198
Copyrights © 2015 The Korean Society of RadiologyINTRODUCTION
The thyroid gland is one of the most vascular organs of the body. However, the clinical and surgical series have reported an incidence of secondary malignancies in this gland of only 3%.
Nevertheless, thyroid metastasis is not an exceptional finding; at autopsy, it is encountered in a variable proportion (2% to 24%) of patients affected by a malignant neoplasm (1).
The most common primary sites are the kidney, lung, breast, and gastrointestinal tract (2). However, a variety of cancers may metastasize to the thyroid, including nasopharyngeal carcinoma, choriocarcinoma, osteosarcoma, leiomyosarcoma, liposarcoma, melanoma, and tumors of neuroendocrine origin. Review of the literature on hepatocellular carcinoma (HCC) metastasized to the thyroid identified four such cases (3, 4). However, to the best of our knowledge, this is the first radiologic report.
Thyroid nodules found in patients who have malignant disease could be benign, second primary malignancy or metastasis from other organs. High-resolution ultrasonography (US) is highly sensitive for the detection of thyroid nodules that are not even palpable on clinical examination, and it plays a major role in guid- ing fine-needle aspiration of such lesions (5). We report a rare case of a HCC metastatic to the thyroid and discuss the sono- graphic findings of thyroid metastasis arising from non-thyroid primaries. The likely difficulties encountered in such patients from diagnosis to evaluation of thyroid disease are discussed.
CASE REPORT
A 53-year-old man diagnosed with liver abscess 3 years ago was admitted for epigastric discomfort (Fig. 1A). The serum al- pha-fetoprotein level was 2700 ng/mL. Subsequent liver com-
Case Report
pISSN 1738-2637 / eISSN 2288-2928 J Korean Soc Radiol 2015;72(3):198-201 http://dx.doi.org/10.3348/jksr.2015.72.3.198
Received September 11, 2014; Accepted November 25, 2014Corresponding author: Noh Hyuck Park, MD Department of Radiology, Myongji Hospital, 55 Hwasu-ro 14beon-gil, Deogyang-gu, Goyang 412-270, Korea.
Tel. 82-31-810-7164 Fax. 82-31-810-6537 E-mail: nhpark904@cku.ac.kr
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distri- bution, and reproduction in any medium, provided the original work is properly cited.
Although the thyroid gland is one of the most vascular organs of the body, meta- static disease in the thyroid is encountered infrequently. However, at autopsy, the incidence rate of thyroid metastasis ranges from 1.25% to 24%. The primary sites are the kidney, lung, breast, and gastrointestinal tract. We report a rare case of a hepatocellular carcinoma metastatic to the thyroid gland. The patient had multiple palpable masses in the anterior and left lateral neck along the internal jugular chain on physical examination 9 months after the initial diagnosis of liver tumor. These masses were confirmed as metastasis from hepatocellular carcinoma by ultraso- nography-guided 16-G core needle biopsy. We discuss the sonographic findings of thyroid metastasis and their use as an additional aid for differentiating between unknown primary tumor and thyroid metastasis.
Index terms Metastasis Ultrasound
Hepatocellular Carcinoma Thyroid
Ultrasonography Findings of Thyroid Metastasis in a Patient with Hepatocellular Carcinoma: A Case Report
1간세포암의 갑상선 전이의 초음파: 증례 보고1
Kyung Ho Kim, MD
1, Noh Hyuck Park, MD
1, Jae Hoon Lim, MD
1, Chan Sub Park, MD
1, Su Ok Seong, MD
1, Tae Jung Kwon, MD
2Departments of 1Radiology, 2Pathology, Myongji Hospital, Goyang, Korea
Kyung Ho Kim, et al
199
jksronline.org J Korean Soc Radiol 2015;72(3):198-201
due to direct invasion of the tumor were noted (Fig. 1B, C). Un- derlying conditions were chronic hepatitis B infection, atrial fi- brillation, and heart failure. Physical examination was negative for spider angioma, shifting dullness, jaundice or scleral icterus, hand flapping tremor, or palpable neck mass. Laboratory data puted tomography (CT) showed a mass with arterial enhance-
ment and delayed washout pattern on dynamic enhancement, which was highly suggestive of HCC; it had been considered to be a liver abscess previously, and tumor thrombosis in the right hepatic vein and intrahepatic segment of the inferior vena cava
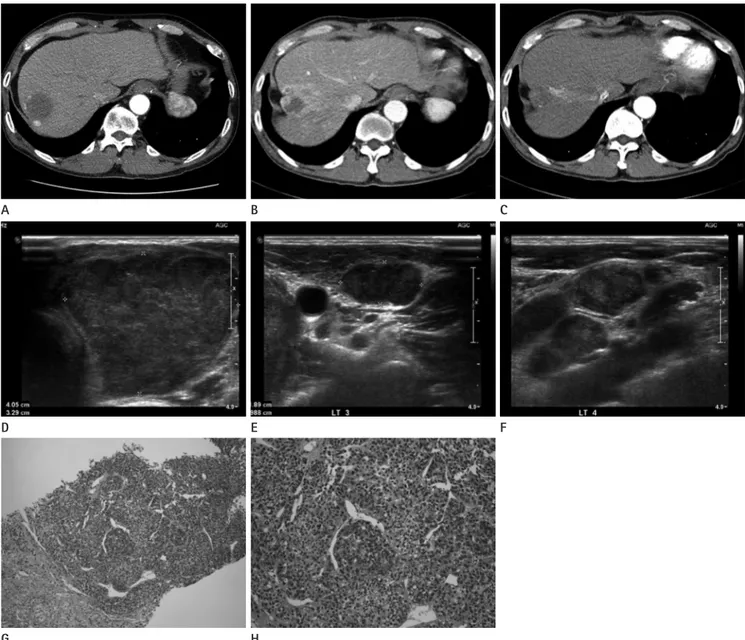
Fig. 1. Hepatocellular carcinoma with thyroid metastasis in a 53-year-old male patient.
A. Initial CT taken 3 yrs ago. A low density hepatic mass 3.8 × 3.5 cm in size was noted in segment 7 of the liver. This mass was regarded as a liv- er abscess.
B, C. Follow-up CT scans. A 8.4 × 2 cm elongated mass was noted in the right hepatic lobe with invasion of right hepatic vein showing arterial enhancement and delayed washout pattern of enhancement. The findings were highly of hepatocellular carcinoma. Tumor thrombosis of right hepatic vein and intrahepatic segment of inferior vena cava were evident.
D. A 4 cm sized homogenous hypoechoic solid mass replaced the left thyroid lobe. The masses in the thyroid gland showed heterogenous hy- poechoic features without necrosis or calcification.
E, F. Enlarged pathologic lymph nodes, left level 3 and 4 were evident. The nodes showed the same nature as the thyroid masses. No significant increase of intratumoral or intranodal vascularity was found on color Doppler study–denotes metastatic lymph nodes.
G. Typical trabecular pattern of tumor cells (hematoxylin & eosin stain, × 100).
H. Higher magnification of tumor cells showing pleomorphic cells with nuclear atypia (hematoxylin & eosin stain, × 200).
H E B
G D A
F C
Ultrasonography Findings of Thyroid Metastasis in a Patient with Hepatocellular Carcinoma
200
J Korean Soc Radiol 2015;72(3):198-201 jksronline.organd generally associated with evidence of widespread malignant disease. However, symptoms such as dysphagia, stridor, hoarse- ness, or palpable neck mass may be present (8, 9). Our patient presented with multiple palpable neck masses in the anterior neck and left lateral neck along the internal jugular chain.
US findings that indicate a high possibility of metastasis to the thyroid are nodules with ill-defined hypoechoic character and heterogeneous echotexture, and no evidence of microcalcifica- tion (10). In the present case, US showed heterogeneous, hy- poechoic echogenicity without necrosis or calcification, but, the margins of masses were well-circumscribed and their shape was wider than tall, which could mimic a benign nodule. A patient with these sonographic findings who has an underlying malig- nancy should be considered for US-guided biopsy.
We confirmed thyroid metastasis from HCC with a 16-gauge core needle biopsy under ultrasound guidance because it may be difficult to distinguish primary from metastatic disease with fine needle biopsy when the cells are highly anaplastic, or the tissue shows histological architecture resembling that of a pri- mary tumor (1).
Immunohistochemistry can also be helpful for correctly iden- tifying undifferentiated cancers. Since only 20–30% of anaplastic thyroid carcinomas are positive for thyroid markers such as thy- roglobulin, it is important to be aware of primary malignancies for appropriate marker staining (1). Although immunostaining for thyroglobulin was not performed in this case, hematoxylin and eosin staining showed typical histologic features of HCC.
HCC tumor cells were positive for epithelial membrane antigen and cytokeratin, and negative for carcinoembryonic antigen.
We concur with the previous recommendation that all pa- tients with a history of cancer should be evaluated for possible metastasis when a thyroid lesion is discovered (6).
The sonographic findings of thyroid metastasis from HCC in the present case were multiple, heterogeneous, hypoechoic, solid masses without significantly increased intratumoral vascularity, wider than tall in shape, no calcification or cystic changes, well- circumscribed margins, which are not typical benign or malig- nant findings. However, findings such as wider than tall in shape, well-circumscribed margins, no calcification, or significant intra- tumoral vascularity can be the findings that differentiate metas- tasis from primary thyroid malignancy. US-guided core needle biopsy with additional use of immunohistochemistry is helpful revealed serum aspartate aminotransferase level of 54 IU/L, ala-
nine aminotransferase level of 10 IU/L, and creatinine level of 1.0 mg/dL. Transarterial embolization therapy was performed for the infiltrative tumor with a hepatic vein tumor thrombus and multiple tumors in the right lobe.
Nine months after the initial diagnosis of liver tumor, multiple masses were palpated in the anterior and left lateral neck along the internal jugular chain on physical examination. US per- formed to evaluate neck masses revealed multiple, variable-sized solid masses in the thyroid gland and enlarged lymph nodes along the left internal jugular chain (Fig. 1D-F). The masses in the thyroid gland showed echo features with heterogeneous, hy- poechoic solid echogenicity without necrosis or calcification. The margins of the masses were well-circumscribed and they had a wider than tall shape. The lymph nodes appeared similar to the thyroid masses. No significant increase in the intratumoral or in- tranodal vascularity was found on the color Doppler study.
US-guided 16-gauge core needle biopsy was performed for the left thyroid mass and a pathologic lymph node at the left level 3.
Histopathologic examination of the thyroid gland and lymph node showed similar histologic features, suggestive of metastatic HCC. The tumor cells had a typical trabecular pattern with a network of sinusoidal vessels, scanty cytoplasm, and nuclear pleomorphism (Fig. 1G, H). Additionally, immunohistochemi- cal staining was positive for epithelial membrane antigen and cytokeratin, and negative for carcinoembryonic antigen.
The patient expired 20 days after the diagnosis of thyroid me- tastasis, due to hepatorenal syndrome.
DISCUSSION
Metastatic spread to the thyroid gland may be more common than primary malignant tumors of thyroid origin among pa- tients with a history of a malignant neoplasm (6).
Primary tumors that most frequently metastasize to the thy- roid gland are those that most often give rise to hematogenous metastasis, such as malignant melanoma, renal, breast, and lung carcinoma, and less frequently, secondary lesions from pancre- atic and gastrointestinal malignancies (3). However, there are few case reports about thyroid metastases of HCC (7).
Metastatic lesions of the thyroid and neck usually do not pres- ent important clinical problems because they are mostly small
Kyung Ho Kim, et al
201
jksronline.org J Korean Soc Radiol 2015;72(3):198-201
of ultrasonography and fine needle aspiration biopsy. J Clin Ultrasound 1989;17:657-660
6. Wood K, Vini L, Harmer C. Metastases to the thyroid gland:
the Royal Marsden experience. Eur J Surg Oncol 2004;30:
583-588
7. Mirallié E, Rigaud J, Mathonnet M, Gibelin H, Regenet N, Hamy A, et al. Management and prognosis of metastases to the thyroid gland. J Am Coll Surg 2005;200:203-207 8. Masuda T, Fukuya T, Ono M, Mitsuyama S, Toyoshima S.
Thyroid metastasis from hepatocellular carcinoma as an initial presentation: a case report. Radiat Med 2001;19:43- 46
9. Shimaoka K, Sokal JE, Pickren JW. Metastatic neoplasms in the thyroid gland. Pathological and clinical findings. Can- cer 1962;15:557-565
10. Chung SY, Kim EK, Kim JH, Oh KK, Kim DJ, Lee YH, et al.
Sonographic findings of metastatic disease to the thyroid.
Yonsei Med J 2001;42:411-417 for differentiating metastasis from primary malignancies.
REFERENCES
1. Chen H, Nicol TL, Udelsman R. Clinically significant, isolat- ed metastatic disease to the thyroid gland. World J Surg 1999;23:177-180; discussion 181
2. Nakhjavani MK, Gharib H, Goellner JR, van Heerden JA.
Metastasis to the thyroid gland. A report of 43 cases. Can- cer 1997;79:574-578
3. Liang HH, Wu CH, Tam KW, Chai CY, Lin SE, Chen SC. Thy- roid metastasis in a patient with hepatocellular carcino- ma: case report and review of literature. World J Surg On- col 2007;5:144
4. Katyal S, Oliver JH 3rd, Peterson MS, Ferris JV, Carr BS, Baron RL. Extrahepatic metastases of hepatocellular carci- noma. Radiology 2000;216:698-703
5. Eftekhari F, Peuchot M. Thyroid metastases: combined role
간세포암의 갑상선 전이의 초음파: 증례 보고1
김경호
1· 박노혁
1· 임재훈
1· 박찬섭
1· 성수옥
1· 권태정
2갑상선은 우리 몸에서 가장 혈류가 많은 장기 중 하나임에도 불구하고, 갑상선의 전이암은 드물다. 암 환자에서 갑상선으 로 전이되는 비율은 1.25~24%로 일반적인 생각과는 다르게 낮은 편이다. 갑상선으로 전이되는 암 중 가장 많은 것은 콩 팥, 폐, 유방, 위장관계암이다. 그 중에서 간암의 갑상선 전이는 매우 드문 것으로 알려져있다. 여기서는 간암으로 진단되 고 9개월 후 목에 만져지는 종괴로 조직검사상에서 간암의 갑상선 전이로 확인된 증례 보고를 하고 갑상선의 원발암과 전 이암 감별에 도움을 줄 수 있는 초음파적 소견과 다른 도움이 될만한 소견에 대해 말하고자 한다.
명지병원 1영상의학과, 2병리과