대 한 류 마 티 스 학 회 지
□
증 례
□ Vol. 12, No. 4, December, 2005― 311 ― 서 론
베체트병은 재발성 구강궤양, 성기궤양 및 포도막 염을 특징으로 하는 만성 염증성 질병으로 젊은 남
성에서 치명적인 혈관염을 일으키는 중요한 원인이 며 환자의 약 25%에서 혈전정맥염, 동맥류 및 동 맥폐색 등을 경험한다1). 그 중 1∼7.7%에서 폐동맥 을 침범한다고 알려져 있으며, 이는 불량한 예후와 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
<접수일:2005년 4월 29일, 심사통과일:2005년 9월 5일>
※통신저자:이 창 근
서울시 송파구 풍납동 388-1번지 서울아산병원 알레르기류마티스 내과
Tel:02) 3010-3284, Fax:02) 3010-6969, E-mail:[email protected]
대량 객혈로 내원한 베체트병 환자에서 시행된 기관지동맥색전술 1예
울산대학교 의과대학 서울아산병원 알레르기류마티스 내과, 진단방사선과*
김용길․고흥규*․고옥배․김택수․김현우․이창근․유 빈․문희범
= Abstract =
Bronchial Artery Embolization for Massive Hemoptysis in a Patient with Behçet’s Disease
Yong Gil Kim, M.D., Heung Kyu Ko, M.D.*, Ock Bae Ko, M.D., Taeg Soo Kim, M.D., Hyun Woo Kim, M.D., Chang-Keun Lee, M.D., Bin Yoo, M.D., Hee-Bom Moon, M.D.
Division of Allergy and Rheumatology, Departments of Internal Medicine, Radiology*, University of Ulsan Collage of Medicine, Asan Medical Center, Seoul, Korea
Behçet’s disease is an important cause of fatal vasculitis in young adult males and vascular involvement has been reported in more than 25% of patients. Pulmonary vascular involvement has been found in 1∼7.7% of patients and is known to be related to poor prognosis. A incidence of fatal hemoptysis is high in patients whose Behçet`s disease is complicated by pulmonary artery aneurysm (PAA). The recurrence of hemoptysis in PAA of Behçet’s disease may result from inadequate medical therapy and complications of surgical treatment. We report a case with Behçet’s disease whose fatal hemoptysis has been successfully treated with bronchial artery embolization.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: Behçet’s disease, Pulmonary artery aneurysm, Embolization
― 대한류마티스학회지 제 12 권 제 4 호 2005 ―
― 312 ― 연관이 있다2). 또한 폐동맥은 두번째로 흔한 동맥침 범 부위이며 침범한 병변의 65%에서는 동맥류를 보 이며 35%에서는 동맥폐색의 형태로 나타난다3,4). 폐 동맥류는 여러 결합조직병 중 베체트병에서 특징적 으로 나타나며 동맥중간막의 탄성섬유의 손상과 혈 관강의 확장 등으로 인한 염증반응이 일어나 전층의 괴사를 동반한 가성동맥류를 형성한다고 알려져 있 으며 대부분 양폐야를 침범하는 다발성 병변으로 나 타나지만 드물게 단일 병변을 보이기도 한다5-7). 1994년 Hamuryudan 등이 보고한 바에 따르면 베 체트병으로 인한 객혈을 경험한 환자의 50%에서 평 균 9.5개월의 생존율을 보였다2). 이는 베체트병의 총 체적 사망률이 3∼4%인 점을 고려할 때 객혈은 사 망에 이르게 하는 중요한 원인으로 여겨지고 있다8). 객혈의 치료에는 객혈의 양과 신체 증후에 따라 cor- ticosteroid, cyclophosphamide 등의 내과적 약물치료와 엽절제술, 구역절제술 등의 수술적 방법, 기관지동맥 색전술 등의 방법이 있다9). 약물치료는 동맥류의 퇴 행을 일으킬 수 있으나 수주에서 수개월 이내에 재 발이 흔하며 응급수술은 40% 정도의 높은 술 후 사 망률을 보인다고 알려져 있다10,11). 이에 비해 기관지 동맥색전술은 비교적 안전한 방법으로 즉각적인 지 혈효과도 90% 이상으로 보고되고 있으며 수술을 시 행한 경우에 비해 좋은 예후를 보였다12,13). 결핵, 기
관지확장증, 폐암 등으로 인한 다량객혈의 경우 우 선적으로 기관지동맥색전술이 추천되고 있으나 베체 트병에 동반된 폐동맥류 출혈로 인한 다량 객혈 시 기관지동맥색전술이 시행된 예가 국내에는 아직 보 고가 없어 기관지동맥색전술 후 객혈이 조절된 1예 를 보고하는 바이다.
증 례
36세 남자가 5년 전부터 한 달에 1회 이상 재발하 는 구강궤양과 좌측 하지의 5 cm 크기의 열감과 통 증을 동반한 홍반성 피부병변이 발생하였으며 당시 좌안의 갑작스런 시력감퇴가 있어 지역병원 방문 후 베체트병을 진단받고 6개월 정도 부신피질호르몬을 복용하였다.
내원 3년 전 갑자기 발생한 말더듬증으로 인근 대 학병원에서 컴퓨터 단층촬영 및 자기공명영상 촬영 을 통해 열공중풍(lacunar stroke) 진단 후 물리치료 및 보존적 치료로 회복되었다. 이후 간혹 주사 맞은 부위에 염증이 생기는 증상 외에는 별다른 문제없었 다.
내원 2주 전 갑자기 300 cc 이상의 객혈이 발생하 여 인근 병원 방문 후 컴퓨터 단층촬영상 우하엽의 출혈 소견 보여 우측 기관지동맥의 색전술을 시행하
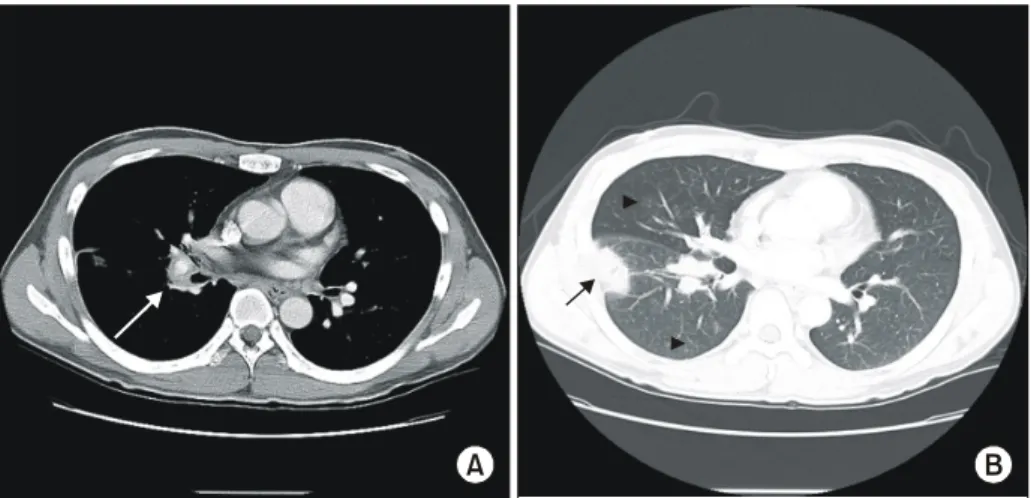
Fig. 1. Chest computed tomography with mediastinal window setting (A) and lung window setting (B). (A) Pseudoaneurysm with surrounding vascular wall thickening is noted at the right lower lobar pulmonary artery (arrow). (B) Subpleural infarction secondary to pseudoaneurysm and vasculitis is noted (arrow). Multiple focal ground glass opacity represents aspirated blood due to hemoptysis (arrowhead).
A B
― 김용길 외 : 베체트병에서의 기관지동맥색전술 ―
― 313 ― 였으나 2일 후 다시 객혈을 보여 본원으로 전원되었 다. 본원 내원 당시 혈압은 118/80 mmHg, 맥박 112 회/분, 호흡수 20회/분, 체온은 36.5oC로 관찰되었으 며 의식은 명료하였으나 지속적인 객혈을 보여 중환 자실로 입원하였다. 검사실 소견상 백혈구 7,900/mm3, 혈색소 10.4 g/dL, 혈소판 355,000/mm3, 적혈구침강속 도 105 mm/hr를 보였고 프로트롬빈시간 73.6%, 활성 화 부분 트롬보플라스틴 시간 41.5초, 항트롬빈 III 87%, 섬유소원 845 mg/dL, D-이중체(D-dimer) 1.60으 로 나타났다. 본원에서 시행한 컴퓨터 단층촬영상 우하엽에 흉막과 인접하여 쐐기모양의 경화소견과 광범위한 젖빛유리모양의 병변이 관찰되었으며 우하 엽 폐동맥의 동맥류를 동반한 혈전과 갑작스런 차단 이 관찰되어 베체트병의 폐동맥 침범에 합당한 소견 이었으며(그림 1A, B) 응급으로 시행한 기관지동맥 조영술에서도 우하엽 폐동맥류의 출혈 소견이 관찰 되어 젤폼(gelfoam)을 사용하여 색전술을 시행하였다 (그림 2A∼C). 내원 당시 보였던 좌측하지의 부종에 대해 심부정맥혈전 동반되었을 가능성 높아 하지정 맥도플러 검사를 시행하였으며 좌측 대퇴정맥에서 오금정맥에 걸쳐 약 15 cm의 혈전이 관찰되었다. 매 일 고용량의 prednisolone (1 mg/kg)과 cyclophospha- mide 100 mg을 같이 복용하였으며 기관지동맥색전술 후 5개월 관찰 시 더 이상의 객혈은 보이지 않았다.
고 찰
베체트병은 전신을 침범하는 만성 염증성 질환으 로 병인은 명확하지 않다. 조직학적으로 모든 크기 의 혈관을 침범하여 혈관염을 일으킨다고 알려져 있 으며 드물지만 폐동맥의 경색이나 출혈, 동맥류 등 을 형성하기도 한다14). 베체트병의 동맥침범은 드물 지만 병의 경과에 매우 나쁜 영향을 끼친다고 알려 져 있다. Turkey에서 시행된 534명의 베체트병 환자 중 후향적 검색을 통해 밝혀낸 8명의 폐동맥류 환자 에 대한 치료결과를 보면 수술이 시행된 3명은 모두 수술 후 사망하였으며 corticosteroid나 cyclophopha- mide 등의 약물치료만 시행된 5명 중 3명도 지속적 인 객혈로 사망하여 결국 폐동맥류가 발생된 경우 수술이나 면역억제제만의 치료로 병의 경과를 호전 시킬 수 없다고 주장하였다15). 베체트병의 폐동맥류 는 많은 경우 다발성으로 발생하며 혈관염으로 인한 유약한 혈관벽으로 인하여 수술이 어려울 수 있다.
또한 재발한 경우 지속적으로 복용 중인 cortico- steroid, 면역억제제로 인한 수술 후 치유과정의 지연 및 감염의 위험은 반복적인 수술이 이루어지기 어렵 게 한다. 대안으로 기관지동맥색전술이 최근에 보고 되고 있으며 성공적인 지혈작용으로 객혈로 인한 사 망을 막을 수 있었다9). 본 증례에서는 Tunaci 등의 보고와 같이 가장 흔히 침범하는 우하기관지동맥에 서 병변이 관찰되었으며 반복적인 색전술을 시행하 Fig. 2. Selective arteriography of the right intercosto- bronchial trunk (A), right 6th intercostals artery (B) and right
bronchial artery (C) showed parenchymal staining and distal pulmonary artery filled with contrast suggesting bronchial-pulmonary shunt. After selective embolization of above arteries, massive hemoptysis was successfully
― 대한류마티스학회지 제 12 권 제 4 호 2005 ―
― 314 ― 여 성공적으로 객혈을 조절하였다6). 이후 고용량의 corticosteroid와 cyclophosphamide를 사용하여 베체트 병의 활성도를 안정화 시켰다. 우측 하지정맥의 혈 전에 대한 치료는 출혈의 가능성이 높아 적극적인 항응고제나 항혈소판제제를 사용하지 않고 침상안정 과 탄력양말 등의 고식적인 치료를 시행하였다. 흔 히 객혈을 유발시키는 원인으로 알려진 결핵, 기관 지확장증, 아스페루질루스종 등의 기질적인 폐질환 의 경우 기관지동맥색전술의 장기 지혈효과에 대해 비교적 많이 알려져 있으나 베체트병과 같은 자가면 역질환의 경우는 아직 효과가 검증되어 있지 않은 실정이다12).
본 증례는 베체트병으로 인한 폐동맥류 출혈 시 면역억제제 사용과 더불어 신속한 기관지동맥색전술 을 시행하여 초기 대량 객혈을 성공적으로 치료함으 로써 객혈로 인한 사망을 예방하여 향후 지속적인 치료를 가능하게 하였다는 데 의미가 있다. 이와 같 은 증례는 드물게 보고되기 때문에 색전술의 유용성 에 대한 전향적인 연구가 어려운 제한점을 가지고 있으므로 먼저 후향적 연구를 통하여 치료의 효과를 검증하는 것이 필요할 것으로 생각한다.
REFERENCES
1) Shimizu T, Ehrlich GE, Inaba G, Hayashi K. Behcet disease (Behcet syndrome). Semin Arthritis Rheum 1979;8:223-60.
2) Hamuryudan V, Yurdakul S, Moral F, Numan F, Tu- zun H, Tuzuner N, et al. Pulmonary artery aneurysm in Behcet’s Syndrome: a report of 24 cases. Br J Rheumatol 1994;33:48-51.
3) Koc Y, Gullu I, Akpek G, Akpolat T, Kansu E, Kiraz S, et al. Vascular involvement in Behcet’s disease. J Rheumatol 1992;19:402-10.
4) Erkan F, Kiyan E, Tunaci A. Pulmonary complica-
tions of Behcet’s disease. Clin Chest Med 2002;23:
493-503.
5) Hiller N, Lieberman S, Chajek-Shaul T, Bar-Ziv J, Shaham D. Thoracic manifestations of Behcet disease at CT. Radiographics 2004;24:801-8.
6) Tunaci M, Ozkorkmaz B, Tunaci A, Gul A, Engin G, Acunas B. CT findings of pulmonary artery aneurysms during treatment for Behcet’s disease. AJR Am J Roentgenol 1999;172:729-33.
7) Grenier P, Bletry O, Cornud F, Godeau P, Nahum H.
Pulmonary involvement in Behcet disease. AJR Am J Roentgenol 1981;137:565-9.
8) Lacombe P, Qanadli SD, Jondeau G, Barre O, Mosu- rolle B, Mouas H, et al. Treatment of hemoptysis in Behcet syndrome with pulmonary and bronchial Em- bolization. J Vasc Interv Radiol 1997;8:1043-7.
9) Cantasdemir M, Kantarci F, Mihmanli I, Akman C, Numan F, Islak C, et al. Emergency endovascular management of pulmonary artery aneurysms in Beh- cet’s disease: report of two cases and a review of the literature. Cardiovasc Intervent Radiol 2002; 25:533-7.
10) Efthimiou J, Johnston C, Spiro SG, Turner-Warwick M. Pulmonary disease in Behcet’s syndrome. Q J Med 1986;58:259-80.
11) Gourin A, Garzon AA. Operative treatment of massive hemoptysis. Ann Thorac Surg 1974;18:52-60.
12) Mal H, Rullon I, Mellot F, Brugiere O, Sleiman C, Menu Y, et al. Immediate and long-term results of bronchial artery embolization for life-threatening hemoptysis. Chest 1999;115:996-1007.
13) Uzun O, Akpolat T, Erkan L. Pulmonary vasculitis in Behcet’s disease. A cumulative analysis. Chest 2005;
127:2243-53.
14) Kasikcioglu E, Akhan H, Cuhadaroglu C, Erkan F.
Pulmonary artery aneurysm in Behcet’s disease: a case report. Heart Vessels 2004;19:157-9.
15) Saba D, Saricaoglu H, Bayram AS, Erdogan C, Dilek K, Gebitekin C, et al. Arterial lesions in Behcet’s disease. Vasa 2003;32:75-81.