변형된 S a u v e - K a p a n d j i 술식을 이용한 부정유합된 C o l l e s골절의 치료
신현대・이광진・이준규・양준영・정제택
충남대학교 의과대학 정형외과학교실
= Abstract =
The Modified Sauve-Kapandji Procedure for Treatment of Malunited Colles` Fracture
Hyun-Dae Shin, M.D., Kwang-Jin Rhee, M.D., June-Kyu Lee, M.D., June-Young Yang, M.D. and Je-Taek Jeong, M.D.
Department of Orthopaedic Surgery, School of Medicine Chungnam National University, Taejon, Korea
Distal radius fracture is one of the most common fracture of upper extremities including Colles’fracture. Since 1913, classic Darrach’s technique which performed excision of the distal end of the ulna for distal radioulnar arthrosis have been introduced, many procedures have been described for the surgical management of painful disorders of the distal radioulnar joint. In 1936, Sauve and Kapandji first described the procedure that included an arthrodesis across the distal radioulnar joint and created a pseudarthrosis of the ulna, proximal to the fusion, to restore pronation and supination. The purpose of the present study is to evaluate clinical results of treatment for malunited Colles’fracture using modified Sauve-Kapandji procedure as an alternative salvage operation. From 1994 May, total nine patients were evaluated, average follow-up was twenty one months. There were four male patients and five female patients.
※통신저자 : 신현대
대전광역시중구대사동640 (301-040) 충남대학교병원정형외과학교실
Tel : (042) 220 - 7343, 7349 Fax : (042) 253 - 3010
*이논문은 1 9 9 8년추계골절학회에서구연되었슴.
서 론
C o l l e s골절을포함하는원위부요골의골절은상지 에발생하는가장흔한골절로 , 과거에는치료방법에 관계없이비교적좋은 예후를가지는손상으로받아 들여졌다. 그러나현재에는치료방법과골절의형태 에따라서다양한결과와예후를보이는매우복잡한 골절로인식되고있다.
한편, 부정유합된원위부요골의골절은크게관절 외 골절과 관절내 골절로 분류되고, 관절외 골절의 부정유합의 문제점은 골간단부의 각형성과 요골의 단축이며, 관절내 골절은 요수근 관절 또는 요척 관 절 및 양 관절의 문제를 초래하고 관절외 골절의 문 제점과관절내골절의문제점이복합되는경우도적 지않다.
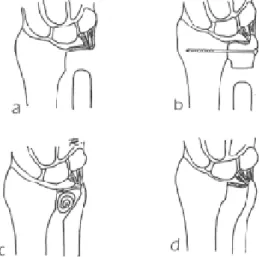
1 9 1 3년 D a r r a c h가 원위부 척골을 절제하는 시술을 시행한이후여러종류의변형된술식이발전해왔는 데(Fig. 1), 부정유합된 원위부 요골의 수술적 치료는 완관절 기능의 소실, 동통의 정도, 방사선학적 소견, 임상증상 등을 참고로 결정되어지고 있다6 , 7 , 8 , 1 1 ). 이 에 저자들은 Sauve-Kapandji 술식을 이용한 부정유합 된 Colles 골절의임상치험례및수술결과를문헌고 찰과함께보고하는바이다.
연구대상 및 방법
1. 연구대상
1 9 9 4년 5월이후부터충남대학교병원정형외과에 Radiographic measurement, pain of radiocarpal and radioulnar joint, range of motion of the wrist, grip strength, instability of the distal radioulnar joint were foci of this present study. We used modified Sauve-Kapandji procedure. The purpose of modification is to preserve the pseudoarthrosis and stabilize the ulna, proximal ulnar stump was stabilized with a strip of flexor carpi ulnaris and pronator quadratus was sutured to sheath of extensor carpi ulnaris. According to Fernandez Point-Score System, results showed excellent 6, good 2 and fair 1. But two patients complained continuous pain at vigorous range of motion. All of the patient showed improvment of arc of motion and rotation, especially pronation-supination and did not develop any instability. But radiographic measurement was not correlated with clinical symptoms. In conclusion, modified Sauve-Kapandji procedure is effective procedure for treatment of the malunited Colles’fracture which have severe distal radioulnar disruption, ligament laxity, subluxation of the ulna, and ulnocarpal impingement. We should consider as alternative salvage operation options of malunited Colles’fracture.
Key Words: Distal radioulnar joint, Malunited Colles’fracture, Modified Sauve-Kapandji procedure
Fig 1.Schematic of the various operative procedures for the distorted distal radioulnar joint ; (A) Darrach, (B) Sauve-Kapandji arthrodesis, (C) Bowers’hemiresection interposition
arthroplasty, (D) Watson matched ulnar resection.
Table 1. Preoperative clinical data.
1 55/F -24 16 14 +1/+3 severe 5/80 90/80 10/90 15/90 9/20
2 49/M +34 30 1 +1/+2 severe 45/75 45/75 65/80 40/80 29/42
3 20/M 0 5 9 0/+1 mild 70/75 80/75 85/70 90/80 27/35
4 62/M -18 13 2 +1/+3 mod 40/80 60/85 45/85 30/90 21/42
5 63/F -30 10 9 +1/+3 severe 45/80 90/80 60/80 40/85 7/22
6 54/F -8 18 6 0/+2 mild 30/75 15/70 45/85 45/90 10/30
7 67/F -12 9 6 0/+3 mod 25/75 30/75 30/80 35/85 10/19
8 48/F -15 15 5 +1/+3 mild 50/65 50/80 40/80 50/75 12/25
9 53/M -5 12 0 0/+2 mild 80/70 30/70 50/90 40/80 21/47
*: Volar tilt, ulnar tilt ; degree. Ulnar variance ; milimeter.
†: Radiocarpal/radioulnar pain. 0 ; none, +1 ; mild, +2 ; moderate, + 3 ; severe
‡: Radiographic degenerative change. Severe ; narrowing of the joint space, subchondral scleosis, formation of osteophytes,
subluxation, and incongruity of the joint. Moderate ; narrowing of the joint space, subchondral scleosis, and incongruity of the joint. Mild ; minimum narrowing of the joint space. None ; none of the this radiographic findings.
§: Affected/normal
Grip strength
(kgf)§
Age/ Deg.
Case Pain†
Sex change‡
Radiographic measurement* Volar Ulnar Ulnar
tilt tilt variance
ROM of wrist(deg)§ Flex Ext Pron Supin
Table 1. Postoperative clinical data.
1 12 2 9 2 0/+1 mild 45/80 80/80 75/90 70/90 15/25
2 19 13 34 -1 0/0 mild 50/75 70/75 90/80 85/80 37/42
3 34 5 0 0 0/0 none 80/75 80/75 90/70 90/80 35/40
4 25 6 21 0 0/0 none 75/80 70/85 70/85 75/90 30/39
5 17 -3 18 2 +1/0 mod 70/80 70/80 75/80 80/85 15/20
6 23 7 19 0 0/0 none 60/75 75/70 80/85 85/90 23/32
7 22 0 15 1 0/0 mild 55/75 7075 70/80 65/85 12/18
8 14 4 22 1 0/0 none 65/65 80/80 75/80 80/75 25/27
9 27 3 25 0 0/0 none 80/70 80/70 80/90 80/90 30/45
*: Volar tilt, ulnar tilt ; degree. Ulnar variance ; milimeter.
†: Radiocarpal/radioulnar pain. 0 ; none, +1 ; mild, +2 ; moderate, + 3 ; severe
‡: Radiographic degenerative change. Severe ; narrowing of the joint space, subchondral scleosis, formation of osteophytes,
subluxation, and incongruity of the joint. Moderate ; narrowing of the joint space, subchondral scleosis, and incongruity of the joint. Mild ; minimum narrowing of the joint space. None ; none of the this radiographic findings.
§: Affected/normal
Grip strength
(kgf)§
F/U Deg.
Case Pain†
(m) change‡
Radiographic measurement* Volar Ulnar Ulnar
tilt tilt variance
ROM of wrist(deg)§ Flex Ext Pron Supin
서원위부요골의부정유합으로교정수술을 받았던 환자중, 최소 1 2개월이상추시가가능하였고요수근 관절(radiocarpal joint)에 광범위한 관절 파괴를 갖고 있지않으면서원위요척골관절 (distal radioulnar joint) 의 광범위한 손상이나 아탈구( s u b l u x a t i o n )를 가지고 있는 환자로연구대상을 제한하였다. 선택된 총 9 례 의환자중남녀비율은 4 : 5 이었으며, 평균나이는 5 2 세( 2 0~67 세)였고, 평균추시 기간은 21 개월( 1 2~3 4 개월)이었다(Table 1, 2).
2. 연구방법
방사선학적 측정(radiographic measurement), 원위부 요척골의 동통(pain of radioulnar joint), 완관절의 운동 범위(ROM of wrist), 수부완력(grip strength), 완관절의 불안정성(instability) 등을 중점적으로 측정 비교하였 다(Table 1, 2). 방사선학적으로volar tilt, ulnar tilt, ulnar variance 등을 측정하였데 수술전 평균값이 각각 - 8 . 7 도, 14.2도, 5.8 mm 의 소견을 보였다. 원위부 요척골 관절의 동통(pain of radioulnar joint)은 심한 작업시에 동통은있으나정신적신체적장애를보이지않을때 를 경증 ( m i l d )으로 , 장애를 보일 때를 중등도 ( m o d e r a t e )로, 휴식 또는 일상 생활 동안에도 동통이 있을때를중증( s e v e r e )으로정의하였다. 또한 요수근 ( r a d i o - c a r p a l )과 요척골관절(radio-ulnar joint)의 동통으 로세분하여측정하였는데수술전주로요척골관절 부위의 동통을 호소하였고 특히 5례의 환자에서는 중증( s e v e r e )의 동통을 호소하였다. 완관절의 운동범 위는신전굴곡(arc of motion ; flexion-extension)과회전 (rotation ; pronation-supination)으로 측정하였는데수술 전 평균이 각각 9 7 . 8도, 90.6도를 보였다. 수부완력 (grip strength)은 Jamar hand dynamometer (Asimow Engineering, Los Angeles, California)를 이용하여 측정 하였는데 정상측의 50% 정도의 완력을 수술전에 보 였다. 완관절의 불안정성( i n s t a b i l i t y )은 전완부를회내 전시켜 척골두가 현저한 돌출을 보일 때를 중등도 (moderate), 아탈구소견을보일때를중증( s e v e r e )의불 안정성이있는것으로판단하였다.
3. 수술방법(surgical technique)
전례에서 Sauve-Kapandji 술식을 통한 교정 수술을 시행하였는데, 시술방법은원위부척요골관절면으
로부터 척수근 신근( E C U )의 건을 따라 근위부 약 5 cm 상방까지 절개선을 넣고 척골 신경 분지를 확인 한 다음, 척골두의1 . 5~2 c m에서가능한한척골의 원 위 부 에 가 깝 게 절제하였다 . 척 골 의 가관절 ( p s e u d o a r t h r o s i s )를유지하고 안정시키기 위해척수근 굴근( F C U )을 사용하여 근위부 척골(proximal ulnar s t u m p )을 안정시켜주고 방형 회내근 ( p r o n a t o r q u a d r a t u s )을척수근신건( E C U )에봉합하는변형된술 식을사용하였다(Fig. 2). 또한경우에따라요골의절 골술(open wedge radial osteotomy) 및척골의단축을시 행하였으며, T-자형 금속판과 K강선을 이용하여 고 정하였다.
4. 수술후처치(postoperative care)
술후 2주간의 석고 고정후 바로 수동적 운동을 시 작하였고, K강선은술후 8주, 금속판은3개월후에특 히수배부절개(dorsal approach)를한경우는장무지신 전근( E P L )이 tethering 되는 것을 방지하기 위해 제거 하는것을원칙으로하였다.
Fig 2.Schematic representation of modified Sauve- Kapandji procedure. The ulnar head is secured with two screws or k-wires. The proximal ulnar stump is stabilized with a strip of the flexor carpi ulnaris(FCU). The pronator quadratus(PQ) is sutured to the sheath of the extensor carpi ulnaris(ECU).
결 과
총 9명의환자를최소 1 2개월이상 최종추시한결 과, Fernandez point-score system에 의거하여 우수 (excellent) 6례(67%), 양호(good) 2례(22%), 유용(fair) 1 례( 1 1 % )였으며, 불량( p o o r )한결과는없었고전체 9례 중양호이상이 8례( 8 9 % )로나타났다. 하지만이중 2 례에서심한작업시경미한원위요척골관절부위의 동통을 호소하였다. 수술후 volar tilt, ulnar tilt 및 u l n a r v a r i a n c e는각각 4 . 1도, 18.1도, 0.55mm로술전의 - 8 . 7도, 1 4 . 2도, 5.8mm보다 1 2 . 8도, 3.9도, 5.2mm의방사선학적 인 호전을 보였다. 완관절의 굴곡신전 및 회전 운동 범위도각각 1 3 9 . 4도, 157.2도로 술전의 9 7 . 8도, 90.6도 보다 4 1 . 6도, 66.6도의 호전된 양상을 보였다. 수부완 력(grip strength score)은 술전의 정상측의 5 0 %에서 7 6 %로회복소견을보여 2 6 %의호전을보였다. 완관 절의불안정성( i n s t a b i l i t y )는 모든례에서발생하지않 았다.
증례 보고
증례1. 유ㅇ순
5 5세 여자 환자로 좌측 완관절의 심한 동통 및 운 동범위 제한, 특히 회전 장애( p r o n a t i o n - s u i n a t i o n l i m i t a t i o n )를주소로내원하였으며약 20 년전낙상사 고로보존적 요법으로 치료한경력과함께 1 년전부 터 완관절 이하의 저림(tingling sensation)이 동반되었 고 이학적 검사상 2 5도의 회전 제한 및 심한 수부완 력의 약화 소견을 보였던 증례였다. 방사선 소견상 volar tilt -24도, ulnar tilt 16도, ulnar positive variance 14 mm 로 측정되었으며 , 심한 척수근 관절의 충돌 (ulnocarpal impingement)과좁아진관절면과골극의형 성등퇴행성 변화가심한소견을 보였다(Fig. 3). 수술 은요골절골술(open wedge radial osteotomy)과척골원 위부를 절제한 후, T자 금속판과 K강선을 이용하여 해부학적인 위치로 내고정한후 자가 골이식술을 시 행하였다. 최종추시에서동통은심한운동시에만호 소하였고 완관절 회전은 1 4 5도로 상당한 회복을 보
Fig 3.Radiographic findings of a 55-year-old woman with posttraumatic distal radioulnar joint arthrosis.
A.Preoperative views showing 14mm of ulnar positive variance, ulnocarpal impingement and posttraumatic osteoarthritis of DRUJ.
B.Postoperative views demonstrate correction of the ulnar positive variance and pinning of the DRUJ.
C.Radiographic appearence of the wrist at follow-up.
The patient had symptomatic relief.
A
C
B
였던예였다.
증례2. 이ㅇ행
4 9세 남자로 완관절 동통을 주소로 내원하였으며 현병력상 1년전 낙상 사고로 보존적 치료를 시행했 던경력이 있었고이학적소견상중등도의운동범위 제한 및 수부완력의 감소를 보였다. 방사선 사진상 심한 관절면의 불일치(incongruity) 및 원위부 요척골 의부정유합소견이동반되었고, volar tilt +34도, ulnar tilt 30도, ulnar positive variance 1mm 로측정되었다( F i g . 4). 수술은 K강선을 이용하여 시행하였고, 술후동통 은호소하지않았던증례였다.
고 찰
1 9 1 3년 D a r r a c h가 원위부 척골을 절제하는 시술을 시행한 이후, Sauve-Kapandji 술식, Watson의 m a t c h e d distal ulnar resection, Bowers의 h e m i r e s e c t i o n - i n t e r p o s i t i o n arthroplasty 등등 여러 종류의 변형된 술식이 발전해
왔는데(Fig. 1), 일반적으로완관절기능의소실, 동통 의 정도, 방사선학적 소견, 임상증상 등을 참고로 부 정유합된 원위부 요골의 수술적 치료방법이 결정되 어 지고 있다. Fernandez6 , 7 , 8 )는 원위부 요척골 부정유 합의 기본적인 후유증으로는 척수근 관절의 충돌 (ulno-carpal impingement), 척골두의 아탈구( d o r s a l subluxation or instability of ulnar head)과 요척골 관절의 불일치(incongruity of the surface of the radioulnar joint)등 이라고 주장하였으며, 여러저자들에의해 Darrah 술 식의 가장 큰 문제점은 수부완력의 약화 및 척골의 불안정성과 동통이라고 보고되어 왔다3 , 6 , 1 3 , 1 6 ). 따라 서 B o w e r s3 )와 Watson 등2 2 , 2 3 )은 척수근 관절과 T F C C 를 보존하는 원위부 요골의 부분 절제술 ( p a r t i a l r e s e c t i o n )을고안하였고 S a u v e와 Kapandji 2 0 )는척골두 를 절제하지 않는 술식을 고안하였다. 본 연구에서 시행한 Sauve-Kapandji 술식은 척골두가 절제되지 않 기때문에원위부요척골관절의일치 ( c o n g r u i t y )를유 지할 수 있고 미용상 좋으며 관절면이 건전( i n t a c t )하 고힘의전달 과정이보다 생리적이고TFCC, 척수근 관절건(ulnocarpal ligament), 척수근신전근( E C U )등을 Fig 4.Radiographic findings of a 49-year-old man with
malunited intraarticular DRUJ fracture.
A.Preoperative views showing articular incongruity with 34 degree volar tilt.
B.Postoperative views showing ulnar resection and DRUJ fusion with K-wire.
C.Radiographic appearence at the most recent follow- up, one year and seven months postoperatively.
A
C
B
보전할수있는장점이있는것으로알려져있다1 4 , 1 5 ). 단점으로는 근위부 척골의 불안정성, 동통, 이소성 화골염 및 불유합등 있으나3 , 2 1 ), 본 임상 치험례에서 는 2례에서만 경한 동통을 보였을 뿐 다른 합병증은 없었다. Lichtman 등1 4 )은 Darrach 술식은 활동성이 비 교적 적은 노인에서 유용한 술식이지만 건의 이완 (ligament incompetence)이 동반된 류마티스관절염 환 자에서는주의를 요하며, Sauve-Kapandji 술식은척수 근 충돌(ulnocarpal abutment)이나 건 이완( l i g a m e n t l a x i t y )을보이는류마티스관절염환자에서효과적인 술식이지만골질이약한 (poor bone stock)경우에는세 심한주위가필요하다고하였고, 이와유사한보고들 이발표되어왔다4 , 5 , 1 0 , 2 0 ). Field 등9 )은 Darrah 술식을시 행한 3 6례중, 단지 5 0 %에서만족할만한결과를얻었 고수부완력약화및동통은지속되었다고발표하였 다. Bell 등1 )은 1 1례의 경험에서 불량한 결과를 얻었 다고 했으며, Bieber 등2 )은특히 젊은환자와 건이완 을보인환자에서 불량한결과를보였다고보고하였 다. 하지만 변형된 Sauve-Kapandji 술식을 이용한 본 연구에서는 전체 9례 중 양호 이상이 8례로 좋은 결 과를보여주었다.
한편, Fernandez8 )는 원위부 요척골 관절의 불일치 ( i n c o n g r u i t y )가단순 방사선사진소견상 잘증명되지 않을 경우에는 컴퓨터 촬영을 통하여 요골두 및
sigmoid notch에서의 불일치을 확인하는 것이중요하
다고 하였으나, 본 연구에서는 잘 보이지 않는 경우 에 사위( o b l i q u e )사진을 얻어 관찰함으로서, 컴퓨터 촬영을시행한경우는 1례도없었다. 또한 F e r n a n d e z8 ) 는 충돌( i m p i n g e m e n t )가 존재하는 경우 요골두와 수 근골이 접촉하는 부위에 연골연화증( c h o n d r o m a l a c i a ) 과 T F C C의괴양(ulcer) 소견이항상 관찰된다고하였 으나, 본연구에서는수술소견상일부에서만연골연 화증소견이확인되었다. 이는아마도심한 volar tilt로 인한 아탈구가있는경우가있었기때문으로사료되 었다.
B o w e r s3 )는 positive ulnar variance가 2 m m이상소견을 보이는 경우 hemiresection arthroplasty와 함께 척골의 단축을 추가적으로 시행해야 한다고 하였고 , Lichtman 등1 4 )은 가능하다면 1mm negative ulnar variance 상태로 고정하는 것을 추천하였으며, 또한 Bowers 술식에서는 척수근 관절의 충돌( u l n o - c a r p a l
a b u t m e n t )이 존재하는 경우 교정이 불가능하며 추가 적인척골의단축수술이필요하다고하였고, Watson 술식의경우에도원위부요척골관절외의다른 동반 된병변이있는경우에는동통완화에있어서만족할 만한 술식은 아니라고 주장하였다. 본 연구에서는 ulnar variance가 존재하는 경우 변형된 S a u v e - K a p a n d j i 술식을 시행함으로서 불필요한 추가적인 수술을 피 할수있었으며대체로수술후만족할만한방사선소 견을얻을수있었다(Table 1,2).
J u p i t e r와 R i n g1 2 )은 관절면의 부정유합( a r t i c u l a r m a l r e d u c t i o n )과 각형성(dorsal angulation)이 2 0도 이상 인경우 조기교정수술이필요하지만 방사선학적소 견보다는동통과완관절의기능제한등의임상적증 상에기초하여수술적응증을결정해야한다고주장 하였는데, 본연구에서도방사선학적소견과동통의 정도가 일치하지 않았으며(Table 1), 주로 임상적인 증상에비중을두어수술적응증을선택하였다.
Darrach 술식과 마찬가지로 불안정성과 이에따른 동통이 Sauve-Kapandji 술식에서도 발생한다고 여러 저자들이 보고하였다1 1 , 1 5 , 1 7 , 1 8 , 1 9 , 2 0 ). Mikkelsen 등1 5 )은 Sauve-Kapandji 술식을시행한 1 2례의환자중 2례에서 절제된근위부척골부위에심한운동시동통을호소 하였다고 했으며, Sanders 등1 9 )은 1 0례중 6례에서 불 안정성을 보였고 그중 2례에서 완관절 회전시에 동 통을호소하였다고보고하였다. Kapandji2 0 )는가관절 ( p s e u d o a r t h r o s i s )은 가능하면 원위부에 시행하고 절제 부위도 가능한한 적게 해야 한다고 주장하였으며, Nakamura 등1 7 )은 가능하면 원위부에 가관절을 만들 어야 수부완력(grip strength)을 증가시킬수 있으며 그 렇게함으로서 요골두로부터축력(axial force)을효과 적으로절제된근위부 척골로전달할수있다고하였 다. 본연구에서도가능한한원위부에서적은부위의 척골절제를시행하였고척수근굴근( F C U )과척수근 신근( E C U )을 이용한 변형된 술식을 사용함으로서 불안정성은전례에서보이지않았으며, 오직 2 례에 서만 경한 동통을 보이는 만족할 만한 결과를 얻을 수있었다.
Mikkelsen 등1 5 )은 1 2례의 임상 경험에서 수부완력 이 5 3 %에서 7 6 %로의 호전을 보고하였고, Taleisnik2 1 ) 는 1 7례의 외상환자군에서 1 1례는정상, 5례는 정상 의 70%, 나머지 1례에서는 정상의 5 0 %의 회복을 보
고하였는데, 본 연구의 경우 5 0 %에서 7 6 %로 2 6 %의 호전을보여비슷한결과를얻을수있었다 .
결 론
1 9 9 4년 5월 이후부터 충남대학교병원 정형외과에 서, Colles 골절후 원위부 요골의 부정유합으로 수술 적치료를받았고 1년이상추시가가능하였던 9명의 환자을분석한결과, 방사선학적소견과임상증상은 서로상관관계가없었으며. 완관절의굴곡신전보다 회전에서더좋은결과를보였다. 결론적으로변형된 Sauve-Kapandji 술식은건이완소견및 원위부요척골 관절의 광범위한 손상과 특히 척수근 관절의 충돌 (ulnocarpal impingement)소견을보이고, 퇴행성관절염 이합병된경우나관절의아탈구등의불안정한경우 에 있어서 더욱 효과적인 술식이 될 수 있을 것으로 생각되며, 또다른 구제수술치료(salvage operation)의 한방법으로고려할수있을것으로사료된다 .
R E F E R E N C E
1. Bell MJ, Hill RJ and McMurtry RY : Ulnar impingement syndrome. J Bone Joint Surg, 67-B : 126-129, 1985.
2. Bieber EJ, Linscheid RL and Dobyns JH : Failed distal ulna resections. J hand Surg, 13-A : 193-200, 1 9 8 8 .
3. Bowers WH : Distal radioulnar joint arthroplasty : The hemiresection interposition technique. J hand S u r g, 10-A : 169-178, 1985.
4. Dell PC : Distal radioulnar joint dysfunction. H a n d C l i n, 3 : 563-583, 1987.
5. Drewniany JJ and Palmer AK : Injuries to the distal radioulnar joint. Orthop Clin N Am, 3 : 451- 459, 1986.
6. Fernandez DL : Correction of posttraumatic wrist deformity in adults by osteotomy, bone-grafting, and internal fixation. J Bone Joint Surg, 64-A : 1164- 1178, 1982.
7. Fernandez DL : Radial osteotomy and Bowers arthroplasty for malunited fractures of the distal end of the radius. J Bone Joint Surg, 64-A : 1164-1178, 1 9 8 2 .
8. Fernandez DL : Radial osteotomy and Bowers arthroplasty for malunited fractures of the distal end of the radius. J Bone Joint Surg, 70-A : 1538-1551, 1 9 8 8 .
9. Field J, Majkowski RJ and Leslie IJ : Poor results of Darrach’s procedure after wrist injuries. J Bone Joint Surg, 75-B : 53-57, 1993.
10. Gonqalves D : Correction of disorders of the distal radioulnar joint by artificial pseudarthrosis of the ulna. J Bone Joint Surg, 56-B : 462-464, 1974.
11. Jupiter JB and Fernandez DL : Fractures of the distal radius : A practical approach to management.
1st ed, New York, Springer-Verlag : 263-315, 1996.
12. Jupiter JB and Ring D : A comparision of early and late reconstruction of malunited fractures of the distal end of the radius. J Bone Joint Surg, 78-A : 739-748, 1996.
13. King GJ, McMurtry RY, Rubenstein JD and Gertzbein SD : Kinematics ofthe distal radioulnar joint. J hand Surg, 11-A : 798-804, 1986.
14. Lichtman DM, Ganocy TK and Kim DC : The indications for and techniques and outcomes of ablative procedures of the distal ulna. Hand Clin, 14 : 265-277, 1998.
1 5 . Mikkelsen SS, Lindblad BE and Larsen ER : Sauve-Kapandji operation for disorders of the distal radioulnar joint after Colles’fracture. Acta Orthop S c a n d, 68 : 64-66, 1997.
16. Milch H : Cuff resection of the ulnar for malunited C o l l e s’fracture. J Bone Joint Surg, 32 :311-313, 1 9 4 1 .
17. Nakamura R, Tsunoda K and Watanabe E : The Sauve-Kapandji procedure for chronic dislocation of the distal radioulnar joint with destruction of the articular surface. J hand Surg, Br : 127-132, 1992.
18. Rothwell AG, O’neill L and Cragg K : Sauve- Kapandji procedure for disorders of the distal
radioulnar joint : A simplified technique. J hand S u r g, 21-A : 771-777, 1996.
19. Sanders RA, Frederick HA and Hontas RB : The Sauve-Kapandji procedure : A salvage operation for the distal radioulnar joint. J hand Surg, 16-A : 1125- 1129, 1991.
20. Sauve K and Kapandji IA : Nouvelle technique de traitment chirurgical des luxations recidivantes isolees de l’extremite inferieure du cubitus. J Chir ( P a r i s ) 47 : 589-594, 1936.
21. Taleisnik J : The Sauve-Kapandji procedure. C l i n O r t h o p, 275 : 110-123, 1992.
22. Watson HK and Gabuzda GM : Matched distal ulnar resection for posttraumatic disorders of the distal radioulnar joint. J hand Surg, 17-A : 724-730, 1 9 9 2 .
23. Watson HK, Ryu JY and Burgess RC : Matched distal ulnar resection. J hand Surg, 11-A : 812-817, 1 9 8 6 .