Tuberc Respir Dis 2009;67:338-344
CopyrightⒸ2009. The Korean Academy of Tuberculosis and Respiratory Diseases. All rights reserved.
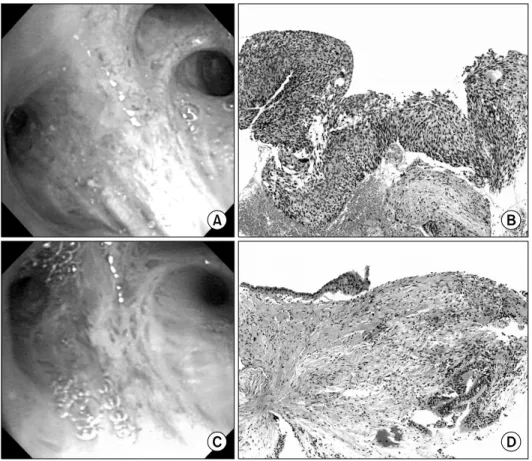
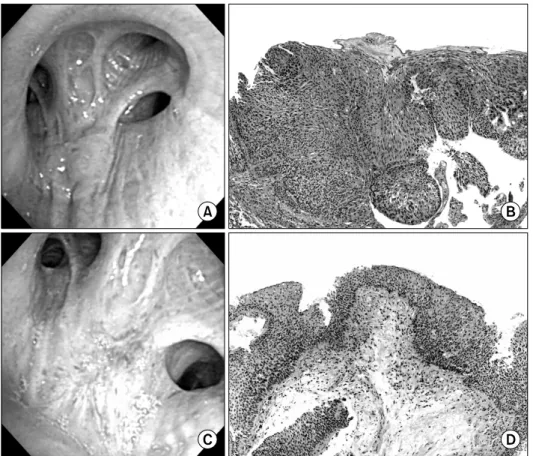
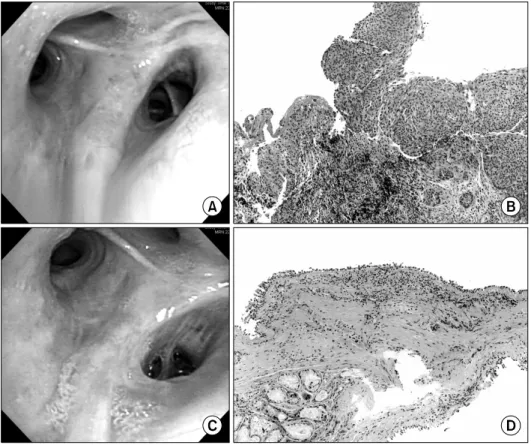
Usefulness of Photodynamic Therapy in the Management of Early Central Lung Cancer: A Report of Three Cases
1
전체 글
1
수치
관련 문서
Key words: Early radiation therapy, Head and neck cancer, Odontogenic infectious lesions, Conservative endodontic drainage.. 통상적으로 보 존수복, 치근관
저자들은 폐암으로 완전 절제 후 다시 반대측 기관지 폐 쇄를 동반한 재발된 폐암 2예에서 광역동 치료를 시행하여 기관지 폐쇄로 인한 심한 호흡 곤란을 치료 하였기에 보고
We had six cases of patients who were treated with long-term testosterone replacement therapy (TRT) after high dose-rate (HDR) brachytherapy and androgen deprivation therapy
