Vol. 11, No. 4, December, 2004
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
<접수일:2004년 9월 30일, 심사통과일:2004년 10월 21일>
※통신저자:전 재 범
서울특별시 성동구 행당동 17번지
한양대학교 의과대학 내과학교실, 류마티스병원
Tel:02) 2290-9244, Fax:02) 2298-8231, E-mail:[email protected]
강직성 척추염 환자에서 골밀도 측정의 임상적 의의
한양대학교 의과대학 내과학교실, 류마티스병원, 종합검진센터*, 핵의학교실**, 진단방사선과***
왕준광․박의순․이혜순․엄완식․김태환․배상철 유대현․안유헌*․최윤영**․주경빈***․전재범
= Abstract =
The Clinical Significance of Bone Mineral Density Measurement in Patients with Ankylosing Spondylitis
Joon-Kwang Wang, M.D., Ui-Soon Park, M.D., Hye-Soon Lee, M.D., Wan-Sik Uhm, M.D., Tae-Hwan Kim, M.D., Sang-Cheol Bae, M.D., Dae-Hyun Yoo, M.D., You-Hern Ahn, M.D.*, Yun-Young Choi, M.D.**,
Kyung-Bin Joo, M.D.***, Jae-Bum Jun, M.D.
Department of Internal Medicine, The Hospital for Rheumatic Diseases, Health Promotion Center*, Department of Nuclear Medicine**, Department of Radiology***, Hanyang University, Seoul, Korea
Objective: Decrease in bone mineral density (BMD) occurs relatively early and is known to be correlated with disease activity in patients with ankylosing spondylitis (AS). We investigated BMD and its correlation factors in Korean patients with AS.
Methods: Fifty patients with AS fulfilling modified New York criteria and age-, sex-, and body mass index-matched 100 normal controls were selected. Medical records were reviewed retrospectively. Lumbar and femur BMD was measured using a dual energy X-ray absor- ptiometry.
Results: Both lumbar and femur BMD in patients with AS were significantly lower than BMD in control group. Although Bath ankylosing spondylitis disease activity index, C-reactive protein and erythrocyte sedimentation rate showed no correlation with BMD, lumbar BMD in patients
서 론
강직성 척추염은 HLA-B27과 연관된 만성 염증성 질환으로 그 원인은 아직 정확히 밝혀지지 않았다1). 주로 천장관절과 중추골격을 침범하지만, 말초관절 에도 침범하며 급성 포도막염, 대동맥 기능부전, 심 장 전도 장애, 폐섬유화, 신경학적 질환, 신장 아밀 로이드증 등 골격계 외의 질환을 일으키기도 한다.
골격계에는 골밀도가 감소하여 골다공증이 생기는 데, 이를 1877년 Fagge2)가 처음으로 보고하였다. 강 직성 척추염 환자들은 만성적인 염증에 의해서 정상 인보다 골밀도의 감소가 비교적 이른 시기부터 나타 나고3), 골다공증에 의한 척추 골절이 정상군에 비해 더 많이 발생한다고 알려져 있다4). 1999년 Meirelles 등5)은 강직성 척추염 환자에서 질병의 활성도가 높 은 군이 낮은 군보다 골밀도의 감소가 더 심하여 질 병의 활성도가 골밀도에 많은 영향을 주는 것으로 보고하였다. 2001년 Maillefert 등6)은 2년 동안 코호 트 연구를 통하여 지속적으로 염증 활성도가 높은 군이 낮은 군보다 골밀도가 더 낮아, 염증 자체가 골밀도 저하를 일으키는 것으로 보고한 바 있다6). 이처럼 강직성 척추염의 만성 염증이 골밀도를 감 소시키는 것으로 보고되고 있으나, 국내에서는 아직 이에 대한 연구가 미미한 상태이다. 이에 한국인 강 직성 척추염 환자에 있어서 골밀도의 감소여부, 각 부위별 골밀도의 차이, 골밀도와의 상관관계가 있는 인자들을 조사하고, 질병의 활성도와 방사선학적 중 증도에 따라 요추부와 대퇴부의 골밀도의 차이를 조 사하였다.
대상 및 방법 1. 대상
2003년 3월부터 2003년 10월 사이에 류마티스내과 외래에 연속적으로 내원한 modified New York cri- teria7,8)에 합당한 강직성 척추염 환자 중에서 평가에 동의한 50명을 대상으로 하였다. 폐경기 여성, 간질 환, 신장질환, 부갑상선질환, 요추 및 대퇴골 부위의 외상 및 골절 병력이 있는 자는 대상에서 제외하였 다. 대조군은 같은 시기에 건강검진을 위해 건강검 진센타에 내원한 피검자로, 골밀도에 영향을 주는 질환이 없으며, 나이, 성별, 신체비만지수를 1대 2로 일치시킨 100명을 대상으로 하였다.
2. 방법
1) 임상적 평가: 나이, 성별, 체중, 신장, 신체비만 지수, 질병 이환 기간, 스테로이드 복용량은 차트를 통하여 후향적으로 조사하였다. 스테로이드 복용량 은 ‘prednisolone 5 mg의 동등량×개월’을 한 ‘단위’
로 표시하였다. 척추의 가동성을 나타내는 이학적 검사로 modified Schober's test9), finger to ground test 를 조사하였고, Bath ankylosing spondylitis disease activity index (BASDAI)를 조사하였다. BASDAI는 배 등10)이 한글로 번역하여 통계적으로 유의성이 입 증된 설문지를 사용하였고, 각 6가지의 문항에 대해 0∼10씩 점수화하여 이에 대한 합을 이용하였다11). 2) 혈액검사적 평가: 염증의 활성도를 보기 위해 C-반응단백(C-reactive protein; CRP)과 적혈구침강속 도(erythrocyte sedimentation rate, ESR, Westergren법) 를 측정하였다. CRP, ESR과 골밀도의 상관관계를 조사하였고, 각각 CRP가 1.4 mg/dL 이상인 군, ESR 이 15 mm/hr 이상인 군을 염증의 활성도가 높은 군 으로, 그 미만은 염증의 활성도가 낮은 군으로 나누 with high disease activity in terms of inflammatory factors was significantly lower than that in patients with low disease activity.
Conclusion: BMD in patients with AS was significantly lower than those in control group. Early detection and appropriate management will be necessary in patients with AS.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: Ankylosing spondylitis, Bone mineral density
어 골밀도를 비교하였다12). HLA-B27은 혈청형별 검 사법으로 검사하였다.
3) 방사선적 평가: Bath ankylosing spondylitis ra- diological index (BASRI)는 방사선학적으로 강직성 척추염의 진행 정도를 나타낸 것으로, 경추, 요추, 천장관절의 세 곳의 점수로 세분화하여 나타낼 수 있는데 본 연구에서는 요추부위를 점수화하였다. 판 독은 근골격계 방사선판독에 10년 이상 경력이 있는 진단방사선과 전문의가 하였고, picture archiving and communication system (PACS, Piview STARTM, INFINITT Technology Co., Ltd., Seoul, Korea)을 이용 하여 판독하였다. 요추의 전후방, 측방 단순사진을 판독하여 0에서 4까지 점수화하였다13). 방사선학적 중증도는 BASRI의 점수에 따라 0∼1점은 초기군, 2∼4점은 진행군으로 나누어14), 두 군의 골밀도의 차이를 조사하였다.
4) 골밀도의 평가: 골밀도는 요추부(제2∼제4요추) 와 왼쪽 대퇴골부(목, 큰돌기, 돌기사이, 워드 삼각 부)를 측정하였고, 실험군은 dual energy X-ray absor- ptiometry (QDR 4500A, Hologic Inc, Waltharn, USA) 로, 대조군은 dual energy X-ray absorptiometry (Delphi W, Hologic Inc, Philadelphia, USA)로 측정하였다. 같 은 회사의 동종기종이므로 양측 기계의 오차는 모형 으로 20번 측정하여 구한 상수(QDR=Delphi×1.007) 를 이용하여 보정하였다.
5) 통계적 분석: 측정 수치는 평균±표준편차로 나타냈다. 각 부위에 따른 골밀도, 염증의 활성도에 따른 골밀도, 방사선학적 중증도에 따른 골밀도는 t-test를 통해 검증하였다. 그리고, 각 부위별 골밀도 와 각종 지표사이의 상관관계는 Pearson 상관관계분 석으로 조사하였다. p-value는 0.05 이하를 통계학적 으로 유의한 것으로 간주하였다. 통계처리는 SPSS (Version 10.0, Chicago, USA)를 이용하였다.
결 과 1. 임상적 특징
강직성 척추염 환자 50명(남자 46명, 여자 4명)의 연령은 30.0±6.8세(범위19∼44)였고, 신장은 171.4±
6.3 cm, 체중은 63.3±9.4 kg, 신체비만지수는 21.6±
2.9 kg/m2, 질병 이환 기간은 79.7±62.9개월, 스테로
이드 복용량(16명)은 4.5±12.7단위였다.
CRP는 2.44±2.47 mg/dL, ESR은 35.3±31.3 mm/hr, modified Schober's test는 18.2±2.1 cm, finger to ground test는 20.5±14.9 cm, BASDAI 점수는 24.0±
9.1점, BASRI 점수는 2.0±1.6점이었다(표 1). HLA- B27 양성인 환자는 검사자 44명 중에 40명(90.9%)이 었다.
2. 골밀도의 비교
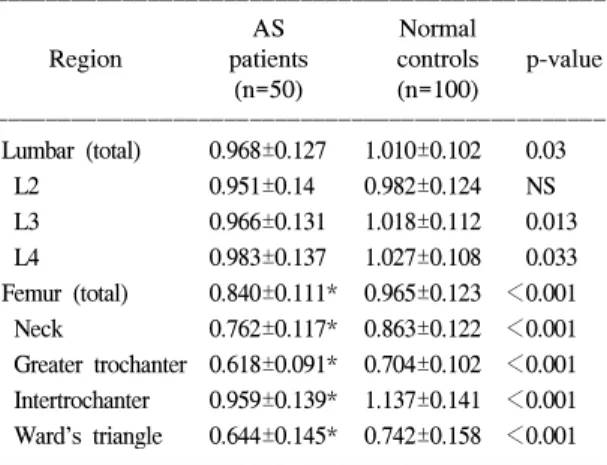
환자군의 요추부와 대퇴부 골밀도의 평균은 대조 군에 비하여 제2요추 부위를 제외한 모든 부위에서 의미있게 감소되어 있었다. 부위별 골밀도를 살펴보 면 환자군과 대조군 모두 요추부에서는 하부요추에 서 높은 경향을 보였으며 대퇴부에서는 큰돌기 부위 Table 1. Clinical characteristics of patients with AS
and normal controls
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
AS Normal
Variable patients control p value (n=50) (n=100)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Age (years) 30.0±6.8 30.0±6.8
Sex (M:F) 46:4 92:8 Height (cm) 171.4±6.3 171.5±6.2 NS Weight (kg) 63.3±9.4 64.6±8.9 NS Body mass
21.6±2.9 21.9±2.3 NS index (kg/m2)
Disease duration
79.7±62.9 (months)
Steroid history
4.5±12.7
(5 mg×months)
CRP (mg/dL) 2.44±2.47 ESR (mm/hr) 35.3±31.3 Modified Schober's
18.2±2.1 test (cm)
Finger to ground
20.5±14.9 test (cm)
BASDAI (score) 24.0±9.1 BASRI (score) 2.0±1.6
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*AS: ankylosing spondylitis, NS: not significant, CRP:
C-reactive protein, ESR: erythrocyte sedimentation rate, BASDAI: Bath ankylosing spondylitis disease activity index, BASRI: Bath ankylosing spondylitis radiological index
가 가장 낮았고, 돌기 사이가 가장 높게 나타났다 (표 2).
3. 골밀도와 상관관계가 있는 인자
염증성 척도의 지표인 CRP, ESR과 질병 활성도 지표인 BASDAI는 요추부 및 대퇴부의 골밀도와 상 관관계를 보이지 않았다.
척추의 가동성을 평가할 수 있는 modified Schober's test와 finger to ground test의 측정값과 골밀도의 관
계를 조사해 보면, modified Schober's test의 측정값 은 요추부의 골밀도와 상관관계가 없었고, 대퇴부의 골밀도와는 유의한 양의 상관관계가 보였다(p=0.026, R=0.322, 그림 1). 또한 대퇴부의 각각의 하위부위 (목, 큰돌기, 돌기 사이, 워드 삼각부)와도 유의한 양 의 상관관계가 있었다(p=0.042, 0.014, 0.026, 0.026, R=0.295, 0.354, 0.321, 0.322). Finger to ground test의 측정값은 요추부의 골밀도와 유의한 음의 상관관계 가 있었고(p=0.004, R=-0.404, 그림 2), 대퇴부와는 상관관계가 없었다.
비록 각각의 염증성 척도가 골밀도치와 상관관계 를 보이지 않았지만 ESR과 CRP의 값에 따라 염증
Fig. 1. Correlation between modified Schober's test and femur BMD (p=0.026, R=0.322, BMD:
bone mineral density).
Table 2. Comparison of regional bone mineral density between ankylosing spondylitis patients and normal controls
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
AS Normal
Region patients controls p-value (n=50) (n=100)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Lumbar (total) 0.968±0.127 1.010±0.102 0.03
L2 0.951±0.14 0.982±0.124 NS L3 0.966±0.131 1.018±0.112 0.013 L4 0.983±0.137 1.027±0.108 0.033 Femur (total) 0.840±0.111* 0.965±0.123 <0.001 Neck 0.762±0.117* 0.863±0.122 <0.001 Greater trochanter 0.618±0.091* 0.704±0.102 <0.001 Intertrochanter 0.959±0.139* 1.137±0.141 <0.001 Ward's triangle 0.644±0.145* 0.742±0.158 <0.001 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*n=48 (2 patients: total hip replacement), AS: ankylos- ing spondylitis
Table 3. Distribution of ankylosing spondylitis patients according to inflammatory factors
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Region Inflammation N BMD p-value ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Low group* 27 0.914±0.123
Lumbar p=0.004
High group** 23 1.014±0.112 Low group 27 0.836±0.122
Femur p=0.835
High group 21† 0.843±0.104
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*Low group: C-reactive protein<1.4 mg/dL or erythro- cyte sedimentation test<15 mm/hr. **High group: C- reactive protein≥1.4 mg/dL, erythrocyte sedimentation test≥15mm/hr. †2 patients: total hip replacement ther- apy, N: number, BMD: bone mineral density.
Fig. 2. Correlation between finger to ground test and lumbar BMD (p=0.004, R=-0.404, BMD:
bone mineral density).
의 활성도가 높은 군과 낮은 군으로 구분하여 골밀 도를 비교하였던 바, 염증의 활성도가 높은 군에서 요추부의 골밀도가 유의하게 낮았다(표 3).
4. 방사선학적 중증도와 골밀도
방사선학적 초기군과 진행군에서 골밀도의 평균치 는 요추부와 대퇴부 모두에서 유의한 차이를 보이지 않았다(표 4).
고 찰
강직성 척추염 환자에서 골다공증이 발생한다는 것은 이미 수많은 연구를 통해 나타나 있고, 요추나 골반부의 부위별로 골밀도에 대한 여러 연구가 있었 다. 1989년 Will 등15)은 강직성 척추염 환자에 있어 서 대퇴골 목부위가 다른 부위에 비하여 골밀도가 의미있게 낮다고 보고하였다. 또한, 1999년 Meirelles 등5)은 요추부나 대퇴부 모두 골밀도가 정상인에 비 해 상대적으로 감소되어 있으나 골감소증과 골다공 증의 빈도는 요추부보다 대퇴부가 더 의미있게 높다 고 보고하였다. 본 연구에서도 마찬가지로 요추부와 대퇴부 모두 골밀도가 낮았으며, 대퇴부가 더 의미 있게 낮았다.
강직성 척추염에서 발생하는 골밀도 감소의 원인 이나 관련인자에 대하여 여러 곳에서 연구가 진행되 고 있지만, 아직까지 뚜렷하게 관련된 인자를 찾지 못하고 있다. 1999년 Armour 등16)은 산화질소의 증 가나 산화질소경로의 활성의 증가가 염증성 질환에 서 골다공증의 병태생리에 영향을 준다고 하였다.
또한, 2001년 Lange 등17)은 1,25(OH)2D3, 부갑상선호 르몬이 강직성척추염의 활성도(ESR, CRP, BASDAI) 와 음의 상관관계가 있고, 알칼리성 인산분해효소와 는 양의 상관관계가 있다고 보고하였다. 즉, 강직성 척추염의 활성도가 높으면 비타민 D의 대사에 영향 을 주고, 골생성을 방해한다는 것이다.
Modified Schober's test는 대퇴부 골밀도와 양의 상관관계, Finger to ground test는 요추부 골밀도와 음의 상관관계를 보여 척추의 가동성과 골밀도사이 에 상관관계가 있음을 보여주었다.
CRP와 ESR이 각각 골밀도와 유의한 상관관계를 보이지 않았으나, CRP와 ESR이 높은 군을 낮은 군 과 비교하였을 때 활성도가 높은 군에서 요추부 골 밀도가 의미있게 낮았다. Dos Santos 등18)은 특히 질 병의 활성도(CRP, ESR)가 높을수록 요추부의 골밀 도가 의미있게 낮다고 보고하였고, Meirelles 등5)도 염증의 활성도가 높은 환자군에서 골밀도가 유의하 게 낮았다고 보고한 바 있다. 본 연구에서도 비슷한 결과를 보여 염증 활성군에서 요추부 골밀도가 의미 있게 낮았다. 따라서 염증의 활성도가 높은 군에서 는 요추부의 골밀도에 대한 주의깊은 관찰이 필요할 것으로 보인다. 그러나 한편으로는 CRP와 ESR가 질 병의 활성도와 연관이 없다는 보고도 있다. 즉, Spoorenberg 등12)은 CRP, ESR보다는 의사의 임상적 소견이 강직성 척추염의 활성도를 더 잘 반영한다는 결과를 보고한 바 있다.
Capaci 등14)은 강직성 척추염이 진행될수록 요추 부보다 대퇴부에서 골밀도가 의미있게 낮다는 결과 를 보고하였다. 본 연구에서 요추부에서는 방사선학 적으로 초기군과 진행군 사이에 골밀도의 의미있는 차이를 보이지 않았다. 그러나 비록 통계학적 유의 수준에는 미치지는 못하였지만(p=0.056) 대퇴부에서 는 진행군의 골밀도가 초기군에 비해 낮게 측정되어 강직성 척추염이 진행될수록 대퇴부의 골밀도가 감 소할 것으로 생각된다.
본 연구는 다음과 같은 제한점이 있다. 첫째, 후향 적 연구이고 대상 환자의 수가 적어 강직성 척추염 환자의 전체를 대표하기에 부족한 점이 있다. 향후 좀 더 많은 환자를 대상으로 전향적인 연구가 필요 할 것이다. 그러나 1대 2로 성별, 연령, 그리고 신체 비만지수까지 일치시킨 대조연구이므로 그 가치가 Table 4. Bone mineral density between early and ad-
vanced according to BASRI
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Bone mineral density ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Early group Advanced group
Region (0∼1) (2∼4) p-value
N=21 N=27
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Lumbar 0.948±0.108 0.974±0.136 0.477 Femur 0.874±0.103 0.813±0.111 0.056 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ BASRI: Bath ankylosing spondylitis radiological index
있다고 하겠다. 둘째, 환자군과 대조군 사이에 골밀 도를 측정하는 기계의 기종이 다르다는 점이다. 그 러나, 같은 회사의 동종모델이었으며, 이를 극복하기 위해 모형을 대상으로 각각 20번 측정하여 얻은 비 교상수가 1.007로 극히 미미하였으므로 골밀도의 결 과와 이에 대한 통계분석에는 영향이 없을 것이라 판단된다. 셋째, 일부 환자에서 스테로이드를 복용한 병력이 있다는 것이다. 그러나 그 숫자가 적었으며 스테로이드 복용량과 골밀도의 상관관계가 없었고, 스테로이드를 복용한 군과 복용하지 않은 군 사이에 도 골밀도의 유의한 차이가 없어 스테로이드 복용병 력이 이 연구의 결과에 커다란 영향을 미치지 않았 을 것으로 판단된다.
결 론
한국인의 강직성 척추염 환자는 건강 대조군에 비 하여 요추부와 대퇴부 모두에서 골밀도가 낮았다.
염증성 활성도가 높은 군에서 요추부 골밀도가 낮았 으며, 척추의 가동성과 골밀도간에도 유의한 상관관 계가 있었다. 강직성 척추염 환자에서 골밀도 감소 에 대한 관심과 적절한 치료가 중요할 것으로 생각 한다.
REFERENCES
1) Ruddy S, Harris ED, Sledge CB, Budd RC, Sergent TS. Kelly's Textbook of Rheumatology. 6th ed. p.
1046. W. B. Saunders. 2001.
2) Fagge CH. Diseases of the osseous system. Case No 1. In: Mitra D, Elvins DM, Collins AJ. Biochemical markers of bone metabolism in mild ankylosing spondylitis and their relationship with bone mineral density and vertebral fractures. J Rheumatol 1999;26:2201-4.
3) Toussirot E, Michel F, Wending D. Bone density, ultrasound measurements and body composition in early ankylosing spondylitis. Rheumatology 2001;
40:882-8.
4) Cooper C, Carbone L, Michet CJ, Atkinson EJ, O'Fallon WM, Melton LJ 3rd. Fracture risk in patients with ankylosing spondylitis: A population based study. J Rheumatol 1994;21:1877.
5) Meirelles ES, Borelli A, Camargo OP. Influence of disease activity and chronicity on ankylosing spon-
dylitis bone mass loss. Clin Rheumatol 1999;18:
364-8.
6) Maillefert JF, Aho LS, Maghraoui El, Dougados M, Roux C. Changes in bone density in patients with ankylosing spondylitis:a two-year follow-up study.
Osteoporos Int 2001;12:605-9.
7) Van der Linden SM, Valkenburg HA, Cats A.
Evaluation of diagnostic criteria for ankylosing spondylitis: A proposal for modification of the New York criteria. Arthritis Rheum 1984;27:361-8.
8) Goie HS, Steven MM, Van der Linden SM, Cats A.
Evaluation of diagnostic criteria for ankylosing spondylitis: a comparison of the Rome, New York and modified New York criteria in patients with a positive clinical history screening test for ankylosing spondylitis. Br J Rheumatol 1985;24:242-9.
9) Auleley GR, Benbouazza K, Spoorenberg A, Collantes E, Hajjaj-Hassouni N, Van Der Heijde D, et al. Evaluation of the smallest detectable difference in outcome or process variables in ankylosing spon- dylitis. Arthritis Rheum 2002;47:582-7.
10) Park HJ, Kim SH, Lee JE, Jun JB, Bae SC. Korean translation and validation of Bath ankylosing spon- dylitis disease activity index (BASDAI): a pilot test.
Qual Life Res 2003;12:817.
11) Calin A, Nakache JP, Gueguen A, Zeidler H, Mielants H, Dougados M. Defining disease acitivity in ankylosing spondylitis is a combination of variables (Bath Ankylosing Spondylitis Disease Activity Index) an appropriate instrument? Rhematology 1999;38:
878-82.
12) Spoorenberg A, van der Heijde D, de Klerk E, Dougados M, de Vlam K, Mielants H, et al. Relative value of erythrocyte sedimentation rate and C-reactive protein in assessment of disease activity in ankylosing spondylitis. J Rheumatol 1999;26:980-4.
13) MacKay K, Mack C, Brophy S, Calin A. The Bath Ankylosing Spondylitis Radiology Index (BASRI): a new, validated approach to disease assessment.
Arthritis Rheum 1998;41:2263-70.
14) Capaci K, Hepguler S, Argin M, Tas I. Bone mineral density in mild and advanced ankylosing spondylitis.
Yonsei Med J 2003;44:379-84.
15) Will R, Palmer R, Bhalla AK, Ring F, Calin A.
Osteoporosis in early ankylosing spondylitis: a primary pathological event? Lancet 1989;23:1483-5.
16) Armour KE, Van'T Hof RJ, Grabowski PS, Reid DM, Ralston SH. Evidence for a pathogenic role of nitric oxide in inflammation-induced osteoporosis. J Bone
Miner Res 1999;14:2137-42.
17) Lange U, Jung O, Teichmann J, Neeck G. Rela- tionship between disease activity and serum levels of vitamin D metabolites and parathyroid hormone in ankylosing spondylitis. Osteoporos Int 2001;12:
1031-5.
18) Dos Santos FP, Constantin A, Laroche M, Destombes
F, Bernard J, Mazieres B, et al. Whole body and regional bone mineral density in ankylosing spondylitis. J Rheumatol 2001;28:547-9.
19) Sivri A, Kilinc S, Gokce-Kutsal Y, Ariyurek M. Bone mineral density in ankylosing spondylitis. Clin Rheumatol 1996;15:51-4.