저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다. 변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
Master’s Thesis in Medicine
Craniovertebral junction abnormalities in
patients with congenital muscular torticollis
Ajou University Graduate School
Major in Medicine
Craniovertebral junction abnormalities in
patients with congenital muscular torticollis
Shin-Young Yim, M.D., Ph. D., Advisor
I submit this thesis as the Master’s thesis in Medicine
August 2016
Ajou University Graduate School
Major in Medicine
The Master’s thesis of Ah-Reum Ahn in Medicine is hereby approved.
Thesis Defense Committee President
Shin-Young Yim
Member Myong Chul Park
Member Sang Hyun Kim
Ajou University Graduate School
i
ABSTRACT
Background: To the best of our knowledge, no report on craniovertebral junction (CVJ) abnormalities, except those regarding atlanto-axial rotatory subluxation, in subjects with congenital muscular torticollis (CMT) has been published to date. This study aims to present a variety of concurrent CVJ abnormalities in subjects with CMT and examine the relationship between CVJ abnormalities and the clinical severity of CMT.
Methods: This retrospective cohort study included 48 subjects with CMT who underwent craniofacial computed tomography and neck magnetic resonance imaging. The CVJ was examined in terms of atlanto-occipital rotational angle and atlanto-axial rotational angle and lateral and anterior atlanto-dens intervals for evaluation of rotation of the atlanto-occipital joint, rotation of the atlanto-axial joint, and lateral and anterior shift of the atlanto-axial joint,
respectively. We assessed the correlation between degrees of CVJ abnormalities and the clinical severity of CMT. Cervicomandibular angle, cranial vault asymmetry index and ratio of intensity were measured as parameters for clinical severity.
Results: The mean age at the time of imaging study was 75.35±77.56 months in 48 subjects and 41 (85.4%) of them underwent a surgery for CMT. Thirty-one (64.6%) subjects had one or more CVJ abnormalities. Twenty-four (50%) subjects had rotation of the atlanto-axial joint with atlanto-axial rotational angle of more than 6 degrees. Nine (18.8%) subjects had rotation of atlanto-occipital joint with the atlanto-occipital rotational angle of more than 3 degrees. Thirteen (27.1%) subjects had lateral shift of atlanto-axial joint with difference of bilateral lateral ADIs of more than 2mm and no one had instability of the atlanto-axial joint with anterior ADI within normal range. Atlanto-occipital rotational angle and cervico-mandibular angle were positively correlated in 41 subjects who underwent surgery (r=0.32, p<0.05).
Conclusions: This appears to be the first documented study where subjects with CMT also presented with various types of CVJ abnormalities. CVJ abnormalities are common concurrent skeletal deformities in patients with CMT and presence of CVJ abnormalities may indicate the severe severity of CMT. Further prospective studies are required to verify these findings. Keywords: Torticollis/congenital; Atlanto-axial joint; Atlanto-occipital joint
ii
TABLE OF CONTENTS
List of Text
ABSTRACT ...……….. i TABLE OF CONTENTS ...………... ii I. INTRODUCTION ……..………. 1II. SUBJECTS AND METHODS ……….... 3
A. Enrollment ……… 3
B. Collection of demographic data ……… 3
C. Acquisition of craniofacial 3 dimentional computed tomography and neck magnetic resonance image ……… 3
D. Analysis of the severity of congenital muscular torticollis ………4
E. Analysis of craniovertebral junction abnormalities ………5
1. Rotation of the atlanto-occipital joint ……… 7
2. Rotation of the atlanto-axial joint………7
3. Lateral shift of the atlnto-axial joint ………7
4. Anterior shift of the atlanto-axial joint ………7
F. Statistical analysis………7
III. RESULTS ………..………..………..… 9
A. Characteristics of the subjects ………9
B. Inter-rater reliability of measurements………10
C. Analysis of the severity of congenital muscular torticollis ………11
D. Analysis of craniovertebral junction abnormalities ………11
E. Correlation between degrees of craniovertebral junction abnormalities and the severity of congenital muscular torticollis ………13
IV. DISCUSSION ………..…… 14
V. CONCLUSION ………..…… 16
REFERENCES ……….. 17
iii
List of Figures
Fig 1. Craniofacial computed tomography of the age-matched control and the patient with congenital muscular torticollis………...……… 6 Fig 2. Number of subjects according to the number of craniovertebral junction abnormalities and the type of abnormalities ……… 12 Fig 3. Correlation between cervico-mandibular angle and degrees of each craniovertebral junction abnormalities among subjects who underwent surgery………13
List of Tables
Table 1. Characteristics of the subjects………9 Table 2. Inter-rater reliability of measurements of craniovertebral junction abnormalities and the severity of congenital muscular torticollis ……… 10 Table 3. Types of craniovertebral junction abnormalities among the subjects with congenital muscular torticollis ……… 11
- 1 -
I.
INTRODUCTION
Congenital muscular torticollis (CMT) is the third most common musculoskeletal disease among newborns after clubfoot and developmental dysplasia of the hip (Cheng and Au 1994; Cheng et al., 2000; Dobbs and Gurnett, 2009; Loder and Skopelja, 2011). CMT is characterized by thickening and/or tightness of the unilateral sternocleidomastoid (SCM) muscle, with limited motion of the neck (Hwang et al., 2012). Most subjects with CMT can be treated with physical therapy, however, some cases require a surgical release of the SCM to minimize secondary complications, such as cervical and thoracolumbar scoliosis, deformational plagiocephaly, and various forms of facial asymmetry (Binder et al., 1987; Canale, Griffin and Hubbard 1982; Chate, 2004; Cheng et al., 2001; Holier et al., 2000; Jeong et al., 2015; Kim, Ahn and Yim 2015; Kuo, Tritasavit and Graham, 2014; Ozer et al., 2004; Rogers, Oh and Mulliken, 2009; Yu et al., 2004). These skeletal deformities may progress if the contracted SCM is not released (Holier et al., 2000; Seo et al., 2013). Therefore, physicians must make timely decision for surgery. Findings indicating need of surgery include palpable cord-like unilateral SCM, significant limited motion of the neck despite adequate physical therapy, significant craniofacial asymmetry, evident spinal deformities, and extensive unilateral fibrosis within the SCM seen on magnetic resonance imaging (MRI) (Cheng and Tang, 1999; Hwang et al., 2012; Lee, Kang and Bose 1986).
The craniovertebral junction (CVJ) is a complex region that incorporates the occiput, the atlas, the axis, adjacent ligaments, and neurovascular structures. The CVJ is the most mobile region of the cervical spines and plays an important role in posture and neck movement (Martin, Bruner and Maiman, 2010; Steinmetz, Mroz and Benzel, 2010). In our clinical experience, we observed that some subjects with CMT have CVJ abnormalities on craniofacial computed tomography. A review of available literature revealed only two retrospective studies about concurrent CVJ abnormalities in subjects with CMT. Ozer et al. reported that rotation of the atlanto-axial joint (AAJ) was found in all cases (6 subjects) with CMT (Ozer et al., 2004). Slate et al. reported that 13 of 26 subjects with CMT showed rotation of the AAJ (Slate et al., 1993). However, these two studies had a small sample, provided no information regarding other types of CVJ abnormalities, and did not discuss clinical implications of concurrent CVJ abnormalities
- 2 - in subjects with CMT.
CVJ abnormalities in CMT may occur due to the chronic mechanical force generated by the tight unilateral SCM and might reflect severe CMT. The objectives of this study were (1) to present a variety of concurrent CVJ abnormalities in patients with CMT and (2) to examine the relationship between CVJ abnormalities and clinical severity of CMT.
- 3 -
II.
SUBJECTS AND METHODS
This retrospective study was conducted in a tertiary medical center. Approval was granted by the Institutional Review Board of Ajou Medical center (AJIRB-MED-MDB-15-018).
A. Enrollment
We retrospectively reviewed medical records and radiological findings of patients who visited the Center for Torticollis for an abnormal posture of head and neck between March 2014 and January 2015. Those who met all of the following criteria were enrolled into the study: (1) diagnosis of CMT; (2) significant tightness or thickening of the unilateral SCM with ipsilateral head tilting and/or rotation of the chin toward the contralateral side which resulted in limitation of passive rotation of the neck toward the involved side, despite adequate physical therapy; and (3) availability of neck MRI and craniofacial three-dimensional volume-rendered computed tomographic image (3D-CT) which provided an adequate view for evaluation of the CVJ.
Exclusion criteria were as follows: (1) abnormal posture of the head and neck associated with neurodevelopmental disorders; (2) anomalies of formation and segmentation of cervical spines; (3) craniosynostosis; (4) history of head and neck trauma; (5) history of surgery for CMT; and (6) abnormal posture of head and neck caused by ocular disorders such as unilateral superior oblique palsy.
CMT was diagnosed when at least one of following two conditions were met: (1) large or multiple low signal intensities within the involved SCM in MRI (Hwang et al., 2012); (2) thickness of the SCM of the involved side >2mm than that of the contralateral side, along with increased echogenicity, on ultrasonography (Yim et al., 2010).
B. Collection of Demographic Data
Characteristics such as age, sex, affected side of CMT, and whether subjects underwent surgery for CMT were gathered from medical chart reviews.
C. Acquisition of Craniofacial 3D-CT and Neck MRI
- 4 -
had obvious craniofacial deformities and limited motion of the neck at the age of 4 months or older, despite adequate physical therapy. All subjects underwent a craniofacial 3D-CT and neck MRI in a single medical center with the same protocol.
A craniofacial 3D-CT was performed with a multi-detector row helical CT (Philips, Eindhoven, Netherlands) (scan parameters: 120kVp, 50–80mAs, scan time: 4–6ms, section thickness: 3mm, matrix size: 512×512). CT scans from the vertex to the C3 body were used for measurements. The neck MRI was performed using a 1.5-T MRI unit (Signa, GE Medical Systems, Milwaukee, WI, USA) or a 3.0-T MRI unit (Achieva, Philips, Amsterdam,
Netherlands) (scan parameters: TR/TE, 400–600/11–14 for T1-weighted imaging and 3,000– 4,000/75–100 for T2- weighted imaging, section thickness: 3.0–6.0mm, slice gap: 1–2.5mm, and FOV 180–240mm depending on the body side and section planes). The MRI and CT scans were reviewed with a PiView STAR program (Infinitt, Seoul, Korea). The subjects’ body was pressed flat against the table to maintain a 0-degree plane during the MRI and CT.
D. Analysis of the Severity of CMT
A quantitative analysis of laterocollis, plagiocephaly, and MRI findings of CMT was conducted in terms of the cervico-mandibular angle (CMA), cranial vault asymmetry index (CVAI), and ratio of intensity, respectively. These were considered to represent the severity of CMT. Measurements were taken by physicians who had no knowledge of subject status.
CMA was measured to evaluate degree of lateral head tilting from an antero-posterior radiograph of cervical spines. It was defined as the angle between a line along the upper border of the C7 vertebral body and the line connecting bilateral mandibular angles (Shim and Jang, 2008; Lim, Shim and Lee, 2014).The presence of laterocollis was defined as a CMA of greater than 5 degrees. Laterocollis was classified as mild (5 ≤ CMA < 10), moderate (10 ≤ CMA < 15) or severe (CMA ≥ 15).
CVAI was measured on the axial image of craniofacial 3D-CT (Loveday and de Chalain, 2001; Wilbrand et al., 2012). CVAI was calculated as follows: (the maximum difference between the longer diagonal and the shorter diagonal)/shorter diagonal×100. The presence of plagiocephaly was defined as a CVAI value of greater than 3.5 percent. Plagiocephaly was categorized as mild (3.5 < CVAI ≤ 7), moderate (7 < CVAI ≤ 12), and severe (CVAI > 12).
- 5 -
neck MRI (Hwang et al., 2012). The lowest mean gray color intensity was measured in the SCM with CMT on the axial T1-weighted image. The mean gray color intensity was also measured in the contralateral SCM at the same level. The ratio of intensity was calculated as follows: (the mean gray color intensity of the SCM without CMT − the lowest mean gray color intensity of the SCM with CMT)/the mean gray color intensity of the SCM without CMT×100. A ratio of intensity above 0.05 percent was regarded as clinically significant fibrosis (Kim et al, 2015).
E. Analysis of CVJ Abnormalities
Analysis used axial images of craniofacial 3D-CT as they had an adequate view of the CVJ. Two physicians, who had no knowledge of subject status, took measurements of CVJ
abnormalities independently. The anatomical landmarks for measurements are shown in Fig 1. A quantitative analysis of CVJ abnormalities was made as follows.
- 6 -
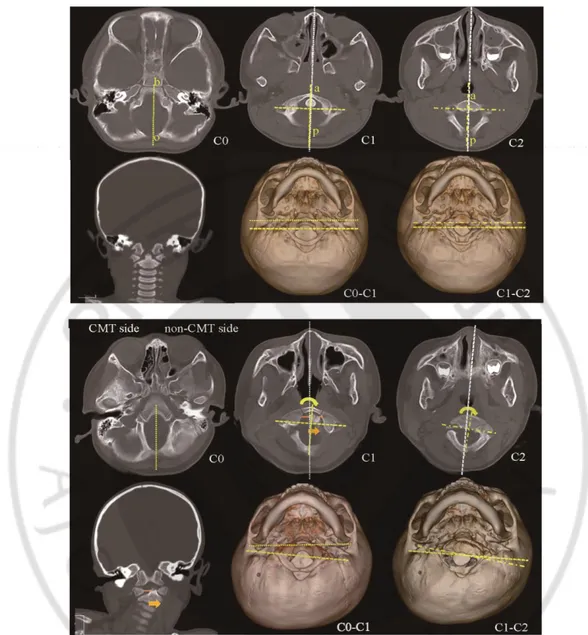
Fig 1. Craniofacial computed tomography (CT) of the age-matched control and the patient with congenital muscular torticollis (CMT).
(above) CT scans of 48-month-old boy without CMT show no craniovertebral junction abnormality. (b) basion; (o) opisthion; (a) the anterior tubercle of the atlas (C1) and the axis (C2); (p) the posterior tubercle of the atlas and the axis; (C0) the occiput.
(below) CT scans of 46-month-old boy with right CMT show rotation of the atlanto-occipital joint (curved arrow), rotation of the atlanto-axial joint (curved arrow) and lateral shift of the atlanto-axial joint (straight arrow). The sagittal midline of the atlas (the less densely dotted lines) is rotated toward contralateral side of CMT in relation to the sagittal midline of the occiput (the
- 7 -
most densely dotted lines). The sagittal midline of the axis (the most scattered dotted lines) is
rotated toward the contralateral side of CMT in relation to the sagittal midline of the atlas. The dens is shifted toward the contralateral side of CMT.
1. Rotation of the Atlanto-Occipital Joint (AOJ)
The presence of rotation of the AOJ was defined as an atlanto-occipital rotational angle of greater than 3 degrees (Pang and Li, 2004; Pang and Li, 2005).The atlanto-occipital rotational angle is the angle between the midline of the occiput and the midline of the atlas. The sagittal midline of the occiput was drawn between the basion and the opisthion of foramen magnum. The sagittal midline of the atlas was drawn using one of following two methods, depending on visibility of anatomical structures: 1) The midline was drawn between the anterior and posterior tubercles of the atlas; 2) The midline was drawn as the perpendicular that bisected the line joining transverse foramina of the atlas.
2. Rotation of the AAJ
The presence of rotation of the AAJ was defined as an atlanto-axial rotational angle of more than 5 degrees. The atlanto-axial rotational angle was defined as the angle between the line joining transverse foramina of the atlas and the line joining transverse foramina of the axis (Duan, Ye and Kang, 2007).
3. Lateral Shift of the AAJ
Lateral shift of the AAJ was defined as lateral shift of the dens of more than 2mm. Lateral shift of the dens was measured as |right lateral atlanto-dens interval − left lateral atlanto-dens interval| (Sutherland, Taszemski and White 1995; Wolansky et al., 1999).
4. Anterior Shift of the AAJ
Anterior shift of the AAJ was defined as anterior shift of the dens of more than 5mm. The anterior atlanto-dens interval was measured for anterior shift of the dens between the dens and anterior ring of the atlas (Locke, Gardner and Van 1966).
- 8 -
Pearson correlations were performed to assess the relation between degrees of CVJ abnormalities and the clinical severity of CMT. The intra-class correlation coefficients (ICC) between two investigators were calculated for inter-rater reliability for all measurements. The ICC was interpreted as follows: 1.0, perfect agreement; 0.81–0.99, almost perfect agreement; 0.61–0.80, substantial agreement; 0.41–0.60, moderate agreement; 0.21–0.40, fair agreement; and ≤0.20, slight agreement. After assessing inter-rater reliability, we used mean values measured by two raters for analysis. P-value <0.05 was considered statistically significant.
- 9 -
III. RESULTS
A. Characteristics of the Subjects
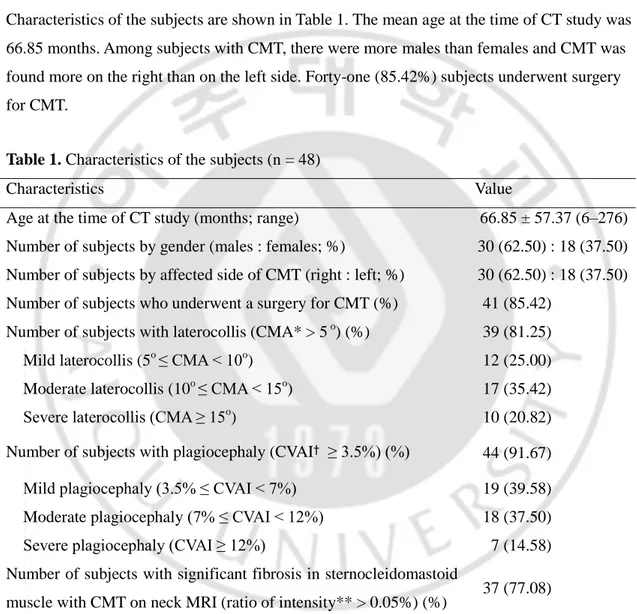
Forty-eight subjects (30 males and 18 females) meeting the inclusion criteria were enrolled. Characteristics of the subjects are shown in Table 1. The mean age at the time of CT study was 66.85 months. Among subjects with CMT, there were more males than females and CMT was found more on the right than on the left side. Forty-one (85.42%) subjects underwent surgery for CMT.
Table 1. Characteristics of the subjects (n = 48)
Characteristics Value
Age at the time of CT study (months; range) 66.85 ± 57.37 (6–276)
Number of subjects by gender (males : females; %) 30 (62.50) : 18 (37.50)
Number of subjects by affected side of CMT (right : left; %) 30 (62.50) : 18 (37.50)
Number of subjects who underwent a surgery for CMT (%) 41 (85.42)
Number of subjects with laterocollis (CMA* > 5 o) (%) 39 (81.25)
Mild laterocollis (5o ≤ CMA < 10o) 12 (25.00)
Moderate laterocollis (10o ≤ CMA < 15o) 17 (35.42)
Severe laterocollis (CMA ≥ 15o
) 10 (20.82)
Number of subjects with plagiocephaly (CVAI† ≥ 3.5%) (%) 44 (91.67)
Mild plagiocephaly (3.5% ≤ CVAI < 7%) 19 (39.58)
Moderate plagiocephaly (7% ≤ CVAI < 12%) 18 (37.50)
Severe plagiocephaly (CVAI ≥ 12%) 7 (14.58)
Number of subjects with significant fibrosis in sternocleidomastoid
muscle with CMT on neck MRI (ratio of intensity** > 0.05%) (%) 37 (77.08) All values are expressed as means ± standard deviation or numbers
CT, craniofacial three-dimensional volume-rendered computed tomographic image; CMT, congenital muscular torticollis
* CMA, cervico-mandibular angle = the angle between the line along the upper border of the C7 spine and the lines connecting the lower borders of both mandibles
- 10 -
† CVAI, cranial vault asymmetry index = (the biggest difference between longer diagonal and shorter diagonal)/shorter diagonal × 100 on the axial image of craciofacial 3D-CT
** Ratio of intensity = (The mean gray color intensity of the contralateral sternocleidomastoid without CMT – the lowest mean gray color intensity of sternocleidomastoid with CMT) / the mean gray color intensity of the contralateral sternocleidomastoid without CMT × 100
B. Inter-rater Reliability of Measurements
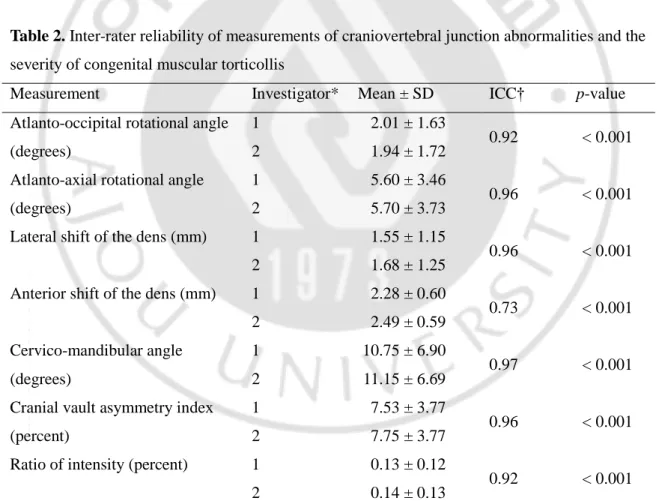
The ICC values of measurements of CVJ abnormalities and the severity of CMT are presented in Table 2. The ICC values of all measurements were higher than 0.70, suggesting almost perfect or substantial inter-rater reliability (p<0.001).
Table 2. Inter-rater reliability of measurements of craniovertebral junction abnormalities and the severity of congenital muscular torticollis
Measurement Investigator* Mean ± SD ICC† p-value
Atlanto-occipital rotational angle (degrees)
1 2.01 ± 1.63
0.92 < 0.001
2 1.94 ± 1.72
Atlanto-axial rotational angle (degrees)
1 5.60 ± 3.46
0.96 < 0.001
2 5.70 ± 3.73
Lateral shift of the dens (mm) 1 1.55 ± 1.15
0.96 < 0.001
2 1.68 ± 1.25
Anterior shift of the dens (mm) 1 2.28 ± 0.60
0.73 < 0.001 2 2.49 ± 0.59 Cervico-mandibular angle (degrees) 1 10.75 ± 6.90 0.97 < 0.001 2 11.15 ± 6.69
Cranial vault asymmetry index (percent)
1 7.53 ± 3.77
0.96 < 0.001
2 7.75 ± 3.77
Ratio of intensity (percent) 1 0.13 ± 0.12
0.92 < 0.001
2 0.14 ± 0.13
*Investigator 1: ARA, 2: JEW
- 11 -
agreement; 0.81–0.99, almost perfect agreement; 0.61–0.80, substantial agreement; 0.41–0.60, moderate agreement; 0.21–0.40, fair agreement; and ≤0.20, slight agreement.
C. Analysis of the Severity of CMT
Results of a quantitative analysis for the severity of CMT are shown in Table 1. Thirty-nine (81.25%) subjects had laterocollis and mean CMA was 10.97 degrees. Forty-four (91.7%) subjects had plagiocephaly and mean CVAI was 7.61 percent. Thirty-seven (77.08%) subjects had significant fibrosis in the SCM on the side with CMT and the mean ratio of intensity was 0.13 percent.
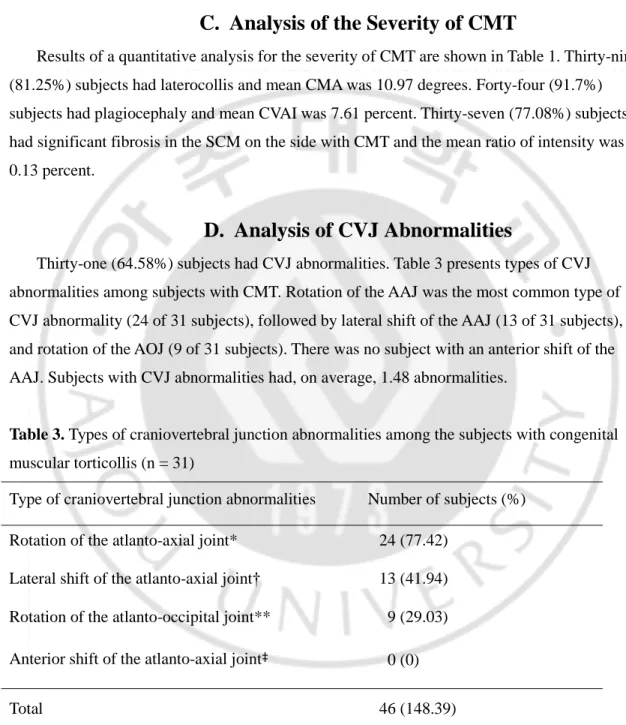
D. Analysis of CVJ Abnormalities
Thirty-one (64.58%) subjects had CVJ abnormalities. Table 3 presents types of CVJ abnormalities among subjects with CMT. Rotation of the AAJ was the most common type of CVJ abnormality (24 of 31 subjects), followed by lateral shift of the AAJ (13 of 31 subjects), and rotation of the AOJ (9 of 31 subjects). There was no subject with an anterior shift of the AAJ. Subjects with CVJ abnormalities had, on average, 1.48 abnormalities.
Table 3. Types of craniovertebral junction abnormalities among the subjects with congenital muscular torticollis (n = 31)
Type of craniovertebral junction abnormalities Number of subjects (%)
Rotation of the atlanto-axial joint* 24 (77.42)
Lateral shift of the atlanto-axial joint† 13 (41.94)
Rotation of the atlanto-occipital joint** 9 (29.03)
Anterior shift of the atlanto-axial joint‡ 0 (0)
Total 46 (148.39)
* atlanto-axial rotational angle >5 degrees
- 12 - ** atlanto-occipital rotational angle >3 degrees ‡ anterioratlanto-dens interval >5 mm
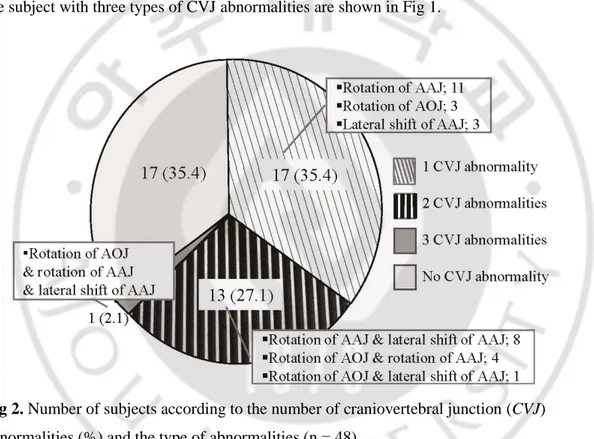
Fig 2 presents number of subjects according to the number of CVJ abnormalities and the type of abnormalities. Thirty-one (64.58%) subjects had one or more types of CVJ
abnormalities. Seventeen (35.42%) subjects had a single CVJ abnormality, thirteen (27.08%) subjects had two abnormalities, and one (2.08%) subject had three abnormalities. CT scans of the subject with three types of CVJ abnormalities are shown in Fig 1.
Fig 2. Number of subjects according to the number of craniovertebral junction (CVJ) abnormalities (%) and the type of abnormalities (n = 48)
(AAJ) atlanto-axial joint; (AOJ) atlanto-occipital joint.
In 23 of 24 (95.83%) subjects with rotation of the AAJ, the sagittal midline of the atlas was rotated toward the contralateral side of CMT in relation to the sagittal midline of the atlas (Fig. 1). The dens had shifted toward the contralateral side of CMT in all subjects with lateral shift of the AAJ. In 8 of the 9 (88.89%) subjects with rotation of the AOJ, the sagittal midline of the atlas was rotated toward the contralateral side of CMT in relation to the sagittal midline of the occiput.
- 13 -
Among subjects with CVJ abnormalities, 29 of 31 (93.5%) subjects underwent surgery, whereas only 12 of 17 (70.6%) of subjects without CVJ abnormalities underwent surgery. The two subjects with CVJ abnormalities who did not undergo surgery, a 14-month-old girl and a 16-month-old girl, are under close observation for a surgical decision.
E. Correlation between Degrees of CVJ Abnormalities with the
Severity of CMT
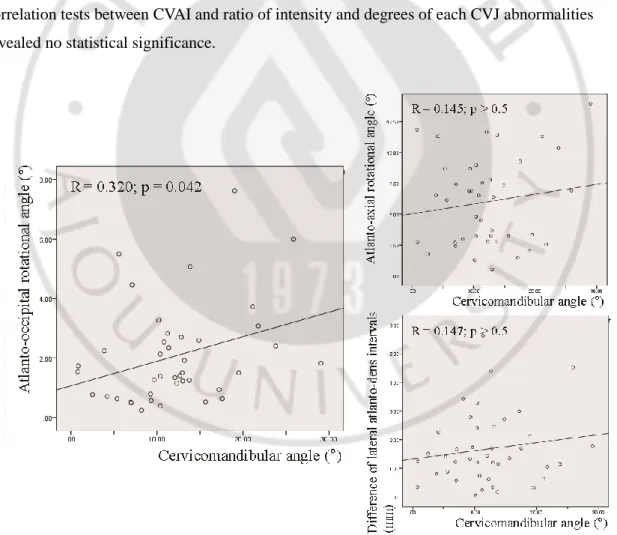
Fig 3 shows the results of correlation tests between CMA and degrees of each of the CVJ abnormalities among 41 subjects who underwent surgery. A significant positive correlation was found between CMA and atlanto-occipital rotational angle (r=0.32; p<0.05). However,
correlation tests between CVAI and ratio of intensity and degrees of each CVJ abnormalities revealed no statistical significance.
Fig 3. Correlation between cervico-mandibular angle and degrees of each craniovertebral junction abnormalities among subjects who underwent surgery (n = 41)
- 14 -
IV. DISCUSSION
The current study reported concurrent CVJ abnormalities in subjects with CMT. Two-thirds of subjects with CMT had one or more types of CVJ abnormalities per quantitative analysis of craniofacial 3D-CT. The quantitative analysis also demonstrated the association between degrees of CVJ abnormalities and the severity of CMT.
This study has several strengths. First is the comprehensive assessment of various CVJ abnormalities. No previous study examined rotation of the AOJ and lateral shift of the AAJ in subjects with CMT. The most common type of CVJ abnormalities in this study was rotation of the AAJ. Fifty percent of subjects had rotation of the AAJ, a finding in line with Slate et al’s report (Slate et al., 1993). Lateral shift of the AAJ was found in 27 percent of subjects, and no subject had anterior shift of the AAJ. Rotation of the AOJ was found in 18 percent of subjects. Rotation of the AOJ might represent laxity of the AOJ, which should be nearly fixed in healthy children. Atlanto-occipital rotational angle in normal children is reported not to exceed 3 degrees by dynamic CT scans in the physiological axial rotation (Pang and Li, 2004). Considering that atlanto-occipital rotational angle was measured with neutral head posture, laxity of the AOJ could be more frequent and severe than reported.
Second, the direction of rotation and shift of cervical spines in subjects was demonstrated with CMT. Lower vertebral segments tended to be rotated or shifted toward the contralateral side of CMT in relation to the occiput. It seems that more movable segments are rotated or shifted to relatively fixed segments; however, these findings require further evaluation.
Third, this study suggests clinical implications of concurrent CVJ abnormalities in subjects with CMT. The quantitative analysis also demonstrated the association between degrees of CVJ abnormalities and the severity of CMT, showing a positive correlation between CMA and atlanto-occipital rotational angle. In subjects with CMT, the chronic mechanical force generated by the tightened SCM might lead to a rotation or shift of cervical spines. Therefore, the
existence of CVJ abnormalities could relate to the severity of CMT.
In this study, 85 percent of subjects underwent surgery for CMT, whereas previous literature reports that approximately 10 percent of subjects need surgical treatment (Cheng et al, 2001; Wei et al., 2001).The Center for Torticollis is a specialized medical facility where subjects who
- 15 -
do not show satisfactory response to physical therapy are referred for further management from across the nation in South Korea. Based on previous studies in the Center for Torticollis, neck MRIs were obtained for approximately 35 percent of subjects with CMT, for whom surgical decisions were considered, and 57 percent of them underwent surgery (Kim et al., 2015). According to unreported data, approximately 25 percent of subjects who visited the Center for Torticollis underwent surgery. The high rate of surgical treatment in this study is likely due to the characteristic roles of the Center for Torticollis in South Korea.
There are several limitations of this study. First, while superficially this may seem like a small data set, subject to issues with low statistical power, compared to the number of subjects undergoing surgery for CMT in the general population of South Korea, this sample size is considerable. Second, a selection bias may have been present, as participants were enrolled from one tertiary medical center with a high rate of a surgical intervention. Third limitation is the risk of measurement bias. However, measurements were conducted using obvious anatomical landmarks and inter-rater reliability was high according to ICC values obtained. Fourth, only imaging parameters were used to assess the severity of CMT. There was also no information about the range of motion of the neck. This may explain a lack of obvious evidence for the relationship between the severity of CMT and degrees of CVJ abnormalities. Finally, the time of development and maturation of the CVJ was not taken into consideration for the analysis due to the small sample size. The atlantal ring is known to complete by about 4–7 years, and the neural arch axis is completed by 3 years (Raybaud, 2011; Ghanem et al., 2008). Future studies are needed to categorize subjects into subgroups according to their age, considering the developmental period of the CVJ.
- 16 -
V. CONCLUSION
The overall results must be interpreted with a degree of caution. However, even with these limitations, this appears to be the first documented study where subjects with CMT also presented with various types of CVJ abnormalities. CVJ abnormalities are common concurrent skeletal deformities in patients with CMT and presence of CVJ abnormalities may indicate the severe severity of CMT. Further prospective studies are required to verify these findings.
- 17 -
REFERENCES
1. Binder H, Eng GD, Gaiser JF, Koch B. Congenital muscular torticollis: results of
conservative management with long-term follow-up in 85 cases. Arch Phys Med Rehabil. 1987;68:222-225.
2. Canale ST, Griffin DW, Hubbard CN. Congenital muscular torticollis. A long-term follow-up. J Bone Joint Surg Am. 1982;64:810-816.
3. Chate RA. Facial scoliosis due to sternocleidomastoid torticollis: a cephalometric analysis. Int J Oral Maxillofac Surg. 2004;33:338-343.
4. Cheng JC, Au AW. Infantile torticollis: a review of 624 cases. J Pediatr Orthop. 1994;14:802-808.
5. Cheng JC, Tang SP, Chen TM, Wong MW, Wong EM. The clinical presentation and outcome of treatment of congenital muscular torticollis in infants--a study of 1,086 cases. J Pediatr Surg. 2000;35:1091-1096.
6. Cheng JC, Tang SP. Outcome of surgical treatment of congenital muscular torticollis. Clin Orthop Relat Res. 1999:190-200.
7. Cheng JC, Wong MW, Tang SP, Chen TM, Shum SL, Wong EM. Clinical determinants of the outcome of manual stretching in the treatment of congenital muscular torticollis in infants. A prospective study of eight hundred and twenty-one cases. J Bone Joint Surg Am. 2001;83-A:679-687.
8. Dobbs MB, Gurnett CA. Update on clubfoot: etiology and treatment. Clin Orthop Relat Res. 2009;467:1146-1153.
9. Duan S, Ye F, Kang J. Three-dimensional CT study on normal anatomical features of atlanto-axial joints. Surg Radiol Anat. 2007;29:83-88.
10. Ghanem I, El Hage S, Rachkidi R, Kharrat K, Dagher F, Kreichati G. Pediatric cervical spine instability. J Child Orthop. 2008;2:71-84
11. Hollier L, Kim J, Grayson BH, McCarthy JG. Congenital muscular torticollis and the associated craniofacial changes. Plast Reconstr Surg. 2000;105:827-835.
12. Hwang JH, Lee HB, Kim JH, Park MC, Kwack KS, Han JD, Yim SY. Magnetic resonance imaging as a determinant for surgical release of congenital muscular torticollis: correlation
- 18 -
with the histopathologic findings. Ann Rehabil Med. 2012;36:320-327.
13. Jeong KY, Min KJ, Woo J, Yim SY. Craniofacial Asymmetry in Adults With Neglected Congenital Muscular Torticollis. Ann Rehabil Med. 2015;39:440-450.
14. Kim HJ, Ahn HS, Yim SY. Effectiveness of Surgical Treatment for Neglected Congenital Muscular Torticollis: A Systematic Review and Meta-Analysis. Plast Reconstr Surg. 2015;136:67e-77e.
15. Kim JW, Kim SH, Yim SY. Quantitative analysis of magnetic resonance imaging of the neck and its usefulness in management of congenital muscular torticollis. Ann Rehabil Med. 2015;39:294-302.
16. Kuo AA, Tritasavit S, Graham JM, Jr. Congenital muscular torticollis and positional plagiocephaly. Pediatr Rev. 2014;35:79-87.
17. Lee EH, Kang YK, Bose K. Surgical correction of muscular torticollis in the older child. J Pediatr Orthop. 1986;6:585-589.
18. Lim KS, Shim JS, Lee YS. Is sternocleidomastoid muscle release effective in adults with neglected congenital muscular torticollis? Clin Orthop Relat Res. 2014;472:1271-1278. 19. Locke GR, Gardner JI, Van Epps EF. Atlas-dens interval (ADI) in children: a survey based
on 200 normal cervical spines. Am J Roentgenol Radium Ther Nucl Med. 1966;97:135-140. 20. Loder RT, Skopelja EN. The epidemiology and demographics of hip dysplasia. ISRN
Orthop. 2011;2011:238607.
21. Loveday BP, de Chalain TB. Active counterpositioning or orthotic device to treat positional plagiocephaly? J Craniofac Surg. 2001;12:308-313.
22. Martin MD, Bruner HJ, Maiman DJ. Anatomic and biomechanical considerations of the craniovertebral junction. Neurosurgery. 2010;66:2-6.
23. Ozer T, Uzun L, Numanoglu V, Savranlar A, Hosnuter M, Gundogdu S. 3D-CT
investigation of craniofacial and cervical spine anomalies in congenital muscular torticollis. Tani Girisim Radyol. 2004;10:272-279.
24. Pang D, Li V. Atlantoaxial rotatory fixation: Part 1--Biomechanics of normal rotation at the atlantoaxial joint in children. Neurosurgery. 2004;55:614-625.
25. Pang D, Li V. Atlantoaxial rotatory fixation: part 3-a prospective study of the clinical manifestation, diagnosis, management, and outcome of children with alantoaxial rotatory fixation. Neurosurgery. 2005;57:954-972.
- 19 -
26. Raybaud C. Anatomy and development of the craniovertebral junction. Neurol Sci. 2011;Suppl 3:S267-70.
27. Rogers GF, Oh AK, Mulliken JB. The role of congenital muscular torticollis in the development of deformational plagiocephaly. Plast Reconstr Surg. 2009;123:643-652. 28. Seo SJ, Yim SY, Lee IJ, Han DH, Kim CS, Lim H, Park MC. Is craniofacial asymmetry
progressive in untreated congenital muscular torticollis? Plast Reconstr Surg. 2013;132:407-413.
29. Shim JS, Jang HP. Operative treatment of congenital torticollis. J Bone Joint Surg Br. 2008;90:934-939.
30. Slate RK, Posnick JC, Armstrong DC, Buncic JR. Cervical spine subluxation associated with congenital muscular torticollis and craniofacial asymmetry. Plast Reconstr Surg. 1993;91:1187-1195.
31. Steinmetz MP, Mroz TE, Benzel EC. Craniovertebral junction: biomechanical considerations. Neurosurgery. 2010;66:7-12.
32. Sutherland JP, Jr., Yaszemski MJ, White AA, 3rd. Radiographic appearance of the odontoid lateral mass interspace in the occipitoatlantoaxial complex. Spine. 1995;20:2221-2225.
33. Wei JL, Schwartz KM, Weaver AL, Orvidas LJ. Pseudotumor of infancy and congenital muscular torticollis: 170 cases. Laryngoscope. 2001;111:688-695.
34. Wilbrand JF, Wilbrand M, Malik CY, Howaldt HP, Streckbein P, Schaaf H, Kerkmann H. Complications in helmet therapy. J Craniomaxillofac Surg. 2012;40:341-346.
35. Wolansky LJ, Rajaraman V, Seo C, Patel N, Kazmi K, Doddakashi S, Siegel S. The lateral atlanto-dens interval: normal range of asymmetry. Emerg Radiol. 1999;6:290-293.
36. Yim SY, Lee IY, Cho KH, Kim JK, Lee IJ, Park MC. The laryngeal cough reflex in congenital muscular torticollis: is it a new finding? Am J Phys Med Rehabil. 2010;89:147-152.
37. Yu CC, Wong FH, Lo LJ, Chen YR. Craniofacial deformity in subjects with uncorrected congenital muscular torticollis: an assessment from three-dimensional computed
- 20 - - 국문 요약 -