When barium extravasates into tissue during radiolog- ic procedures such as barium enema, it is uptaken by macrophages and forms a granuloma. The result of this is a tumorous mass, fibrosis, and stricture (1), and a can- cerous condition is sometimes wrongly suspected. In al- most all cases of barium granuloma there is a history of barium enema, a fact which is helpful in making the correct diagnosis. We report a case of barium granuloma in which there was no history of barium enema or ap- parent rectal trauma.
Case Report
A 47-year-old man who for many years had suffered occasional left flank pain due to a ureter stone, was re- ferred for further evaluation of a rectal mass after an at- tack of colicky pain. For urologic evaluation, KUB (Fig.
1A) and intravenous urography (IVU) were performed at a local hospital; a highly attenuated pelvic lesion, about 1 cm in diameter and with fine strands around it, was found to be present. Colonoscopy and biopsy of the
lesion ware subsequently performed, but before the re- sults of these were known, the patient decided to visit our hospital. Computed tomography (CT) subsequently revealed that the mass was located in the rectal wall (Fig. 1B). The left flank pain had meanwhile subsided, and was presumed to have been due to the ureter stone.
The patient’s medical history showed that five years earlier, during a routine health check, he had undergone upper gastrointestinal series. Nine months later a colonoscopy was performed to evaluate abnormalities of the large bowel prior to hemorrhoidectomy, but no pathologic abnormality was found in any region, includ- ing the rectum. At follow-up colonoscopy, performed four years after the first such examination in the local hospital, a rectal mass was discovered. Symptoms such as diarrhea and weight loss were absent, and because there was no history of barium enema, our preoperative diagnosis was a calcified submucosal tumor such as gas- trointestinal stromal tumor, and the possible presence of milk of calcium in a retention cyst was also suggested.
The patient underwent lower anterior resection of the rectum. The mass was almost surrounded by rectal mu- cosa and the pathologic diagnosis was barium granulo- ma (Figs. 1C-E).
Discussion
Barium granuloma was first reported in 1954 as a pe- dunculated rectal mass (2), and by 1986, description of
J Korean Radiol Soc 2003;49:43-45
─ 43 ─
Barium Granuloma of the Rectum:
Case Report
1Dae Jin Kim, M.D., Se Hyung Kim, M.D., Ah Young Jeoung, M.D., Kyoung Ho Lee, M.D., Byung Ihn Choi, M.D., Joon Koo Han, M.D.
Barium granulomas usually occur after barium enema within 8 cm of the anal verge probably due to minute laceration of rectal wall by enema tip and extravasation of bar- ium during barium enema. We report a case of barium granuloma of rectum in a 47- year-old man, who did not have history of barium enema. In rare instance, barium granuloma can occur without a history of barium enema and careful interpretation of radiologic image is essential to make a correct diagnosis.
1Department of Radiology, Seoul National University College of Medicine, Institute of Radiation Medicine, Seoul National University Medical Research Center, and Clinical Research Institute, Seoul National University Hospital
Received March 20, 2003 ; Accepted May 30, 2003
Address reprint requests to : Joon Koo Han, M.D., Department of Radiology, Seoul National University College of Medicine, 28 Yongon- dong, Chongno-gu, Seoul 110-744, Korea.
Tel. 82-2-760-2514 Fax. 82-2-743-6385 E-mail: [email protected]
less than 45 cases had appeared in the literature in English (3). In the most recent report (4), a sigmoid polyp was diagnosed at barium enema and follow-up colonoscopy was performed three weeks later. A rectal barium granuloma was confirmed at subsequent follow- up colonoscopy, one year later.
The fact that most barium granulomas occur within 8 cm of the anal verge strongly suggests that insertion of the enema tip probably lacerates the rectal wall to some degree, enabling the barium to enter deeper tissue (5).
An inflammatory reaction ensues, a collection of cells (fibroblasts, multinucleated cells, macrophages, and
Dae Jin Kim, et al: Barium Granuloma of the Rectum
─ 44 ─
A B
C D
E
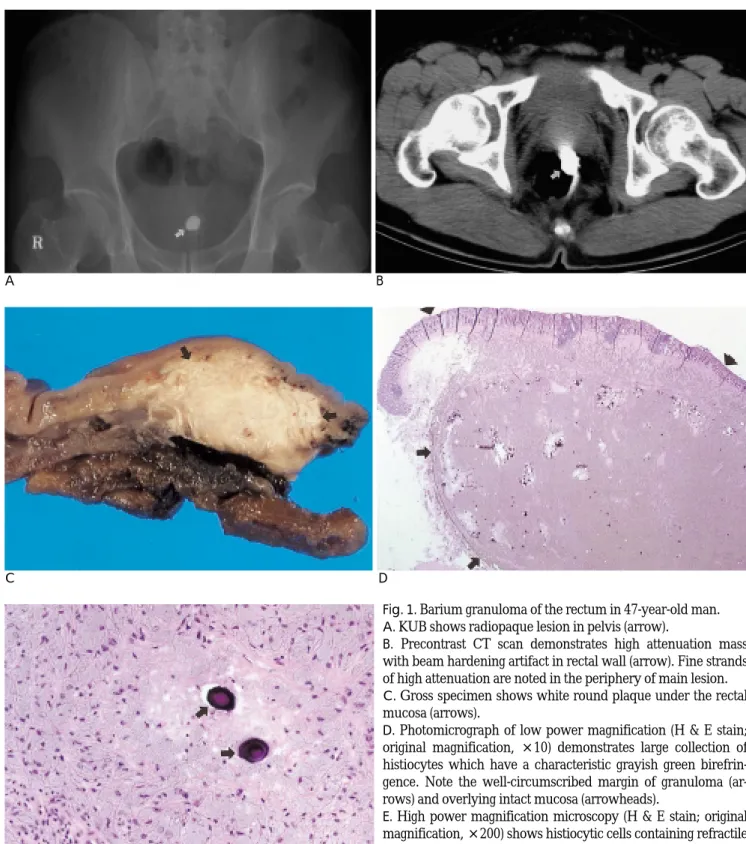
Fig. 1. Barium granuloma of the rectum in 47-year-old man.
A. KUB shows radiopaque lesion in pelvis (arrow).
B. Precontrast CT scan demonstrates high attenuation mass with beam hardening artifact in rectal wall (arrow). Fine strands of high attenuation are noted in the periphery of main lesion.
C. Gross specimen shows white round plaque under the rectal mucosa (arrows).
D. Photomicrograph of low power magnification (H & E stain;
original magnification, ×10) demonstrates large collection of histiocytes which have a characteristic grayish green birefrin- gence. Note the well-circumscribed margin of granuloma (ar- rows) and overlying intact mucosa (arrowheads).
E. High power magnification microscopy (H & E stain; original magnification, ×200) shows histiocytic cells containing refractile materials in submucosal layer. Several dystrophic calcifications (arrows) formed by dead barium-laden histiocytes are also seen.
lymphocytes) characteristic of a granulomatous reaction forming around the barium sulfate crystals (6). The ini- tial ulcerations usually heal within eight weeks (7), but in the case reported by Lewis et al. (8), a 1 cm-sized ul- cerated lesion 6 cm from the anal verge was detected two years after a barium enema.
Our case is differs from those previously reported in that our patient never underwent a barium enema. The only history of barium contact was during UGIS, and this was not preceded by any other incident incolcing possible infury of the rectal mucosa. The only procedure which could have caused rectal injury was a colonoscopy performed nine months after UGIS, and trauma was, therefore, a very unlikely cause of the bari- um granuloma.
Another possible explanation for the etiology of a bari- um granuloma without antecedent trauma is an intra- mural diverticulum. During its early stage of develop- ment, a diverticulum may reside in a muscle layer and will later protrude toward the serosa, with an opening to the lumen. Barium can be trapped within an intramural diverticulum and subsequent inflammatory reaction may seal off its orifice and give rise to an intramural bar- ium granuloma. At low-power magnification, the mass in our case was relatively well demarcated, a feature which may support this hypothesis. Another possible explanation is barium leakage through a small occult mucosal injury perhaps caused by passage of a hard
stool.
In conclusion, barium granuloma should be consid- ered when a highly-attenuated rectal lesion occurs in a patient previously exposed to barium, even without a history of rectal cannulation; the presence of fine strands at the periphery of the main mass might suggest this diagnosis. Final diagnosis depends on the bioptic findings: to obviate the need for surgery, as in our case, the radiologist should alert the pathologist to the possi- ble presence of barium-laden histiocytes in rectal tissue.
References
1. Fenoglio-preiser CM, Noffsinger AE, Stemmermann GN, et al.
Gastrointestinal pathology: an atlas and text. 2nd ed. Philadelphia:
Lippincott Williams and Wilkins 1999;1090-1092
2. Beddoc HL, Kay S, Kaye S. Barium granuloma of the rectum. JA- MA 1954;154:747-749
3. Arlow FL, D’Angelo DM. Barium granuloma mimicking rectal car- cinoma. Henry Ford Hosp Med J 1986;34:213-214
4. Elloway RS, DeRidder PH. Barium granuloma of the rectum.
Gastrointest Endosc 1991;37: 586-587
5. Gardiner H, Miller RE. Barium peritonitis. A new therapeutic ap- proach. Am J Surg 1973;125:350-352
6. Rand AA. Barium granuloma of the rectum. Dis Colon Rectum 1966;9:20-32
7. Carney JA, Stephens DH. Intramural barium (barium granuloma) of colon and rectum. Gastroenterology 1973;65:316-320
8. Lewis JW Jr, Kerstein MD, Koss N. Barium granuloma of the rec- tum: an uncommon complication of barium enema. Ann Surg 1975;
181:418-423 J Korean Radiol Soc 2003;49:43-45
─ 45 ─
대한방사선의학회지 2003;49:43-45
직장 바륨 육아종의 증례보고1
1서울대학교 의과대학 진단방사선과
김대진・김세형・정아영・이경호・최병인・한준구
바륨육아종은 주로 대장조영검사중에 관장기에 의한 직장벽의 작은 열상과 열상을 통한 바륨의 유출로 인해 발생하 며, 대장검사의 기왕력을 이용, 쉽게 진단할 수 있다. 저자들은 대장바륨검사의 기왕력이 없는 47세의 환자에서 발생 한 직장의 바륨육아종 1예를 보고하며, 이 증례에서처럼 바륨에 노출된적은 있지만 직장삽관경력이 없는 환자에서도 철저한 영상소견 분석을 통해 바륨육아종을 감별할 필요가 있다고 생각한다.