은 빈 도로 나타났다.16 그러므로 NOACs은 잘 조절되지 않는 INRs 환자, 출혈합병증의 과거력, 뇌졸중의 예방을 위해 warfarin 을 투여하였으나, 뇌졸중의 과거력이 있는 환자에서 추천될 수 있는 약제이다.17
3. Warfarin을 쓸 수 없는 심방세동 환자에서 항혈소판 제제 치료
1) Effect of Clopidogrel Added to Aspirin in Patients with Atrial Fibrillation: The Atrial Fibrillation Clopi- dogrel Trial with Irbesartan for Prevention of Vas- cular Events (ACTIVE A)18
ACTIVE A 임상 연구는 뇌졸중의 위험인자가 하나 이상 가진 심방세동 환자에서 aspirin단독 요법(75-100 mg/일)과 aspirin과 clopidogrel (75mg/일)의 병합요법과의 효용성을 보 기위한 연구이다. Primary outcome는 뇌졸중, 심근경색, 비중 추성 혈전의 composite 또는 혈관에 의한 사망으로 하였다.
주요 혈관사건은 병합요법군에서 832명(1년에 6.8%) 그리고 단독요법군에서 924명(1년에 7.6%)이 발생하였다(RR, 0.89;
95% CI, 0.81 to 0.98; p=0.01).
차이는 주로 병합요법에서 뇌졸중의 발생빈도가 감소한데 기인한다. 뇌졸중은 병합요법에서 296명(1년에 2.4%) 그리 고 단독요법에서 408명(1년에 3.3%)이 발생하였다(RR, 0.72;
95% CI, 0.62 to 0.83; p<0.001). 심근경색증은 병합요법군 에서 90명(1년에 0.7%) 그리고 단독요법군에서 115명(1년에 0.9%)이 발생하였다(RR, 0.78; 95% CI, 0.59 to 1.03; p=
0.08). Major bleeding은 병합요법군에서 251 명(매년 2.0%) 그리고 단독요법군에서 162명(매년 1.3%)이 발생하였다(RR, 1.57; 95% CI, 1.29 to 1.92; p<0.001).
2) Vitamin K antagonist 치료를 할 수 없는 심방세동 환자 에서 aspirin에 clopidogrel의 추가는 major vascular events, 특히 뇌졸중을 줄이는 반면 심각한 출혈의 위험 성은 증가시킨다.
(1) Clopidogrel Plus Aspirin versus Oral Anticoagulation for Atrial Fibrillation in the Atrial Fibrillation Clopido- grel Trial with Irbesartan for Prevention of Vascular Events (ACTIVE W): a randomized controlled trial19 ACTIVE W는 randomized, controlled, open-label 연구이 며, 복합요법(aspirin 75-100 mg/일과 clopidogrel 75 mg/일) 과 oral vitamin K antagonist (warfarin) 치료의 효능을 비교하 는 연구이다. 이 연구는 warfarin 치료의 우수성이 확인되어
일찍 종료되였다. Warfarin 치료군에서 165 primary events가 생겼고(매년 3.93%) 병합요법군에는 234명 발생하였다(매년 5.60%; RR 1.44; 95% CI, 1.18 to 1.76; p=0.0003).
Warfarin 치료는 뇌졸중의 고위험인자를 가진 심방세동 환 자의 혈관사건, 특히 뇌졸중, 을 예방하는데 병합요법보다 우 수하며, 이는 이미 경구용 항응고제를 복용하고 있는 경우도 해당된다.
16개 연구를 메타 분석한 결과를 보면 심방세동을 가진 환자 에서 용량조절된 warfarin은 비록 심각한 뇌외 출혈은 증가되 었으나, 뇌졸중의 위험도를 62% 줄였고, 반면 aspirin은 22%
줄인 것으로 나타났다.20 Aspirin에 비하여 warfarin 은 심방세 동의 형태에 관계없이 모든 뇌졸중, 허혈성 뇌졸중을 포함해 서, 심혈관계 사건의 위험도를 의미있게 줄였다.21 고령(>75 세)은 확실히 뇌졸중과 출혈의 위험인자가 분명하기 때문에 항응고치료가 아스피린보다는 치료의 일차적으로 생각해야 만 한다.22 그러나, 실제임상에서 항혈소판제제가 경구용 항 응고제를 쓸 수 없는 경우에 대안으로 적용되고 있다. ACTIVE A 연구 결과에 의거하여 aspirin 단독요법이 효과적인지 병합 요법이 더 효과적인지 결정하기 어려울 때에는 출혈 위험성 이 낮을 경우 병합요법을 고려하여 넣어야 한다.
1. Paroxysmal, persistent, permanent 같은 심방세동의 형 태에 관계없이 항혈전요법을 고려해야 한다.
2. 뇌졸중 위험도를 평가하기 위해서 CHA2DS2-VASc score 가 추천된다.
1) 적절한 항혈전 치료를 하기 위해 CHA2DS2-VASc score 를 사용해야만 한다.
2) NOACs 또는 warfarin을 사용한 항응고 치료를 할 때에 는 CHA2DS2-VASc score가 1 보다 클 경우만 항혈전 치 료가 추천된다.
3) CHA2DS2-VASc score가 0 일 때에는 항혈전 치료가 추천 되지 않는다.
4) 여성만이 유일한 위험인자인 경우에는 CHA2DS2-VASc score 가 0으로 간주된다.
ESC 2012 권고사항에는 score가 1 보다 큰 경우에는 war- farin 보다 NOACs이 우선적으로 추천된나 score가 0인 환자 에게는 항혈전 치료가 추천되지 않는다. APHRS 2013 권고사 항에는 score가 2 이상인 환자에게는 NOACs 또는 warfarin 가 추천된다. score가 1인 환자에게는 NOACs (rivaroxaban을 제외한 dabigatrin 또는 apixaban)이 우선적으로 추천되며, rivaroxaban 또는 warfarin이 대체 약품으로 생각된다. score 가 0인 환자는 항혈전치료가 추천되지 않는다. ROCKET AF
연구에 따르면, rivaroxaban가 CHADS2 score가 2 보다 큰 환자 에 투여되었다. 이런 이유로, CHA2DS2-VASc score가 1인 경우 (APHRS 2013) 대체 약품으로 추천된다. 한편, 2014 AHA/ ACC/
HRS guideline을 보면, CHA2DS2-VASc score가 1인 환자의 항 응고치료는 다양해 보인다: 항혈전 치료를 안 하거나 항응고제 나 asprin을 고려하기도 한다.
3. Warfarin은 다음의 경우에 추천된다:
1) 판막대치술을 받았거나 류마틱 판막질환이 있는 환자.
2) 비판막성 심방세동이 있는 환자로 INR이 잘 조절되고 심각한 출혈이 없는 경우
4. Warfarin치료시 적정한 INR 1) 적정한 INR 범위는 2-3
2) Warfarin의 효능을 최대한 하기 위해 적어도 치료 범위 의 시간이 60% 이상 되어야 한다.
APHRS 2013 권고사항에서는 뇌 내출혈과 그 밖의 심각한 출혈을 최소화하고 허혈성 뇌졸중을 효과적으로 예방하기 위 해 고령(≥70세)의 아시안인은 INR의 적정 범위를 1.6-2.6 으로 생각했다.
5. Aspirin 단독요법 또는 aspirin과 clopidogrel을 이용한 병합요법은 경구용 항응고 치료를 하지 못하는 경우나 경 구용 항응고 치료를 거부하는 환자에서 고려될 수 있다.
6. 경구용 항응고치료는 다음과 같은 경우에 항혈소판제 제와 병용이 신중하게 할 수 있다:
1) 항응고 치료를 적절히 했음에도 혈전이 재발하는 경우 2) 비혈전성 뇌경색증이나 TIA의 치료에 항혈소판 제제를
병용을 고려할 수 있다.
3) 허혈성 심질환이 동반된 경우 4) 관상동맥 스텐팅을 하는 경우
7. Warfarin에서 NOACs으로 바꿀 때 투여에 주의할 상황 1) 출혈없이 항응고 조절이 안정적으로 유지되고 있는 환자 에서 warfarin 대신 NOACs을 사용하지 않을 수도 있다.
2) Warfarin에 과민반응이 있거나 warfarin에 대해 비적응 증이 있는데 항응고 치료를 받아야 하는 경우, INR이 적정하게 유지되지 않는 경우, INR이 적절히 유지됨에 도 뇌출혈이 발생한 경우에 NOACs은 warfarin 대신 추 천된다.
3) Dabigatran을 투여하는 경우에는 표준치료로서 하루 두 번 150 mg이 추천되며 다음과 같은 경우 용량(하루 두
번 110 mg)을 줄이는 것을 고려해야 한다:
- 고령(80세 이상), 상호작용이 있는 약제와 병합 투여할 경우(e.g., verapamil), 고출 혈위험(HAS-BLED score ≥ 3), 또는 중등도의 신장기능 이상 (CrCl 30-49 mL/min).
4) Rivaroxaban을 투여하는 경우에는 표준치료로서 하루 한번 20 mg이 추천된다. 다음과 같은 경우는 용량을 (하 루 한번 15 mg) 줄이는 것을 고려해야 한다:
- 고출혈위험(HAS-BLED score ≥3) 또는 중등도 신장기 능이상(CrCl 30-49 mL/min).
5) Apixaban을 투여하는 경우에는 표준치료로서 하루 두 번 5 mg. 다음과 같은 경우에는 용량을(하루 두 번 2.5 mg) 줄이는 것을 고려해야 한다:
- 신장기능 이상(CrCl 30-49 mL/min)
- 다음 3요소 중 2개 이상을 가진 환저인 경우: 고령(≥80 years old), 체중 ≤60 kg, 또는 혈중 크레아티닌농도 ≥ 1.5 mg/dL.
6) NOACs을 투여 전 신장기능 검사를 실시해야 하며, 정상 (CrCl ≥80mL/min) 또는 경도의 신장기능 이상(CrCl 50- 79 mL/min)이 있는 경우 매년 신장기능 검사를 실시해야 한다. 신장 기능이 중등도 신장 기능 이상(CrCl 30-49 mL/
min) 인 경우 매년 2-3번씩 신장기능 검사를 해야 한다.
7) 신장기능 이상(CrCl <30mL/min)이 중증인 경우 NOACs 은 항응고치료로 추천되지 않는다.
8. 출혈합병증의 가능성이 있는 관혈적인 시술이나 수술 이 예정된 환자의 항응고요법
1) Warfarin 치료를 하던 환자인 경우 관혈적인 시술이나 수술전 24시간 내에 INR을 검사하여야 하며, 시술 전, 후나 수술 전, 후의 출혈의 위험성을 생각해 보면 INR이
≤1.5면 일반적으로 안전한 것으로 생각된다. Warfarin 은 지혈이 확인되고 환자가 안전한 상태가 된 후 24시간 후에 재투여될 수 있다.
2) 신장기능이 CrCl ≥50 mL/min 인 환자의 경우, 저출혈 위험도의 시술은 하루 전, 고출혈 위험도시술이면 2-3 일전에 dabigatran을 중지해야 한다. 신장기능이 CrCl 30-49 mL/min 인 환자인 경우는 저출혈 위험도의 시술 인 경우는 2일 전 고출혈 위험도인 시술인 경우 3-4일 전에 dabigatran을 중지해야만 한다.
3) 신장 기능이 CrCl ≥30 mL/min 인 환자인 경우 저출혈 위험도의 시술은 하루전, 고출혈 위험도시술인 경우 rivaroxaban을 2일 전에 중지하여만 한다. 신장 기능이
<30 mL/min 인 환자의 경우 저출혈 위험도인 시술인 경우 2일 전에 고출혈 위험도의 시술인 경우 2일 이상 전에 중지하여야 한다.
4) 신장 기능이 CrCl ≥30 mL/min 인 환자인 경우, 저출혈 위험도인 시술의 경우 1일전에 그리고 고출혈 위험도의 시술인 경우 2일 전에 apixaban을 중지하여야 한다. 신 장기능이 <30 mL/min 인 환자는 저출혈 위험도의 시술 인 경우 2일 전에 그리고 고출혈 위험도의 시술인 경우 2일 이상 전에 apixaban을 중지하여야 한다.
Warfarin을 투여하는 동안 혈전의 고위험군에는 bridge the- rapy를 고려할 수 있다. 그러나, NOACs에는 bridge therapy가 필요치 않다. NOACs를 투여받는 환자는 적절한 antagonist가 없기 때문에 주의하여야 한다.
9. Elective cardioversion이나 radiofrequency catheter abla- tion을 받는 환자의 항응고 치료
1) 48시간 이상된 심방세동이나 언제 생긴 지 모르는 심방 세동인 환자에서 elective direct current cardioversion을 실시할 때에는 혈전위험을 예방하기 위하여 warfarin
(2.0-3.0)이 cardioversion 3주 전, 그리고 cardioversion 4주 후에 투여하는 것이 추천된다.
2) 발생 48시간의 기간을 갖거나 언제 발생하였는지 모르 는 심방세동 환자에서 radiofrequency catheter ablation 를 실시하는 경우에는 혈전의 위험을 줄이기 위해 시술 3주 전 이상, 시술 후 2개월 이상에 warfarin(INR 2.0-3.0) 을 이용한 항응고치료가 추천된다.
3) Elective cardioversion의 전, 후에 NOACs의 적용은 증 거가 불충분하거나 제한적이다.
Dabigtran을 이용한 RE-LY 연구의 하위분석에서 defibrilla- tion 후 처음 30일에 warfarin에 비하여 혈전의 발생 빈도가 증가하지 않았다. 현재 NOACs을 이용한 여러 연구의 결과에 따라 추천사항이 개정될 수 있다.
10. 심방조동을 가진 환자의 경우 항혈전 치료는 심방세동 을 가진 환자와 같은 기준으로 실시한다.
1) Warfarin 또는 NOACs으로 치료시 발생하는 아시아 인의 뇌졸중과 출혈의 특성: 인종간의 특성 (1) Dabigatran 대 Warfarin: 심방세동을 가진 아시아인과
비아시안인의 허혈성과 출혈성 뇌졸중에 대한 효과23
RE-LY 연구에서 아시아 10개국의 2,782명(15%)과 34개
국의 비아시아국의 15,331명(85%)에 대하여 post hoc 분석 이 실시되었는 바 총 18,113에 대하여 dabigatran 또는 war- farin 치료의 뇌출혈과 심각한 출혈의 발생빈도를 비교하였 다. 아시안에서 뇌출혈의 발생 빈도는 dabigatran 110 mg (D110) 그리고 150 mg (D150) 양군에서 warfarin군에 비하 여 현저히 낮게 나타났다(D110 대 warfarin HR, 0.15; 95%
CI, 0.03-0.66 and D150 대 warfarin HR, 0.22; 95% CI, 0.06- 0.77). 심각한 출혈 또한 D110 그리고 D150 양군에서 war- farin에 비해 낮았다(D110 매년 2.22% , D150 매년 2.17%, 그리고 warfarin 매년 3.82%). 비아시아인에서는 뇌출혈과 심각한 출혈의 발생빈도는 차이가 없었다.
(2) Apixaban 대 Warfarin: ARISTOTLE 연구의 하위분석7 지금까지 아시아인에서 apixaban이나 warfarin으로 치료 해서 출혈합병증의 발생 빈도를 분석한 보고는 없었다. 그러 나, ARISTOTLE 연구의 하위분석에 따라 아시아인에서 war- farin군 보다 apixaban군에서 심각한 출혈의 빈도가 낮았다.
(3) ROCKET심방세동 연구로부터 동아시아인에서 뇌졸중 예방에 대한 Rivaroxaban 효과24
ROCKET 심방세동 연구에 참여한 932명은 동아시아에 거 주하고 있었다. 동아시아인에서 절대 event rate가 높음에도 불구하고, primary efficacy end point (stroke/systemic embo lism)에 대하여 rivaroxaban과 warfarin의 상대 효능은 동아시 아인과 비동아시아인에서 일관되게 나타났다(interaction p=
0.666). Rivaroxaban 또는 warfarin으로 치료한 환자에서 임 상적으로 의미있는 major 또는 minor bleeding이 동아시아인 이나 비동아시아인에서 일관되게 나타났다(interaction p=
0.867). 관찰된 상대 효능과 안전성은 rivaroxaban이나 war- farin 모두 동아시아 안이나 밖에서 비슷했다.
Warfarin을 투여받은 백인이 아닌 환자는 백인에 비해 의 미있게 ICH의 발생 위험도가 높았는바, 흑인은 HR 2.05, 히 스패닉은 2.06, 그리고 아시아인은 4.1로 나타났다. Warfarin 을 투여받지 않은 환자는 ICH의 빈도가 인종 간에 차이가 없었다.25 출혈성 뇌졸중의 발생빈도는 타인종에 비하여 아시 아인에게서 2.4배 높았기 때문에 APHRS 2013 권고사항에는 70세가 넘는 아시아인 경우 적절한 INR은 1.6-2.6으로 추천 하였다. 4개의 NOACs를 투여한 메타분석을 출간한 자료, 뇌 졸중 예방과 출혈 합병증에 대한 3개의 연구 중심이 되는 기 간 동안의 자료를 보면 warfarin군과 심각한 출혈은 비슷하나 뇌졸중, ICH, 사망률이 의미있게 감소하는 등 유망한 risk-
Fig. 1. 비판막성 심방세동 환자의 항응고 치료의 알고리즘.
*Aspirin, clopidogrel 또는 병합요법. Solid-line box: recommended option, dotted-line box: alternative option.
NOACs: new oral anticoagulants, VKA: vitamin K antagonist.
benefit profile을 보여 주었다.16 이런 이유로 ICH면(출혈성 뇌졸중을 포함)에서 추가적인 연구 결과가 필요하지만, NOACs 은 비판막성 심방세동 아시아 환자에서 유익할 수 있다.
항혈전치료는 비판막성 심방세동 환자에서 뇌졸중과 전신 혈전을 예방하는 데 중요한 역할을 담당하고 있다. 그러나, 투약으로 인한 출혈합병증 최소화하고 예방 효과를 최대화하 기 위해 각 환자의 임상적인 특성을 주의 깊게 고려해야 한다.
뇌졸중의 위험도를 개량화하는 데는 CHADS2 score 보다는 CHA2DS2-VASc score가 추천된다. 출혈위험을 측정하는 데는 HAS-BLED score가 추천된다. 비판막성 심방세동이 있으나, CHA2DS2-VASc score가 0 인 환자에게 항혈전 치료가 추천되 지 않는다. CHA2DS2-VASc score가 2 이상일 때 항응고치료가
추천된다. 출혈합병증의 가능성이 있는 경우라면 과거의 연 구에 근거해서 warfarin 보다는 NOACs을 고려해야 한다. 비 판막성 심방세동인 환자에서 CHA2DS2-VASc가 1인 경우 항 응고 치료가 선호되나 항혈전 치료를 하지 않거나 항혈소판 제제를 이용한 치료를 고려에 넣어야 한다(Fig. 1).
REFERENCES
1. Camm AJ, Lip GY, De Caterina R, et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrilla- tion: an update of the 2010 ESC Guidelines for the manage- ment of atrial fibrillation. Developed with the special contri- bution of the European Heart Rhythm Association. Eur Heart J 2012;33:2719-47.
2. Park JM, Hong KS, Han SW, et al. Focused update on primary stroke prevention in patients with atrial fibrillation in Korean Clinical Practice Guidelines for Stroke. Korean J Stroke 2012;
14:106-15.
3. Albers GW, Diener HC, Frison L, et al. Ximelagatran vs war- farin for stroke prevention in patients with nonvalvular atrial fibrillation: a randomized trial. JAMA 2005;293:690-8.
4. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139-51.
5. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011;
365:883-91.
6. Connolly SJ, Eikelboom J, Joyner C, et al. Apixaban in patients with atrial fibrillation. N Engl J Med 2011;364:806-17.
7. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011;365:981-92.
8. Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2013;
369:2093-104.
9. Clinical Research Center for Stroke. Writing group of clinical practice guideline for stroke. Clinical Practice Guideline for Stroke. 1st ed. Seoul: Clinical Research Center for Stroke; 2009.
pp. 34-35.
10. European Heart Rhythm Association; European Association for Cardio-Thoracic Surgery. Camm AJ, et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J 2010;31:2369-429.
11. Skanes AC, Healey JS, Cairns JA, et al. Focused 2012 update of the Canadian Cardiovascular Society atrial fibrillation gui- delines: recommendations for stroke prevention and rate/rhy- thm control. Can J Cardiol 2012;28:125-36.
12. Ogawa S, Aonuma K, Tse HF, et al. The APHRS's 2013 state- ment on antithrombotic therapy of patients with nonvalvular atrial fibrillation. J Arrhythm 2013;29:190-200.
13. January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrilla- tion: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Pra- ctice Guidelines and the Heart Rhythm Society. Circulation 2014;130:2071-104.
14. Olesen JB, Lip GY, Hansen ML, et al. Validation of risk stra- tification schemes for predicting stroke and thromboembolism
in patients with atrial fibrillation: nationwide cohort study.
BMJ 2011;342:d124.
15. Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest 2010;138:1093-100.
16. Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomi- sed trials. Lancet 2014;383:955-62.
17. Bang OY, Hong KS, Heo JH, et al. New oral anticoagulants may be particularly useful for Asian stroke patients. J Stroke 2014;16:73-80.
18. ACTIVE Investigators. Connolly SJ, Pogue J, et al. Effect of clopidogrel added to aspirin in patients with atrial fibrillation.
N Engl J Med 2009;360:2066-78.
19. ACTIVE Writing Group of the ACTIVE Investigators. Con- nolly S, Pogue J, et al. Clopidogrel plus aspirin versus oral anti- coagulation for atrial fibrillation in the Atrial fibrillation Clo- pidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): a randomised controlled trial. Lancet 2006;367:
1903-12.
20. Hart RG, Benavente O, McBride R, Pearce LA. Antithrombo- tic therapy to prevent stroke in patients with atrial fibrillation:
a meta-analysis. Ann Intern Med 1999;131:492-501.
21. van Walraven C, Hart RG, Singer DE, et al. Oral anticoagu- lants vs aspirin in nonvalvular atrial fibrillation: an individual patient meta-analysis. JAMA 2002;288:2441-8.
22. Mant J, Hobbs FD, Fletcher K, et al. Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trial. Lan- cet 2007;370:493-503.
23. Hori M, Connolly SJ, Zhu J, et al. Dabigatran versus warfarin:
effects on ischemic and hemorrhagic strokes and bleeding in Asians and non-Asians with atrial fibrillation. Stroke 2013;44:
1891-6.
24. Wong KS, Hu DY, Oomman A, et al. Rivaroxaban for stroke prevention in East Asian patients from the ROCKET AF trial.
Stroke 2014;45:1739-47.
25. Shen AY, Yao JF, Brar SS, Jorgensen MB, Chen W. Racial/
ethnic differences in the risk of intracranial hemorrhage among patients with atrial fibrillation. J Am Coll Cardiol 2007;50:
309-15.