대한외과학회지:제 76 권 제 2 호
□ 원 저 □
Vol. 76, No. 2, February, 2009
90
책임저자: 윤익진, 서울시 화양동 4-12번지
143-729, 건국대학교병원 외과 Tel: 02-2030-7583, Fax: 02-2030-7748 E-mail: [email protected]
접수일:2008년 6월 26일, 게재승인일:2008년 9월 29일
복강경적 충수절제술 후 성인과 소아에서의 합병증 비교 연구
건국대학교 의학대학원 건국대학교병원 외과학교실, 1성균관대학교 의과대학 삼성서울병원 외과학교실
배수연ㆍ윤익진ㆍ이경영ㆍ성무경ㆍ유영범ㆍ장성환ㆍ김지수
1A Comparative Study about Complications of Laparoscopic Appendectomy in Children and Adults
Soo Youn Bae, M.D., Ik Jin Yun, M.D., Kyung Yung Lee, M.D., Moo Kyung Seong, M.D., Young Bum Yoo, M.D., Seong Hwan Chang, M.D., Jee Soo Kim, M.D.1
Department of Surgery, Konkuk University Hospital, Konkuk University School of Medicine, 1Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Purpose: In recent studies, laparoscopic appendectomy has been widely performed for not only uncomplicated
appendicitis but also perforated appendicitis. But, in children, the value of laparoscopic appendectomy for acute appendicitis is not yet established. Our retrospective study is to evaluate the safety of laparoscopic surgery for acute appendicitis in children.
Methods: We reviewed electronic medical records of a total of 595 patients (95 children and 500 adults), who
had been operated upon for acute appendicitis, from August 2005 to February 2007. Those patients were divided into two groups; children and adults. Demographic data, duration of pain, diagnostic methods, length of stay, operative time, time under anesthetic, time to diet, perforation rate, and complication rates were analyzed.
Results: In eight adult patients, laparoscopic surgery was converted to open laparatomy. There was no significant
difference in perforation rates (children 20.0% vs. adults 18.1%, P=0.714). However, postoperative complication rates were significantly higher in the children group (7.4%) compared to the adult group (2.2%).
Conclusion: We noted that laparoscopic appendectomy should be applied cautiously, especially in pediatric groups
due to the relatively high complication rate. However, we need to see more high-quality randomized trials. (J
Korean Surg Soc 2009;76:90-93)Key Words: Appendicitis, Laparoscopy, Perforation, Complications
중심 단어: 충수염, 복강경, 천공, 합병증
서 론
복강경적 충수절제술(laparoscopic appendectomy, LA)은 1983년 Semm(1)에 의해 처음으로 시행되었으며, 이후 성인
뿐만 아니라 소아에서도 대중적으로 시행되고 있다. 복강 경 수술 후 작은 절개 범위, 수술 후 통증 감소, 회복 속도 및 일상 생활로의 조기 복귀 등의 효용성과 복강경적 충수 절제술 후 합병증의 발생률(13.2∼18.5%)이 개복적 충수절 제술 후 발생률(12.8∼17.5%)과 유의한 차이가 없음이 지속 적으로 발표되면서 그 안전성이 입증되고 있으며,(2-9) 최 근에는 단순 충수염뿐만 아니라 천공성 충수염에서도 기능 성과 효능이 증명되고 있다.(10-13)
소아에서도 복강경적 수술법은 개복술과 비교하여 성인 의 경우와 장단점에 있어서 차이점이 없이 안전하게 시행
Soo Youn Bae, et al:A Comparative Study about Complications of Laparoscopic Appendectomy in Children and Adults
91
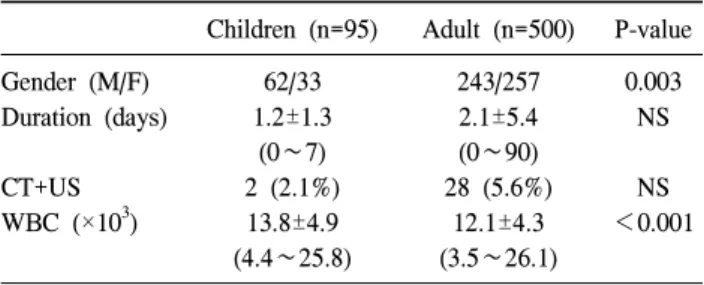
Table 1. Groups characteristics
Children (n=95) Adult (n=500) P-value
Gender (M/F) 62/33 243/257 0.003
Duration (days) 1.2±1.3 2.1±5.4 NS
(0∼7) (0∼90)
CT+US 2 (2.1%) 28 (5.6%) NS
WBC (×103) 13.8±4.9 12.1±4.3 <0.001
(4.4∼25.8) (3.5∼26.1) NS = Not significant.
될 수 있다고 생각되고 있다.(3,14) 그러나, 수술 시간, 병원 비용을 고려할 때 과연 복강경 수술의 장점만 강조할 수 있는지는 단정지을 수 없다.(15) 더구나 소아에게 있어서는 특별한 장점이 없으며,(2) 오히려 복강경적 충수절제술 후 복강 내 농양의 발생률이 높아진다는 보고도 있다.(2,3,16,17) 이에 본 저자들은 급성 충수염으로 복강경적 충수절제술 을 시행 받은 환자들을 대상으로 임상양상, 서로 다른 연령 군 특히, 소아에서 복강경적 수술법이 안전하게 시행할 수 있는가 평가하기 위하여 본 연구를 계획하였다.
방 법
2005년 8월부터 2007년 2월까지 급성충수염으로 복강경 적 충수절제술을 시행 받은 595명의 환자들을 대상으로 전 자 의료 차트 시스템을 이용하여 후향적으로 분석하였다.
환자들은 연령에 따라 15세 이하 소아군과 16세 이상 성 인군으로 나누어 성별, 증상 발현 기간, 백혈구 수, 알부민, C반응단백(C-reactive protein, CRP), 술 전 영상검사(US, CT), 천공성 충수염의 비율, 수술 시간, 수술 소견, 개복술로 의 전환, 임상 과정(입원기간, 가스배출시기, 식이시작시기, 수술 후 합병증)에 대하여 비교하였다.
여기서의 천공성 충수염은 수술 전 영상자료에 농양 및 연조직염(phlegmon)을 동반하는 등 천공의 소견이 보이는 경우, 수술 시 육안적으로 천공이 있었던 경우, 조직 검사에 서 충수돌기의 천공이 확인된 경우로 정의하였다.
복강경 충수절제술은 3-공법으로 배꼽 부위와 배곧은근 옆 두 부위는 5 mm 트로카를, 치골 상방 부위는 10 mm 트 로카를 삽관하였으며, 복강 내 압력은 15 mmHg로 유지하 였다. 충수간막(mesoappendix)은 Sonosurgy (또는 Ligasure) 와 복강경 전기 소작기를 이용하여 충수돌기와 분리하였고 충수돌기 기저부는 HEM-O-LOK 폴리머 클립(Weck, North Carolina, USA) 또는 ENDO LOOP (Johnson & Johnson, Seoul, Korea)를 이용하여 봉합 후 절단하였다.
충수돌기는 복강경 주머니(LAPBAG, Sejong, Paju, Korea) 를 이용하여 제거하였고 치골 상방의 근막 결손 부위는 polysorb 2-0을 이용하여 복구해주었으며 천공이 있거나 수 술 전 복강에 전체적으로 퍼져있어 범 복막염 상태로 술 후 농양 형성이 가능성이 높다고 판단되는 경우에 Jackson- Pratt 배액관을 삽입하였다.
SPSS for Window를 이용하여 카이 제곱 검정과 스튜던트 T검정으로 두 그룹 간의 결과들을 비교하였으며 다중선형
회귀분석을 이용하여 합병증과의 관련인자를 분석하였다.
P<0.05인 경우에 통계적 유의성이 있다고 판단하였다.
결 과
총 595명의 환자들 중 15세 이하의 소아는 95명(남아 62 명, 여아 33명), 성인 500명(남자 243명, 여자 257명)으로 소 아군에서 남아의 비율이 높았다(P=0.003)(Table 1).
증상 발현 후 병원 내원하기까지 기간은 소아군에서 평 균 1.2±1.3일(범위: 0∼7일), 성인군은 평균 2.1±5.4일(범위:
0∼90일)로 통계학적으로 차이는 없었고(P=0.108), 입원 당 시 백혈구 수는 소아군 13.8±4.9 (×103/μl), 성인군 12.1±4.3 (×103/μl)으로 소아에서 높았다(P<0.001).
진단을 위한 영상학적 검사는 CT와 초음파 중 주로 한 가지를 시행하였으며 진단의 정확도를 높이기 위해 CT와 초음파 두 가지를 시행한 경우 소아에서는 2명(2.1%), 성인 에서는 28명(5.6%)으로 두 군에서 유의한 차이는 없었다 (P=0.059).
가스 배출 시기, 식이 진행 시기는 소아군이 성인군보다 빠르게 진행되었지만 총 입원 기간은 소아군은 평균 5.0±
2.6일(범위: 3∼20), 성인군은 평균 5.0±2.0일(범위: 3∼21)로 통계학적 차이가 없었다(P=0.837)(Table 2).
천공성 충수염의 비율은 소아군은 20.0% (19명), 성인군 에서 18.1% (92명)로 유의한 차이는 없었고(P=0.71), 수술시 간도 소아군에서 57.9±27.9분(20∼200분), 성인군에서 60.5±
29.3분(15∼330분)으로 통계적으로 차이가 없었다(P= 0.428) (Table 2).
595명 환자 모두 일차적으로 복강경 충수절제술을 시행한 경우로 염증 정도가 심하여 회장 및 맹장의 부분 절제술이 필요하거나 충수돌기를 확인할 수 없었던 성인 8명의 환자 는 개복술로의 전환이 필요하였으나 소아군에서는 없었다
92
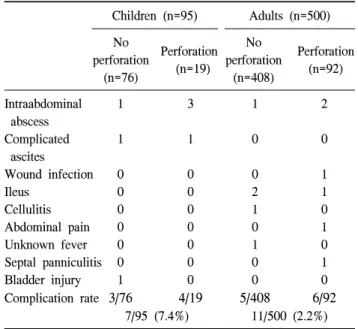
J Korean Surg Soc. Vol. 76, No. 2Table 3. Analysis of all complications
Children (n=95) Adults (n=500) No Perforation
perforation
(n=19) (n=76)
No Perforation perforation
(n=92) (n=408)
Intraabdominal 1 3 1 2
abscess
Complicated 1 1 0 0
ascites
Wound infection 0 0 0 1
Ileus 0 0 2 1
Cellulitis 0 0 1 0
Abdominal pain 0 0 0 1
Unknown fever 0 0 1 0
Septal panniculitis 0 0 0 1
Bladder injury 1 0 0 0
Complication rate 3/76 4/19 5/408 6/92
7/95 (7.4%) 11/500 (2.2%) Table 2. Results of subgroup analysis
Children (n=95) Adults (n=500) P-value
Gender (M/F) 62/33 243/257 0.003
Length of stay 5.0±2.6 5.0±2.0 NS
(days) (3∼20) (3∼21)
Operative time 57.9±27.9 60.5±29.3 NS
(min) (20∼200) (5∼330)
Gas out (#POD) 1.0±0.5 (0∼3) 1.1±0.5 (0∼4) 0.037 Time to liquid 1.2±0.6 (0∼4) 1.4±0.9 (0∼10) 0.017 (#POD)
Perforated (%) 19 (20.0%) 92 (18.1%) NS
Conversion (%) 0 8 (1.6%) NS
Complication (%) 7 (7.4%) 11 (2.2%) 0.007 NS = Not significant.
(P=0.051)(Table 2).
수술 후 합병증이 발생한 경우는 소아군에서 7명(7.4%), 성인군에서는 11명(2.2%)으로 소아군에서 유의하게 높았다 (P=0.007)(Table 2). 비천공성인 경우에 소아 3.9% (3/76), 성 인 1.2% (5/408, P=0.048)로, 천공성 충수염의 경우 소아 21.0% (4/19), 성인 6.5% (6/92, P=0.002)로 소아군에서 합병 증 발생이 높았다(Table 3).
소아에서 유의하게 합병증 발생이 높은 것을 고려하여 합병증 발생의 관련인자에 관하여 다중선형회귀분석 결과 성인군에서는 수술 시 복강 내 고름(pus)동반 여부(P=0.006) 와 천공성 여부(P=0.011)가 유의하게 나왔으나 소아군에서 는 백혈구 수(WBC)만이 유의하게(P=0.011) 나왔고 천공성 여부(P=0.058)나 고름 동반 여부(P=0.065)는 유의한 상관관 계가 없었다.
두 그룹에서 모두 사망한 경우는 없었으며 소아군에서 복강 내 농양 4명, 복수 2명, 방광손상 1명으로 총 7명(7.4%) 이 발생하였고 성인군에서는 복강 내 농양 3명, 상처감염 1명, 장마비 3명, 봉소염 1명, 원인을 알 수 없는 복통 1명, 발열 1명, 중격 지방층염(Septal panniculitis) 1명으로 총 11 명(2.2%)에서 합병증이 발생하였다(Table 3).
고 찰
복강경적 충수절제술 후 발생하는 복강 내 농양의 발생 률은 천공성 충수염의 경우에는 개복적 충수절제술 후 발 생률보다 높으며,(2,16-20) 단순 충수염(비천공성 충수염)의 경우에서도 복강경적 충수절제술 후 복강 내 농양이 발생 할 수 있음이 보고된 바 있다.(14,21)
본 저자들은 소아에서 유의하게 합병증 발생률이 높을 것을 고려, 소아군에서는 성인과 다르게 수술 후 합병증 발 생에 수술 당시의 충수염의 정도(severity) 외에 다른 요인이 관련 있을 수 있음을 고려하였다. 이 연구가 후향적이라는 제한점과 소아 수술 시에 좁은 복강 안에서 복강경 기구 조작이 어려운 점, 성인과 비교하여 질병의 진행 속도가 빠 르고 동반된 장염의 소견에 의한 소장의 팽만 및 염증이 수술에 어려움을 줄 수 있는 것 등의 가능성을 생각할 수 있다.
하지만, Serour 등(11)이 소아에서 복강경적 충수절제술 에서 개복적 충수절제술 후 드물게 발생하는 합병증을 분 석하여 이것은 병리 소견보다는 수술 방법과 관련이 있음 을 밝혔다. 복강경적 충수절제술 후 복강 내 농양의 높은 발생률은 복강 안에서 충수돌기가 절단되면서 복막이 오염 되거나,(8) 충수 돌기 안의 감염된 내용물이 기복강 상태에 서 복강 안으로 흘러나오면서 퍼지는 것으로 설명할 수도 있을 것이다.(17) 몇몇 동물 실험들에서 이런 생각이 가능 함을 보여주기도 하였으며,(11,22) Neuhaus와 Watson(23)은 CO2 기복강에 반응하여 복막표면에서 초 미세구조 및 대사 적, 면역적인 변화를 관찰하였다. 또한 충수돌기 절제 시에 사용되는 전류적 기구들에 의해 인접 조직에 열전도에 의 해 손상이 일어날 수도 있음을 고려해야 한다.(24-27) 우리 자료에서도 복강경적 충수절제술 후 상처 감염이 나, 장마비, 복강 내 농양 등 수술 후 합병증 발생률은 기존 의 개복적 충수절제술이나 복강경적 충수절제술 후 그것과
Soo Youn Bae, et al:A Comparative Study about Complications of Laparoscopic Appendectomy in Children and Adults
93
비교하였을 때 소아군과 성인군에서 모두 낮게 나와 복강 경적 충수절제술의 안정성을 인정할 수 있었다. 그러나 소 아에서는 염증 정도 외에 다른 이차적 요인에 의해 성인과 달리 예상치 못한 합병증이 생길 수 있으므로 수술 방법 선택 시 신중을 기해야 하며 이 문제는 전향적인 연구 등으 로 지속적인 연구가 필요하다고 생각한다.
REFERENCES
1) Semm K. Endoscopic appendectomy. Endoscopy 1983;15:
59-64.
2) Glasgow RE, Fingerhut A, Hunter J. SAGES appropriateness conference: a summary. Surg Endosc 2003;17:1729-34.
3) Sauerland S, Lefering R, Neugebauer EAM. Laparoscopic ver- sus open surgery for suspected appendicitis. Cochrane Database of Systematic Reviews 2004, Issue 4. Art. No.:
CD001546. DOI: 10.1002/14651858.CD001546.pub2.
4) Gilchrist BF, Lobe TE, Schropp KP, Kay GA, Hixson SD, Wrenn EL Jr, et al. Is there a role for laparoscopic appendec- tomy in pediatric surgery? J Pediatr Surg 1992;27:209-12.
5) Canty TG Sr, Collins D, Losasso B, Lynch F, Brown C.
Laparoscopic appendectomy for simple and perforated appen- dicitis in children: the procedure of choice? J Pediatr Surg 2000;35:1582-5.
6) Hart R, Rajgopal C, Plewes A, Sweeney J, Davies W, Gray D, et al. Laparoscopic versus open appendectomy: a prospec- tive randomized trial of 81 patients. Can J Surg 1996;39:
457-62.
7) Hellberg A, Rudberg C, Kullman E, Enochsson L, Fenyo G, Graffner H, et al. Prospective randomized multicentre study of laparoscopic versus open appendicectomy. Br J Surg 1999;86:
48-53.
8) Ortega AE, Hunter JG, Peters JH, Swanstrom LL, Schirmer B. A prospective, randomized comparison of laparoscopic ap- pendectomy with open appendectomy. Laparoscopic Appen- dectomy Study Group. Am J Surg 1995;169:208-12.
9) Katkhouda N, Mason RJ, Towfigh S. Laparoscopic versus open appendectomy: a prospective, randomized, double-blind study. Adv Surg 2006;40:1-19.
10) Yau KK, Siu WT, Tang CN, Yang GP, Li MK. Laparoscopic versus open appendectomy for complicated appendicitis. J Am Coll Surg 2007;205:60-5.
11) Serour F, Witzling M, Gorenstein A. Is laparoscopic appen- dectomy in children associated with an uncommon post- operative complication? Surg Endosc 2005;19:919-22.
12) Ikeda H, Ishimaru Y, Takayasu H, Okamura K, Kisaki Y, Fujino J. Laparoscopic versus open appendectomy in children with uncomplicated and complicated appendicitis. J Pediatr Surg 2004;39:1680-5.
13) Nadler EP, Reblock KK, Qureshi FG, Hackam DJ, Gaines BA, Kane TD. Laparoscopic appendectomy in children with perfo- rated appendicitis. J Laparoendosc Adv Surg Tech A 2006;16:
159-63.
14) Oka T, Kurkchubasche AG, Bussey JG, Wesselhoeft CW Jr, Tracy TF Jr, Luks FI. Open and laparoscopic appendectomy are equally safe and acceptable in children. Surg Endosc 2004;
18:242-5.
15) Ignacio RC, Burke R, Spencer D, Bissell C, Dorsainvil C, Lucha PA. Laparoscopic versus open appendectomy: what is the real difference? Results of a prospective randomized dou- ble-blinded trial. Surg Endosc 2004;18:334-7.
16) Horwitz JR, Custer MD, May BH, Mehall JR, Lally KP.
Should laparoscopic appendectomy be avoided for complicated appendicitis in children? J Pediatr Surg 1997;32:1601-3.
17) Krisher SL, Browne A, Dibbins A, Tkacz N, Curci M.
Intra-abdominal abscess after laparoscopic appendectomy for perforated appendicitis. Arch Surg 2001;136:438-41.
18) Long KH, Bannon MP, Zietlow SP, Helgeson ER, Harmsen WS, Smith CD, et al. A prospective randomized comparison of laparoscopic appendectomy with open appendectomy: clini- cal and economic analyses. Surgery 2001;129:390-400.
19) Pedersen AG, Petersen OB, Wara P, Ronning H, Qvist N, Laurberg S. Randomized clinical trial of laparoscopic versus open appendicectomy. Br J Surg 2001;88:200-5.
20) Tang E, Ortega AE, Anthone GJ, Beart RW Jr. Intraabdominal abscesses following laparoscopic and open appendectomies.
Surg Endosc 1996;10:327-8.
21) Bonanni F, Reed J 3rd, Hartzell G, Trostle D, Boorse R, Gittleman M, et al. Laparoscopic versus conventional appen- dectomy. J Am Coll Surg 1994;179:273-8.
22) Bloechle C, Kluth D, Holstein AF, Emmermann A, Strate T, Zornig C, et al. A pneumoperitoneum perpetuates severe dam- age to the ultrastructural integrity of parietal peritoneum in gastric perforation-induced peritonitis in rats. Surg Endosc 1999;13:683-8.
23) Neuhaus SJ, Watson DI. Pneumoperitoneum and peritoneal surface changes: a review. Surg Endosc 2004;18:1316-22.
24) Campbell PA, Cresswell AB, Frank TG, Cuschieri A. Real- time thermography during energized vessel sealing and dissec- tion. Surg Endosc 2003;17:1640-5.
25) Kennedy JS, Stranahan PL, Taylor KD, Chandler JG. High- burst-strength, feedback-controlled bipolar vessel sealing. Surg Endosc 1998;12:876-8.
26) Hoenig DM, Chrostek CA, Amaral JF. Laparosonic coagulat- ing shears: alternative method of hemostatic control of un- supported tissue. J Endourol 1996;10:431-3.
27) Kinoshita T, Kanehira E, Omura K, Kawakami K, Watanabe Y. Experimental study on heat production by a 23.5-kHz ultra- sonically activated device for endoscopic surgery. Surg Endosc 1999;13:621-5.