173
•교신저자: 이상돈, 부산대학교 의과대학 비뇨기과학교실
부산시 서구 아미동 1-10번지
Tel: 051-240-7348, Fax: 051-255-7133
E-mail: [email protected]
Acute Epididymitis in Children: 10-Year Retrospective Study of Single Center
Jung Man Kim
1, Chang Yell Lee
1, Sang Don Lee
1,2
From the
1Department of Urology, College of Medicine, Pusan National University, and
2
Medical Reserch Institude, Pusan National University Hospital, Busan, Korea
[Abstract]
Purpose: We studied to describe clinical aspects, to assess the value of diagnostic tests and to determine conspicuous characteristics of acute epididymitis between children and adult.
Materials and Methods: A total of 205 patients with acute epididymitis over a 10-year period were divided into 3 groups: group A (prepuberty; 49 patients), group B (puberty; 42 patients) and group C (adult; 114 patients). We analysed retrospectively the medical records: clinical features, laboratory tests, radiological examinations, accompanying diseases and treatment.
Results: The mean ages were 6.5±2.7, 14.1±2.8, and 43.7±13.4 years in the group A, B, and C (p<0.001), respectively. Prevalence of symptoms including swelling, pain, tenderness and fever were not different among these 3 groups. Serum ESR and CRP levels were significantly higher in group C compare to group A and B (p=0.008 and p<0.001). On urinalysis, pyuria was presented 4 (8.2%), 5 (11.9%), and 19 patients (16.7%) in each group (p=0.341). However, there were only 4 positive urine cultures (1.8%):
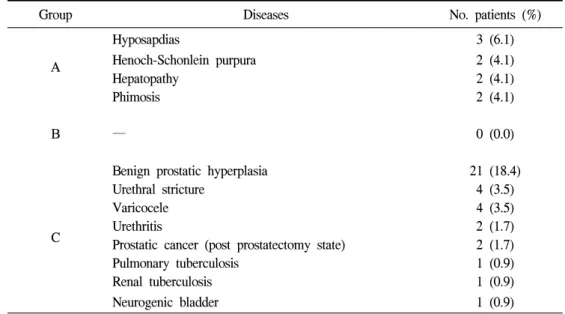
group A; 2 E. coli, group C; 2 Pseudomonas. All of patients performed by Doppler ultrasonography (CDUS) and testicular scan demonstrated the increased vascularity and isotope uptake, respectively. The concomitant diseases causing acquired epididymitis were predominent in the group C. The epididymectomy and scrotal exploration were performed in 0 (0.0%), 1 (2.4%), 1 (0.9%) patients, and in 4 (8.2%), 0 (0.0%), 2 (1.8%) patients in each group, respectively.
Conclusions: Compare to the adults, for the diagnosis of acute epididymitis, CDUS and/or testicular scan were very useful, however serum ESR and CRP level, urinalysis and urine culture seem to be not useful in children. This study suggests that if there is no evidence of infections, empirical antibiotics treatment should not be recommended. (Korean J UTII 2007;2:173-178)
Key Words: Acute epididymitis, Children, Adult
INTRODUCTION
While testicular torsion and appendix testicular
torsion are considered the most common causes of
acute scrotum, acute epididymitis has been recongnized
to have an important role and distressing problem in
acute scrtoum in boys; it accounts for up to 35% of
pediatric patients of acute scrotum.
1 If the adequate
treatment is not provided in the early phase, severe