29
• 교신저자:김태형, 중앙대학교병원 비뇨기과 서울 동작구 흑석동 224-1 우 156-755
Tel: 02-6299-1785, Fax: 02-6294-1406, E-mail: [email protected] Received: February 8, 2012
Revised: February 24 and March 20, 2012 Accepted: March 26, 2012
소변배양검사에서 광범위 베타락탐 분해효소 생산균에 의한 급성단순방광염 환자에서 경험적 항생제 사용의
치료효과 및 비용에 따른 항생제 선택
중앙대학교 의과대학 비뇨기과학교실,
1진단검사의학교실
박세준∙류재형∙박상호∙최중원∙정재동∙이상협∙김정훈∙김경도∙김태형∙이미경
1[Abstract]
Selection of Antibiotics According to the Costs and Efficacy of Empirical Antibiotics Therapy for Extended Spectrum Beta-Lactamase
Producing Uropathogens from Urine Culture Test in Patients with Acute Uncomplicated Cystitis
Se Jun Park, Jae Hyung Ryu, Sang Ho Park, Jung Won Choe, Sang Hyup Lee, Jung Hoon Kim, Kyung Do Kim,
Tae Hyoung Kim, Mi-Kyung Lee
1From the Department of Urology, and 1Laboratory Medicine, College of Medicine, Chung-Ang University, Seoul, Korea
Purpose: The usage of antibiotics on urinary tract infection is high, thus, there is a high chance of ac-
quiring resistance towards antibiotics. Followed by the usage of restricted antibiotics, the emergence of
multiple drug resistant pathogens, such as ESBL producing pathogens, is frequently being reported, and
the increase of resistant pathogens leads to the increase of medical treatment costs. An effective system of
management and observation is needed for this. ESBL is an enzyme produced by gram-negative bacte-
rium, which has beta-lactam rings, that restricts the effectiveness of penicillins and cephalosporins. Such
antibiotics have been used as empirical antibiotics for acute cystitis. The effects of ESBL producing patho-
gens in patients on the curative effectiveness of empirical antibiotics are to be identified and appropriate
antibiotics will be selected, according to the results with consideration to the cost.
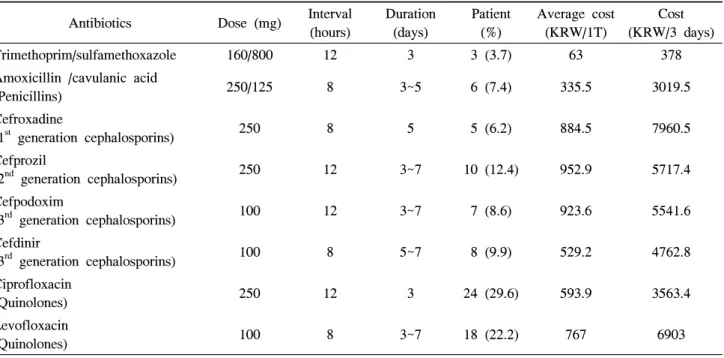
Materials and Methods: From the 4727 patients who have been diagnosed with cystitis between January 2000 and 2011 March, through urine culture test, 81 acute uncomplicated cystitis patients with ESBL pro- ducing pathogens were confirmed and their medical records were examined for this study. For 3~7 days em- pirical antibiotics, such as quinolone (ciprofloxacin / levofloxacin), cephalosporin (1st generation- cefroxadine / 2nd generation- cefprozil / 3rd generation- cefpodoxim, cefdinir), penicillin (amoxicillin-clavulanic acid), tri- methoprim-sulfamethoxazole, were used and the curative effects were confirmed through urine culture test, with the improvements on the initial symptoms. For each antibiotic, the average medical insurance cost of domestic market as of May 2011 was applied and calculation was done after averaging for 3 days.
Results: In urinalysis of 81 patients (age 44.89±17.42, 17~64), pyuria was confirmed in the urine of 79 pa- tients (97.5%) and microscopic hematuria was confirmed in the urine of 17 patients (21.0%). In urine culture test, Escherichia coli was cultured in the urine of 79 patients (97.5%) and Klebsillea pneumonia was cultured in the urine of 2 patients (2.5%). Thirty three patients (40.7%) complained of suprapubic pain, 55 patients (67.9%) of urodynia, 69 patients (85.2%) of frequent urination and 37 patients (45.7%) of urgent urination.
After taking antibiotics, not including 6 patients who have not returned, there were improvements in urine cul- ture test and symptoms in all patients. In the reexamination of urine culture test, no significant pathogens were found. According to the cost, the cost was the cheapest in the order of trimethoprim-sulfamethoxazole (160/800mg, twice a day, 3 day therapy, 378 won), amoxicillin-clavulanic acid (250/125mg, three times a day, 3 day therapy, 3019.5 won), and ciprofloxacin (250mg, once a day, 3 day therapy, 3563.4 won).
Conclusions: Even if ESBL producing pathogens were found in urine culture test of acute un- complicated cystitis patient, curative effectiveness can be expected by just taking empirical antibiotic. In concerning the objective of this study as well as the efficacy and the cost, the most appropriate primary antibiotic is trimethoprim/sulfamethoxazole. The acute uncomplicated cystitis caused by ESBL producing pathogen has the same curative effects of antibiotics of the study, having no relations with the antibiotic sensitiveness. Therefore, the empirical antibiotic with no abnormal reactions, cheap cost and short duration of treatment should be selected for the therapy. (Korean J UTII 2012;7:29-35)
Key Words: Beta-lactamase, Acute cystitis, Empirical, Antibiotic
서 론
요로감염은 일반진료에서 가장 흔한 비뇨기계 질환 중 하나이다.
1,2그 중 방광염은 요로감염에서 가장 빈번히 발생하는 질환으로 발생률 및 재발율 이 높아 항생제 사용 빈도가 증가하며, 이에 따라 항생제 내성율도 점점 높아지는 경향이 있다.
3항 생제 내성이 증가함에 따라 기존의 경험적 항생제 로 치료할 경우 상부요로감염 혹은 패혈증 등의 요 로감염 합병증 발생의 증가로도 이어질 수 있고
4이로 인하여 재원일수 증가 및 항생제 비용의 증가 를 초래할 수 있다.
5만성복잡방광염의 경우 경험 적 항생제에 내성이 높고, 배양결과에 따른 적절한 제한 항생제의 처방여부가 환자의 이환율과 사망 률 영향을 미칠 수 있다.
4,5반면 급성단순방광염은
만성복잡요로감염에 비하여 항생제 내성율이 낮아
6경험적 항생제의 사용 현황 및 효과를 확인함으로 인하여 제한 항생제의 사용을 줄이고 다재내성균 의 발생을 줄일 수 있을 것이라 생각한다.
경험적 항생제로 많이 쓰여진 페니실린계, 세팔
로스포린계 항생제는 베타락탐 링을 포함하고 있
Table 1. The usage and dose of empirical antibiotics
Antibiotics Dose (mg) Interval
(hours)
Duration (days)
Patient (%)
Average cost (KRW/1T)
Cost (KRW/3 days)
Trimethoprim/sulfamethoxazole 160/800 12 3 3 (3.7) 63 378
Amoxicillin /cavulanic acid
(Penicillins) 250/125 8 3~5 6 (7.4) 335.5 3019.5
Cefroxadine
(1
stgeneration cephalosporins) 250 8 5 5 (6.2) 884.5 7960.5
Cefprozil
(2
ndgeneration cephalosporins) 250 12 3~7 10 (12.4) 952.9 5717.4
Cefpodoxim
(3
rdgeneration cephalosporins) 100 12 3~7 7 (8.6) 923.6 5541.6
Cefdinir
(3
rdgeneration cephalosporins) 100 8 5~7 8 (9.9) 529.2 4762.8
Ciprofloxacin
(Quinolones) 250 12 3 24 (29.6) 593.9 3563.4
Levofloxacin
(Quinolones) 100 8 3~7 18 (22.2) 767 6903
KRW: Korean won, T: tablet
는데, 이러한 항생제의 주된 내성 기전은 extended- spectrum beta-lactamase (ESBL)에 의한 항생제의 비 활성이다.
7또한 지역감염 병원균으로서 전 세계적 으로 증가추세에 있어 내성균 중에서도 ESBL 생산 균주에 대한 연구는 그 중요성이 부각되고 있다.
8,9또한 ESBL 생산균주와 퀴놀론계 항생제 내성이 연 관되어 있다고 보고하는 연구들이 있다.
10따라서 본 연구는 ESBL 생산균주에 의한 급성단 순방광염 환자의 과거 의무기록을 확인하여 경험적 항생제 복용의 치료효과에 대하여 알아보고, 비용측 면에서 적합한 항생제 요법을 선택하고자 한다.
대상 및 방법
1. 환자 및 대상
이 연구는 2000년 1월부터 2011년 3월까지 11년 간 본원 비뇨기과를 방문한 환자 중 방광염으로 진 단 받은 4,727명 환자의 의무기록을 확인하여 1,104 명의 급성단순방광염 환자를 확인하였다. 그 중 소 변배양검사에서 ESBL 생산균주가 검출된 환자 81 명 (7.37%)을 대상으로 연구하였다.
2. 급성단순방광염의 정의
급성방광염의 진단기준은 Infectious Disease Society of America (IDSA)를 기초로 청결도뇨법으로 시행한 소변배양검사에서 밀리리터 당 10만개 이상의 세균 집락이 검출되고, 치골상부 동통, 배뇨통, 급박뇨, 빈 뇨 등의 증상이 하나 이상 일 때로 정의하였다.
11,12단순이라는 용어는 요로감염의 유병율, 재발율에 영 향을 미치는 이미 알고 있는 잠재된 상태, 즉 해부학 적 이상, 기능적 이상, 폐색, 내과질환 (당뇨, 만성신 부전) 등이 없는 상태로 정의하였다. 이에 따라 요로 감염이 있을 때 잠재적으로 비뇨기계의 기능장애가 있을 가능성이 있는 65세 이상의 노인 및 소아 환자, 임산부는 대상에서 제외하였다.
133. 소변검사 및 소변배양검사
대상 환자는 내원 후 경요도도뇨법을 이용하여
현미경을 포함한 소변검사와 소변배양검사를 시행
하였으며, 고배율 현미경 검사에서 백혈구가 5개
이상 보인 경우 농뇨, 적혈구가 5개 이상 보인 경
Table 2. Development and improvement of initial symptoms
Initial symptom Patients (%)
(n=82)
Symptom improvement/
follow up patients (%)
Tenderness (suprapubic area) 33 (40.7) 33/33 (100)
Dysuria 55 (67.9) 54/54 (100)
Frequency 69 (85.2) 65/67 (97.0)
Urgency 37 (45.7) 37/37 (100)
Table 3. Results of urine analysis
Initial urine Patients (n=81, %) Repeat urine Patients (n=75, %)
Pyuria (+)
(WBC ≥ 5cells/HPF) 79 (97.5) Pyuria (-)
(WBC < 5cells/HPF) 75 (100) Hematuria (+)
(RBC ≥ 5cells/HPF) 17 (21.0) Hematuria (-)
(RBC < 5cells/HPF) 75 (100) WBC: white blood cell, RBC: red blood cell, HPF: high power field
Table 4. Results of urine culture
Urine culture Initial urine (n=81, %) Repeat urine (n=75, %)
Escherichia coil (+) (> 105 CFU)
79 (97.5) 0 (0.0)
Klebsiella pneumoniae (+) (> 105 CFU)