REPO RT
http://dx.doi.org/10.11106/cet.2014.7.2.194Received April 20, 2014 / Revised May 19, 2014 / Accepted June 3, 2014
Correspondence: Mi Ri Lee, MD, PhD, Department of Surgery, Dong-A University Medical Center, Daeshin Park road 26, Seo-gu, Busan 602-715, Korea
Tel: 82-51-240-2979, Fax: 82-51-247-9316, E-mail: [email protected] This work was supported by the Dong-A University research fund.
Copyright ⓒ 2014, the Korean Thyroid Association. All rights reserved.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http:// creative- commons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Axillary Lymph Node Metastasis of Papillary Thyroid Carcinoma: A Case Report
Eun Jung Koo
1and Mi Ri Lee
2Department of Surgery, Hallym Sacred Heart Hospital, Seoul1, Department of Surgery, Dong-A University Medical Center, Busan2, Korea
We report a case of axillary lymph node metastasis (LNM) as a recurrence of papillary thyroid carcinoma (PTC) in a 68-year-old male. The patient initially presented in 2009 with a 3.4×5.4 cm sized neck swelling and left cervical lymphadenopathy. He underwent total thyroidectomy and central compartment neck dissection (CCND) with left modified radical neck dissection (MRND). The pathological report confirmed PTC with metastasis of neck lymph node. On a regular follow up of positron emission tomography (PET), LNM was found on the right supraclavicular area and on the left axillary area. It was 17 months after the initial thyroid cancer had been diagnosed. The right MRND and left axillary lymph node dissections were performed in April of 2012.
Pathological result confirmed metastatic PTC of left axillary lymph nodes. After recovery from the surgery, the patient got radioactive iodine therapy with I-131 180 mCi.
Key Words: Axillary lymph nodes metastasis, Papillary thyroid carcinoma
Introduction
Papillary thyroid carcinoma (PTC) is the most common thyroid malignancy and an indolent neoplasm with an excellent prognosis, despite its characteristically being associated with lymph node metastasis (LNM). Cervical LNM is common, but axillary LNM is rare and very few cases have been reported. We report a case of axil- lary LNM from PTC.
Case Report
A 68-year-old male patient visited the Family Medicine Clinic with a complaint of palpable mass on his left neck in 2009. He was transferred to the Depa- rtment of Otorhinolaryngology for further evaluation.
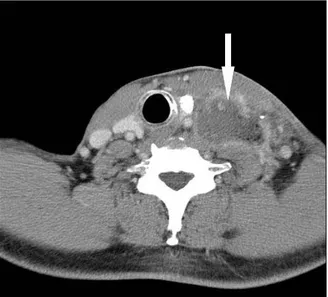
Thyroid function tests results including TSH (0.6 μ IU/mL; reference range, 0.3-4.1 μIU/mL), free T4 (1.44 ng/dL; reference range, 0.78-1.94 ng/dL), T3-RIA (117.3 ng/dL; reference range, 60-190 ng/dL) were normal. But, thyroglobulin antigen (Tg-Ag) was high (>500 ng/mL; reference range, 5-45 ng/mL), the level of thyroglobulin antibody (Tg-Ab) (28.74 IU/mL; reference range, 0-70 IU/mL) was normal. The tumor marker CA 19-9 was highly elevated at 459.22 (normal, 0-37 U/mL), but there was no evidence of another cancer (e.g. colon cancer or pancreatic can- cer) on abdomen computed tomography (CT) and abdominal ultrasonographic finding. Colonoscopy was not performed. The initial neck CT showed 3.4×5.4 cm sized mass with heterogeneous enhancement over the left lower neck and left supraclavicular area (Fig. 1). Differential diagnosis on CT was metastatic
Fig. 1. Neck CT showing large mass in left lower neck carotid space, metastatic lymphadenopathy and left thyroid nodule.
Fig. 2. I-123 5 mCi whole body scan showing normal functioning thyroid tissue in both thyroid gland and cold nodule in left thyroid lobe.
lymphadenopathy or neurogenic tumor such as sch- wannoma or paraganglioma. Fine needle aspiration (FNA) of neck mass presented a few atypical epithelial cell nests in acute inflammatory exudate. To rule out malignancy, incisional biopsy of lymph nodes was carried out. Pathological examination of the lymph no-
des on the left lower neck and left supraclavicular area confirmed the metastasis of PTC. Small calcifica- tion was seen on the precontrast scan. I-123 5 milli- curie (mCi) whole body scan presented normal func- tioning thyroid tissue in both thyroid glands and cold nodule in the left lobe (Fig. 2). The result of FNA of thyroid was suspicious for malignancy, especially of PTC. Therefore, the patient received a total thyroi- dectomy with central compartment neck dissection (CCND) and left modified radical neck dissection (MRND). Pathological test resulted in the diagnosis of PTC with follicular variant of ossification and metastasis of level III, IV, and V neck lymph node, of central com- partment lymph node, and of external jugular area lymph node. The size of the tumor was 1.5×1.2 cm, but it invaded to perithyroidal soft tissue. So the stage was T3N1bM0. After the surgery, the level of Tg-Ag was 4.26 ng/mL and that of Tg-Ab was 27.44 IU/mL (Table 1). The patient received radioactive iodine ther- apy with I-131 150 mCi. The 150 mCi therapeutic whole body scan at 48 hour, reveals two intense ac- cumulation of the I-131 in the mid thyroid bed and remnant pyramidal lobe, with a focal much less I-131
Fig. 3. 151 mCi therapeutic whole body scan at 48 hours showing two intense accumulation of the I-131 in the mid thyroid bed and remnant pyramidal lobe, with a focal much less I-131 uptake in the left upper thyroid bed or neck lymph node.
Table 1. The serial level of Tg-Ag and Tg-Ab
Tg-Ag Tg-Ab
After the initial surgery Follow-up
After axillary and right supraclavicular lymph nodes metastasis After the second* surgery At present
4.26 17.78
>1000
314.98 24.63
27.44 43.06 36.66
12.05 8.1 Tg-Ag: thyroglobulin antigen, Tg-Ab: thyroglobulin antibody
*axillary dissection and right modified radical neck dissection uptake in the left upper thyroid bed or neck lymph node (Fig. 3). Diagnostic I-131 scan performed 6
months after a radioiodine ablation therapy. There was no longer iodine uptake in the thyroid bed (Fig. 4).
Seventeen months later, an enlargement of the left ax- illary and right supraclavicular lymph nodes were de- tected on chest CT during the regular follow up.
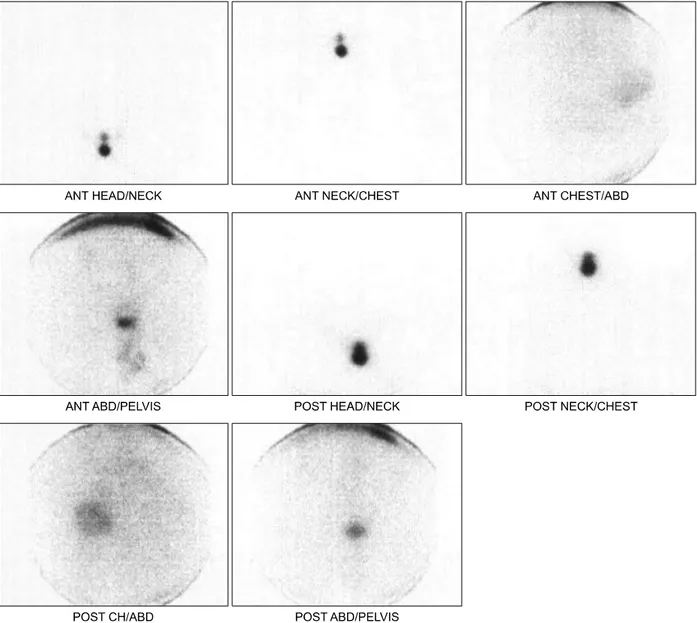
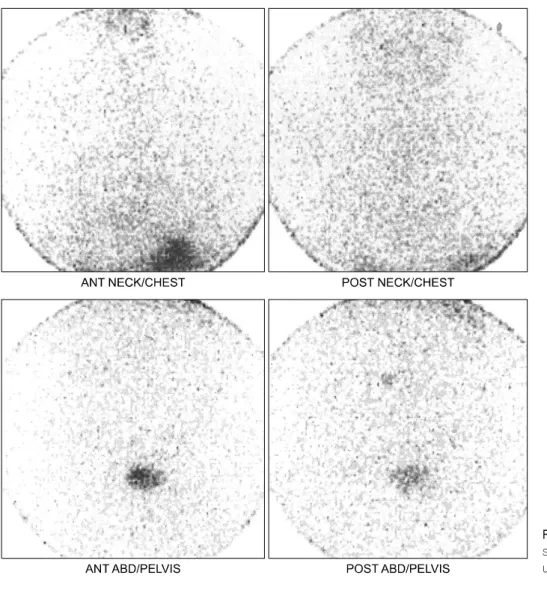
Moreover, there were hypermetabolic metastatic lymph nodes in the right supraclavicular and left axillary area in 18F-FDG positron emission tomography (PET) (Fig. 5). Ultrasonography guided FNA diagnosed LNM of PTC in both in left axillary and right supraclavicular area. Thus, a second operation was urgently required, and the right M RND and left axillary lymph node dissections were performed in April 2012 (Fig. 6).
Fig. 4. Diagnostic I-131 scan showing no longer iodine uptake in the thyroid bed.
Fig. 5. PET showing hypermetabolic metastatic lymph nodes in right suprclavicular (A) and left axillary area (B).
Pathological results confirmed the metastatic PTC (tall cell variant) of the left axillary lymph nodes (Fig. 7).
Malignancy was not seen in the right neck lymph nodes. After recovery from the surgery, the patient re- ceived radioactive iodine therapy with I-131 180 mCi.
The therapeutic whole body scan reveals well uptake of residual thyroid tissue in both thyroid bed (Fig. 8).
It was 9 months after his second surgery when the metastasis of bone, especially on level 2 of the thora- cic spine (T2), was found on PET CT during the regu-
Fig. 8. The therapeutic whole body scan reveals well uptake of residual thyroid tissue in both thyroid bed.
Fig. 7. The tumor shows papillary growths with numerous branches (H&E stain, x10) (A). The papillae of the tumor are lined by single layer or pseudostratified tall columnar cells with elongated nuclei (H&E stain, x200) (B).
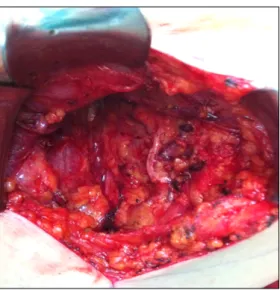
Fig. 6. Intraoperative finding of axillary lymph node dissection.
lar follow up. At that time the level of Tg-Ag was 376.46 ng/mL and that of Tg-Ab was 4.88 IU/mL.
The patient received novalis stereotactic radiotherapy (RT) on T2 (total RT dose: 4000 cGy). One year after RT, 18F-FDG PET shows normal glucose metabolism on bones and soft tissue, the level of Tg-Ag was 24.63 ng/mL and that of Tg-Ab was 8.1 IU/mL.
Discussion
Axillary masses suggest various diseases involving tumors, inflammatory conditions, and infections. Breast cancer is a major disease of axillary metastasis, so the
probability of breast malignancy must be ruled out when the axillary masses are detected. Other tumors may involve the axillary lymph nodes, such as in lymphoma, melanoma, cancers of the head and neck, and occasionally carcinomas from various primary sites.1,2) Metastasis in breast cancer commonly occurs in the axillary lymph node; however, it is not known as the potential site for thyroid cancer metastasis.
A case diagnosed with PTC synchronous with breast cancer has been reported.3) In our case, meta- stasis of axillary lymph nodes and contralateral lymph node occurred 17 months after the first diagnosis of PTC. There was no evidence of breast cancer on chest CT and 18F-FDG PET. Breast ultrasonography was not performed. However, pathologic morphologic characteristics of axillary LNM in this case are different from those of papillary type of breast cancer. Furthe- rmore, after left axillary lymph node dissections and right M RND, the level of Tg-Ag was decreased significantly (Table 1).
Axillary lymph nodes are a rare manifestation of thyroid carcinoma; only 18 cases are in the published literature. Eighteen reports of axillary LNM from thyroid cancer exist in the literature: 12 PTC, 2 mucoepidermoid carcinoma variants, 2 medullary thyroid carcinoma, and 1 each of follicular thyroid carcinoma, and poorly differentiated mucin-producing adenocarcinoma.4-11) Our study reports the case of PTC metastatic to axil- lary lymph nodes.
Some authors reported a case of the axillary lymph node recurrence in papillary thyroid microcarcinoma.
The patient had severe swelling of the cervical lateral lymph node preoperatively, which is indicative of a poor prognosis.5) Our report is also agreement with this studies. Nine month after of the second surgery, the bone metastasis developed.
Other authors reviewed 9 cases of PTC with axillary LNM and described poor outcomes of the axillary LNM in PTC patients. In the 6 reports, all of the patients had poorly differentiated components, suggesting that the axillary LNM may be associated with poorly differentiated thyroid carcinoma. Seven out of the nine patients had synchronous or metachronous distant metastasis, and only one patient was reported to survive without the
disease.6) There was no synchronous distant meta- stasis in our report, but metachronous bone metastasis developed. However, the patient is still alive with disease after RT.
Krishnamurthy et al.7) summarized 7 reports written in English, describing the axillary LNM in PTC. The patients with axillary metastatic lesions predominantly had poorly differentiated tumors. He also mentioned that the axillary LNM of PTC might be related to poor prognosis.
Rouvière12) reported about the communication be- tween the cervical and axillary lymphatics in 1932, but concluded that the physiologic flow is centripetal to the jugulosubclavian junction. However, malignant tumors can change and partially block lymphatic pathways, potentially resulting in axillary LNM in a retrograde direction. Although the altered lymphatic flow is mainly due to blockage of the lymph nodes by metastasis, fibrosis at the jugulosubclavian junction due to ex- tensive lymph node dissection or RT can also result in anomalous lymphatic dissemination to the ax- illa.5-10,13) Moreover, with repeated recurrences, PTCs can be transformed into poorly differentiated carcino- mas or into histological variants associated with worse prognosis,7) as seen in our patient.
In our case, metastasis of axillary lymph node and contralateral lymph node occurred 17 months after the first diagnosis of PTC on chest CT and 18F-FDG PET.
Papillary carcinoma of follicular variant and mixed histologic type thyroid carcinomas tend to cause distant lymph node and organ metastases more fre- quently than papillary carcinomas of classic type.
About 20% of patients with high serum Tg have neg- ative 131I whole body scans which may be due to small size of the metastatic tumor, loss of differentiation of cancer cells leading to low iodine uptake, or poor TSH stimulation. 18F-FDG PET can detect foci of me- tastasis in patients with negative 131I whole body scan and high serum thyroglobulin.11) Therefore, 18F-FDG PET is very important during follow-up period as well as 131I whole body scans. Moreover, 9 month after of the second surgery, the bone metastasis developed.
However, the patient is still alive with disease after RT.
Axillary LNM of PTC is rare, but its possibility should
be kept in mind. Axillary LNM may be an indicator of systemic disease and a poor prognosis. Thus the pa- tients with axillary LNM of PTC need intensive strat- egies to treat a chain of metastasis or the recurrence of disease.
References
1) Ers V, Galant C, Malaise J, Rahier J, Daumerie C. Axillary lymph node metastasis in recurrence of papillary thyroid carcinoma:
a case report. Wien Klin Wochenschr 2006;118(3-4):124-7.
2) Jaffer S, Goldfarb AB, Gold JE, Szporn A, Bleiweiss IJ.
Contralateral axillary lymph node metastasis as the first evidence of locally recurrent breast carcinoma. Cancer 1995;75(12):2875-8.
3) Banzo J, Ubieto MA, Gonzalez C, Razola P, Tardin L, Andres A, et al. [Papillary thyroid carcinoma synchronous with breast cancer: an incidental finding in an (18)F-FDG PET-CT study carried out in a search for occult breast cancer]. Rev Esp Med Nucl Imagen Mol 2012;31(4):213-5.
4) Cummings AL, Goldfarb M. Thyroid carcinoma metastases to axillary lymph nodes: report of two rare cases of papillary and medullary thyroid carcinoma and literature review. Endocr Pract 2014;20(3):e34-7.
5) Koike K, Fujii T, Yanaga H, Nakagawa S, Yokoyama G, Yahara T, et al. Axillary lymph node recurrence of papillary thyroid microcarcinoma: report of a case. Surg Today 2004;
34(5):440-3.
6) Nakayama H, Wada N, Masudo Y, Rino Y. Axillary lymph node metastasis from papillary thyroid carcinoma: report of a case. Surg Today 2007;37(4):311-5.
7) Krishnamurthy A, Vaidhyanathan A. Axillary lymph node metastasis in papillary thyroid carcinoma: report of a case and review of the literature. J Cancer Res Ther 2011;7(2):220-2.
8) Chiofalo MG, Losito NS, Fulciniti F, Setola SV, Tommaselli A, Marone U, et al. Axillary node metastasis from differentiated thyroid carcinoma with Hurthle and signet ring cell differentiation.
A case of disseminated thyroid cancer with peculiar histologic findings. BMC Cancer 2012;12:55.
9) Kepenekci I, Demirkan A, Cakmak A, Tug T, Ekinci C.
Axillary lymph node metastasis as a late manifestation of papillary thyroid carcinoma. Thyroid 2009;19(4):417-9.
10) Wada N, Duh QY, Sugino K, Iwasaki H, Kameyama K, Mimura T, et al. Lymph node metastasis from 259 papillary thyroid microcarcinomas: frequency, pattern of occurrence and recurrence, and optimal strategy for neck dissection. Ann Surg 2003;237(3):399-407.
11) Elboga U, Kalender E, Yilmaz M, Celen YZ, Aktolun C.
Axillary lymph node metastasis of papillary thyroid carcinoma detected by FDG PET/CT in a thyroglobulin-positive patient with negative whole-body 131I scan. Clin Nucl Med 2012;
37(11):1120-2.
12) Rouvière H. Anatomie des lymphatiques de L'homme. Paris:
Masson; 1932.
13) Mazzaferri EL, Young RL. Papillary thyroid carcinoma: a 10 year follow-up report of the impact of therapy in 576 patients.
Am J Med 1981;70(3):511-8.