100
ORIGINAL ARTICLE
급성 음낭증으로 시험적 절개를 시행받은 초등학생 이하 환아들의 임상적 양상
Clinical Outcomes of Scrotal Exploration for Acute Scrotum in Children Less Than 13 Years Old
Hyun Seong Kim, Seoung Wook Lee, Tag Keun Yoo, Jung Yoon Kang From the Department of Urology, Eulji University School of M edicine, Seoul, Korea 김현승ㆍ이승욱ㆍ유탁근
강정윤
을지대학교 의과대학 비뇨기과학교실
Purpose: Acute scrotum is a medical and surgical emergency condition of the scrotum. If testicular torsion, in which early surgical intervention is needed, is not ruled out, scrotal exploration is commonly required. We assessed clinical outcomes of children less than 13 years old who under- went scrotal exploration for acute scrotum.
Patients and Methods: We retrospectively reviewed the medical charts of 57 children less than 13 years old who underwent scrotal exploration for acute scrotum between January 2000 and May 2009. Careful history, duration of scrotal pain, physical examination results, laboratory find- ings, doppler ultrasonographic findings were reviewed. We compared pre- operative presumptive diagnoses with postoperative confirmed diagnoses.
Results: The mean age of the children was 8.5±3.0 years. Forty-three children (75.4%) were admitted through the emergency department, and 14 children (24.6%) visited the outpatient clinic. Of the 53 children, 16 (28.1%) visited our hospital within 6-8 hours of the onset of scrotal pain.
Pyuria was detected in 2 children (3.5%), and leucocytosis in 12 children (21.1%). Blue dot sign was present only in 3 children. Scrotal color dop- pler ultrasonography was performed on 19 children (33.3%). On preopera- tive evaluation, testicular torsion was suspected in 5 children (8.8%), tor- sion of the testicular appendage in 19 children (33.3%), acute epididy- mitis in 12 children (21.1%) and none determined in 21 children (36.8%).
By preoperative color doppler ultrasonography, which was performed on 19 children, testicular torsion was detected in 3 children (15.8%), torsion of the testicular appendage in 4 children (21.1%) and epididymitis in 12 children (63.1%). In 19 children undergoing ultrasonography, the final di- agnosis established after scrotal exploration was testicular torsion (n=3), torsion of the testicular appendage (n=14) or epididymitis (n=2). Overall, the final diagnosis after scrotal exploration was testicular torsion in 12 children (19.0%), torsion of the testicular appendage in 48 children (76.2%) and epididymitis in 3 children (4.8%).
Conclusions: Although doppler ultrasonography has a high accuracy in diagnosis of testicualr torsion, it is not highly accurate for differentiation between torsion of the testicular appendage and epididymitis.
Key Words: Acute scrotum, Torsion, Testicular appendage, Epididymitis 교신저자
강정윤
을지병원 비뇨기과 서울시 노원구 하계1동 281-1, 139-872
Tel: 02-970-8308 Fax: 02-970-8305 E-mail: [email protected]
Fig. 1. Torsion of left testicular appendage in a 4-year-old child whose scrotal sonography findings mimicked epididymitis.
(A) Color Doppler ultrasonography showed increased blood flow in testis and epididymis. (B) Overlying scrotal skin was thickened and epididymis was mildly enlarged.
서 론
급성 음낭증이란 내과적 혹은 외과적 응급치료를 요하는 음낭의 모든 병적 상태를 말한다.1 급성 음낭 증의 원인은 고환염전, 부고환염, 고환염, 고환수염 전, 음낭외상 등이 있고,2 병력과 신체 검사 소견이 도 움이 되나 정확한 감별은 쉽지 않고, 도플러 초음파 등 영상 진단 기구가 발전하였으나 모든 병원에서 언 제나 쉽게 이용하기는 힘들다.3 고환염전은 조기 치료 를 요하는 비뇨기과적 응급 상황이므로 정확한 감별 이 어려울 때 진단을 위한 음낭 시험절개술은 꼭 필요 하다. 고환염전은 주로 사춘기에 나타나고 호발연령 분포가 10-20세에 약 75%를 차지한다고 하나,4 초등 학생 이하 연령에서도 간간히 보고되고 있다. 이에 저 자들은 초등학생 이하 연령에서 급성 음낭증으로 시 험적 절개를 한 환아들의 임상적 양상을 알아보고자 한다.
대상 및 방법
2000년 1월부터 2009년 8월까지 본원 비뇨기과에 급성 음낭증으로 입원한 만 13세 이하 114명의 환아 중 음낭 시험절개술을 시행한 63명을 대상으로 후향 적으로 조사하였다. 내원 당시의 병력, 신체검사, 검 사실 소견, 음낭 색도플러 초음파 소견 등을 기초로 술전 진단과 시험절개술 후 진단을 비교하였다. 진단
은 고환염전, 고환수염전, 급성부고환염 세 가지로 나 누어 각각 좌, 우측 발생 빈도, 나이, 기왕력, 증상 발 현 후 병원까지 도착 시간, 청점 징후 (blue dot sig) 등 을 조사하였다. 가능한 경우에 음낭 색도플러 초음파 검사를 영상의학과에서 시행하였고, ATL IU 22 5-12 MHz (Philips, Andover, USA) 선형 탐촉자를 이용하였 다. 검사는 영상의학과 전문의에 의해 시행되었다. 고 환염전이 의심되어 시험적 절개를 시행할 때 수술은 음낭절개를 통하여 시행하였으며 고환의 색깔, 고환 변색의 회복 여부에 따라 혈액순환이 양호한 경우 고 환고정술을 시행하였고, 경색이 의심된 환자는 고환 적출술을 시행하였다. 고환수염전의 경우에는 고환수 절제술을 시행하였으며, 급성 부고환염으로 판명된 경우에는 보존적 치료를 하였다.
통계학적 검증은 SPSS for windows version 12를 사용 하였으며 Kruskall-Wallis test로 분석하였고 통계학적 인 유의성은 p값이 0.05 미만일 때 의의가 있는 것으 로 간주하였다.
결 과
전체 환아들의 평균 나이는 8.6±2.4세였다. 응급실 을 통해 입원한 경우가 49명 (77.8%), 외래로 직접 내 원한 경우가 14명 (22.2%)이었고, 통증 발생 후 6-8시 간 내에 방문한 경우가 18명 (28.6%)이었다. 소변검사 에서 농뇨가 보인 경우는 2명 (3.5%), 혈액검사에서 백 혈구증다증이 있었던 경우는 14명 (22.2%)이었다. 고
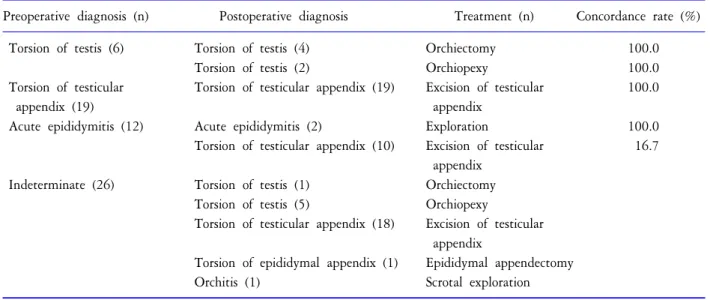
Table 1. Treatment and concordance rate of acute scrotum
Preoperative diagnosis (n) Postoperative diagnosis Treatment (n) Concordance rate (%) Torsion of testis (6) Torsion of testis (4) Orchiectomy 100.0
Torsion of testis (2) Orchiopexy 100.0 Torsion of testicular Torsion of testicular appendix (19) Excision of testicular 100.0
appendix (19) appendix
Acute epididymitis (12) Acute epididymitis (2) Exploration 100.0 Torsion of testicular appendix (10) Excision of testicular 16.7
appendix Indeterminate (26) Torsion of testis (1) Orchiectomy
Torsion of testis (5) Orchiopexy
Torsion of testicular appendix (18) Excision of testicular appendix
Torsion of epididymal appendix (1) Epididymal appendectomy Orchitis (1) Scrotal exploration
Table 2. Clinical characteristics in acute scrotum at postoperative state
Torsion of testis Torsion of testicular Acute epididymitis
p-value (n=12) appendix (n=48) (n=3)
Age (years) 8.7±4.0 8.6±2.7 6.8±3.8 0.480†
Duration of pain (days) 0.9±0.8 1.0±0.8 0.5±0.4 0.206† Visit*≤6-8 hrs (n) 2 (16.7%) 13 (27.1%) 1 (33.3%)
Location (R:L) 4:8 23:25 2:1
Blue dot sign (n) 0 (0.0%) 3 (6.3%) 0 (0.0%) Leukocytosis (n) 4 (33.3%) 8 (16.7%) 2 (66.7%) Previous pain attack (n) 2 (16.7%) 1 (2.1%) 0 (0.0%)
*: number of children who visited hospital within 6-8 hours after onset of scrotal pain, †: Kruskal-Wallis test 환수염전에서 나타나는 청점 징후는 3례에서만 관찰
되었다. 신체검사를 포함하여, 술 전 검사 후의 추적 진단으로는 고환염전이 6명 (9.5%), 고환수염전 19명 (30.2%), 급성 부고환염이 12명 (19.0%), 진단이 애매 한 경우가 26명 (41.3%)이었다. 술 전 색도플러 초음파 검사를 시행한 20명 (31.7%)의 소견은 고환염전 4명 (20.0%), 고환수염전 4명 (20.0%), 급성 부고환염은 12 명 (60.0%)이었다. 이들 20명의 시험적 음낭절개 후 최 종 진단은 고환염전 4명은 모두 염전으로 판명되었 고, 급성 부고환염 12명 중 10명이 고환수염전으로 판 명되었고 나머지는 술 전 색도플러 초음파 검사에서 진단되어진 대로 진단되었다 (Fig. 1). 급성 부고환염 처럼 보였던 고환수염전의 술 전 색도플러 초음파 소 견에서 모두 급성 부고환염의 특징인 부고환의 혈류의 증가 및 부종이 있었다. 농뇨가 보인 2명은 급성 부고
환염이었고 백혈구증다증이 있었던 14명은 고환염전 4명 (28.6%), 고환수염전 8명 (57.1%), 급성 부고환염 2 명 (14.3%)으로 특이성이 없었다. 총 63명의 환아들의 시험절개술 후 최종진단은 고환염전, 고환수염전, 급 성 부고환염이 각각 12명 (19.0%), 48명 (76.2%), 3명 (4.8%)이었다 (Table 1). 고환염전 12명 중 5명 (41.7%) 은 고환혈류가 회복되지 않아 고환적출술을 시행하 였고 7명 (58.3%)은 고환혈류가 회복되어 고환고정술 을 시행하였다. 고환적술술을 시행한 5명의 환아는 평균 나이 8.6세였고 통증이 시작된 후 평균 1.4일에 본원에 도착하였다. 고환수염전 48명 중 부고환수염 전인 경우는 1명 (2.1%)이었다.
음낭 시험적절개술 후 최종 진단된 환아들의 임상 소견을 고환염전, 고환수염전, 급성 부고환염으로 분 류하여 살펴보았다 (Table 2).
고 찰
급성 음낭증은 증상들이 유사하여 원인 질환을 감 별하기 어려운 경우가 있다. 감별이 중요한 이유는 고 환염전을 조기에 판별하여 고환을 보존해야 하기 때 문이다. 이에 급성음낭통과 음낭의 부종이 있는 경우 원인을 알기까지 외과적 응급으로 판단하는 것이 중 요하며 명확하지 않을 시에는 시험적 음낭절개가 필 요하다.3 최근 국내의 많은 병원들에서 색도플러 초음 파 검사가 진단에 이용되고 있다. 색도플러 초음파 검 사는 1980년대 후반부터 급성 음낭증 환자의 진단에 이용하였으며, 고환의 해부학적 영상과 피막 동맥, 구 심성 동맥으로부터 나오는 고환 내 혈류를 알 수 있 다.5 색도플러 초음파로 검사할 때 고환 내 혈류 신호 가 감소되었거나 없을 때 고환염전을 의심하며, 혈류 신호가 증가되어 있고 고환이나 부고환의 종대가 있 을 때 고환염 및 부고환염을 의심할 수 있다.6 색도플 러 초음파 검사는 고환염전에서 민감도 82%, 특이도 100%를 보였고, 부고환염에서 민감도 70%, 특이도 88%를 보이는 것으로 알려져 있다.7 그러나, Steinhardt 등은 고환 염전 2례에서 정상적인 혈류가 나타났으 며, 정상 소아의 고환 혈류는 측정이 안 되는 경우도 있다고 하였다.8,9
고환염전에서 고환의 비가역적 손상으로 인한 고 환 상실을 줄이기 위해 혈류가 차단된 때부터 혈액순 환을 회복하기까지의 시간이 중요하다.10,11 대체로 고 환에서 혈류가 차단된 후 4시간이 지나면 괴사가 시 작되는 것으로 알려져 있다.12 Jefferson 등13이 보고하 기를 고환의 통증이 평균 12시간 지속되었을 때 수술 중 고환혈류가 회복되는 비율이 61%라고 하였다. 본 연구에서 고환염전 12례 중 8시간 내로 온 환아는 2례 (16.7%)였으며 수술 중 소견에서 고환혈류가 회복되 어 고환고정술을 시행하였다. Lewis 등14은 통증 발현 후 8-24시간 내에 내원했을 때 고환의 혈류가 회복되 는 비율이 50%라 하였다. 소아에서는 음낭통증보다 는 복부통증 등 비전형적인 임상소견으로 진단이 늦 어져 고환절제술을 하는 경우도 보고되고 있다.15 본 연구에서는 8-24시간 사이에 병원에 도착한 환아는 1 례 (8.3%)였고, 고환혈류의 회복이 없어서 고환절제술 을 시행하였다.
15세 이하를 대상으로 한 국내 보고에서 32명의 소 아 급성 음낭증 중 급성 부고환염이 66%로 가장 흔하
다고 하였다.16 국외 보고에서는 Flanigan 등17은 소아 의 급성 음낭증 중 가장 흔한 것은 고환수염전이라 보고하였다. 저자들은 국내보고와 다르게 급성 음낭 증 중 급성 부고환염이 3례 (4.8%)밖에 관찰되지 않았 는데 이것은 시험적 음낭절개를 시행하여 고환수와 부고환수의 염전이 있고 이로 인한 고환이나 부고환 의 이차적인 발적이 있는 경우는 고환수염전으로 최 종 진단하였기에 차이가 있을 것으로 생각한다.
고환수는 뮐러관이나 Wolffian관의 흔적기관으로 뮐러관의 근위부가 지속적으로 남아 있을 때 발생하 는 경우가 흔하다.18 주로 고환 상극에 위치하는데 고 환수염전은 고환수의 굵기가 가늘고 길이가 길수록 잘생길 수 있으며, 16세 이전의 소아에서 주로 발생한 다.19 통증은 시간이 지나면서 고환 전체로 퍼져 발적 과 부종을 동반하므로 급성 음낭통을 주소로 하는 다 른 질환과의 감별이 어렵다. 색도플러 초음파 검사의 경우 고환수염전의 진단에 대한 정확성은 확립되지 않았고, 특히 소아에서는 고환 내 동맥직경이 작고 혈 류속도가 느려 감별이 명확하지 않다.20 Karmazyn 등21 이 보고하기를 최종진단이 고환수염전으로 판명된 환아들의 술전 음낭 색도플러초음파에서 급성 부고 환염으로만 진단될 확률이 48%라 하였다. 본 연구에 서 술 전 음낭 색도플러 초음파에서 급성 부고환염으 로 진단된 환아 12명 중 10명이 최종진단에서 고환수 염전으로 판명되었다. 고환수염전에서 음낭부종과 통 증이 5-7일에 걸쳐 서서히 사라진다고 알려져 있어,22 확실한 감별만 이루어지면 보존적 치료도 가능하나 진단이 불확실할 때는 고환의 보존을 위해 시험적 음 낭절개가 추천된다.19
결 론
음낭 색도플러 초음파 검사가 고환염전의 진단에 는 유용하지만, 고환수염전과 급성 부고환염의 감별 에는 정확도가 떨어진다. 그러므로 초등학교 이하 연 령에서 급성 음낭증으로 음낭 색도플러 초음파를 시 행하더라도 의심될 경우 시험적 음낭절개를 시행해 야 하며 또 하나의 유용한 접근법이 될 수 있을 것으 로 생각한다.
REFERENCES
1. Kwon BJ, Kwon SW, Kim DH. Clinical observations on
acute scrotum. Korean J Urol 1988;29:413-9
2. Bae TH, Jung DY, Kim Y, Cho JP. Differential diagnostic method of acute scrotum. J Korean Emerg Med 1997;8:
385-94
3. Cass AS, Cass BP, Veeraraghnvan K. Immedeiate explora- tion of the unilateral acute scrotum in young male subjects.
J Urol 1980;124:829-32
4. Korbel EI. Torsion of the testis. J Urol 1974;111:521-2 5. Middleton WD, Melson GL. Testicular ischemia; Color
Doppler sonographic findings in five patients. AJR 1989;
152:1237-9
6. Dewier DM, Begun FP, Lawson RK, Fitzgerald S, Foley WD. Color Doppler ultrasonography in the evaluation of the Acute scrotum. J Urol 1992;147:89-91
7. Wilbert DM, Schaerfe CW, Stern WD, Stohmaier WL, Bichler KH. Evaluation of the acute scrotum by color- coded Doppler ultrasonography. J Urol 1993;149:1475-7 8. Steinhardt GF, Boyarsky S, Mackey R. Testicular torsion:
Pitfalls of color Doppler sonography. J Urol 1993;150:
461-2
9. Ingram S, Hollman AS. Colour Doppler sonography of the normal paediatric testis. Clin Radiol 1994;49:266-7 10. Lee YB, Kim DS. A clinical observation in torsion of testis.
Korean J Urol 1991;32:932-6
11. Chang HJ, Lee H, Oh YH, Kim DH, Sohn HG, Ha DB, et al. False negative of Doppler ultrasonography during testis torsion in animal model. Korean J Urol 1999;40:
1235-40
12. Bartsch G, Frank S, Marberger H, Mikuz G. Testicular torsion: late results with special regard to fertility and endocrine function. J Urol 1980;124:375-8
13. Jefferson RH, Perez LM, Joseph DB. Critical analysis of
the clinical presentation of the acute scrotum: A 9-year experience at a single institution. J Urol 1997;158:1198- 200
14. Lewis AG, Bukowski TP, Jarvis PD, Wacksman J, Sheldon CA. Evaluation of acute scrotum in the emergency depart- ment. J Pediatr Surg 1995;30:277-81
15. Cho HJ, Kang JY, Yoo TK. Two cases of testicular torsion presented with abdominal pain. Korean J Pediatr Urol 2009;1:64-6
16. Lee JW, Kim YT, Lee HM. Evaluation of the acute scro- tum by color Doppler ultrasonography and radioisotope imaging in children. Korean J Urol 1996;37:671-6 17. Flanigan RC, Dekernion JB, Persky L. Acute scrotal pain
and swelling in children: a surgical emergency. Urology 1981;17:51-3
18. Rolnick D, Kawanoue S, Szanto P, Bush IM. Anatomical incidence of testicular appendates. J Urol 1968;100:758-66 19. Hong SW, Choi HY. The clinical experience of torsion of
testicular appendix with acute scrotal pain. Korean J Urol 1999;40:901-4
20. Burks DD, Markey BJ, Burkhard TK, Balsara ZN, Hal- uszka MM, Canning DA. Suspected testicular torsion and ischemia: evaluation with color Doppler sonography. Radi- ology 1990;175:815-21
21. Karmazyn B, Steinberg R, Livne P, Kornreich L, Grozovski S, Schwarz M et al. Duplex sonographic findings in chil- dren with torsion of the testicular appendages: overlap with epididymitis and epididymoorchitis. J pediztr Surg 2006;
41:500-4
22. Holland JM, Graham JB, Ignatoff JM. Conservative mana- gement of twisted testicular appendages. J Urol 1981;125:
213-4