ARTICLE
https://doi.org/10.11106/ijt.2018.11.2.99Received September 10, 2018 / Accepted October 19, 2018
Correspondence: Guk Haeng Lee, MD, PhD, Department of Otorhinolaryngology-Head & Neck Surgery, Korea Cancer Center Hospital, KIRAMS, 75 Nowon-ro, Nowon-gu, Seoul 01812, Korea
Tel: 82-2-970-1272, Fax: 82-2-970-2450, E-mail: [email protected]
Copyright ⓒ 2018, the Korean Thyroid Association. All rights reserved.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creative- commons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
국소 진행된 갑상선암의 수술 – 기관 및 후두, 식도 침범의 치료
원자력병원 이비인후과
이국행, 강주용
Surgical Treatment in Locally Advanced Thyroid Cancer – Trachea, Larynx, Esophagus Invasion Management
Guk Haeng Lee and Ju Yong Kang
Department of Otorhinolaryngology-Head & Neck Surgery, Korea Cancer Center Hospital, KIRAMS, Seoul, Korea
Most thyroid cancers are well-differentiated cancers and have a very good prognosis. About 10% of thyroid cancer, however, invades the surrounding tissues, causing local recurrence and distant metastasis, and eventually affecting survival rate. In locally advanced thyroid cancers, the invasion of trachea, larynx and esophagus, can be occurred by primary tumor and may also result in lymph nodes metastasis. Surgical resection is still mainstay for the treatment of locally advanced thyroid cancer. The main purpose of the surgical resection is to eliminate the cancer completely, therefore, it can cause many complications such as dysfunction of the larynx, trachea and esophagus. It can have a serious effect on the quality of life, therefore there is still controversy on the extent of the surgery. The authors compare and analyze the opinions which were already discussed in the literatures published so far. These will help to select the surgical method.
Key Words: Locally advanced thyroid cancer, Larynx, Trachea, Esophagus
서 론
갑상선암이 치료의 논란을 일으킬 정도로 천천히 자 라고 예후가 좋은 암이라는 데는 이견이 없을 것이다.
하지만 일부의 갑상선암은 갑상선 주위의 조직을 침범 하여 갑상선뿐만 아니라 주변 구조물의 제거로 인한 구조적, 기능적 장애를 초래할 수 있는 침습성을 보인 다. 이렇게 국소적으로 진행된 갑상선암은 수술로써 완전히 절제하는 것이 일차 목표이지만 이 과정에서 발생할 수 있는 여러 가지 문제로 인해 치료를 어렵게 하고 후유증과 재발 등으로 인해 환자의 삶의 질을 떨
어뜨리는 결과를 초래할 수 있다. 그리고 나아가 환자 의 예후에도 영향을 미치고 원격전이와 더불어 생존율 을 떨어뜨리는 중요한 인자가 된다.1-3)
갑상선의 주위에는 근육, 후두, 기관, 식도 등의 중요 한 구조물이 있고, 이들의 기능을 유지하는 신경과 혈 관이 복잡하게 구성되어 있다. 이들을 침범하는 국소 진행성 갑상선암의 근본적인 치료는 완전한 수술적 절 제와 방사성 동위원소 치료, 혹은 경우에 따라서는 외 부 방사선 조사를 추가하는 것이다. 수술 시 절제연에 종양이 없도록 완전히 절제하는 것이 가장 좋은 치료 법이지만 중요한 구조물을 절제하는 것은 심각한 기능 손실을 초래할 수 있기 때문에 절제 범위에 대해서는
Table 1. Invasion sites of locally advanced thyroid cancer
Sites Incidence (%)
Strap muscles 52-66
Recurrent laryngeal nerve 36-46
Trachea 20-40
Larynx 11-20
Hypopharynx/Esophagus 5-20
Etc. (other nerves & vessels) 1-2 논란이 있다. 일부에서는 침범된 구조물을 포함하여
종양을 육안적으로 완전히 제거하고 술 후 방사선 동 위원소 치료나 외부 방사선 조사를 시행하는 것을 선
호한다.1,4,5) 그러나 침범된 부위를 포함하여 2-3 mm 이
상의 충분한 절제연을 가지고 종양을 완전히 절제하는 것이 국소 제어율과 생존율을 높일 수 있기 때문에 적 극적인 수술을 주장하는 술자들도 있다.6-9)
이렇듯 절제 범위에 대해서는 논란이 있으나, 분화 갑상선암의 특성을 고려할 때 국소 진행성 갑상선암의 수술 원칙은 가능하면 종양을 모두 제거하면서 주변 구조물의 기능을 최대한 보존하는 것이다. 그러므로 환자의 특성과 종양의 특성, 술자의 특성 등을 고려하 여 환자 개개인에게 가장 좋은 결과를 얻을 수 있는 수술 방법을 찾아야 하겠다.
본 론
수술 전 평가 및 준비
갑상선 초음파검사는 갑상선 종물의 크기나 위치를 판단하고 세침흡인 세포검사를 통해 갑상선암을 진단 하는 데 유용하여 갑상선암 일차 검사로 널리 사용되 고 있다.
종양의 크기가 크거나 목소리가 변한 경우 등 국소 침범이 의심되는 경우에는 수술 전에 컴퓨터단층촬영 (computed tomography, CT)이나 자기공명영상(magnetic resonance imaging, MRI)을 통해 종양과 주변 구조물과 의 관계를 파악해야 한다. 만약 갑상연골, 기관, 식도 등의 침범이 의심된다면 수술 전에 침범 부위의 절제 에 따른 적절한 재건 방법을 준비하고 환자와의 면밀 한 상담을 시행해야 한다.
만약 영상 검사에서 기관이나 식도 내로 침범이 의 심된다면 추가적으로 기관지 내시경이나 식도 내시경 을 통해 내부 침범 여부를 확인하는 것이 좋다. 이는 기관이나 식도 내로 종양이 침범된 경우에는 종양을 포함하여 침범된 부위의 분절 절제(segmental resection) 가 필요한 경우가 많으므로 재건방법을 결정하는 데 도움을 주기 때문이다.
수술 전 국소 진행성 갑상선암이 의심된다면 환자 및 보호자에게 수술 전 구조물 손상에 대한 동의서 (informed consent)를 받고, 수술 전 필요한 경우에 비 위영양관(nasogastric feeding tube)을 사전에 위치시키 고 수술 중 신경 감시장치(intraoperative neuromoni- toring, IONM)를 준비하여 만일의 경우에 대비하여야
한다.10)
국소 침범한 갑상선암의 경우 경부 림프절의 전이나 폐, 뼈 등으로의 전신 전이가 잘 발생하므로 수술 전에 경부나 전신 전이에 대한 검사를 시행하는 것이 필요 하다. 전이가 의심되는 경부 림프절은 초음파 유도 세 침흡인 세포검사를 시행하여 전이 여부를 확인할 수 있으며, 복부 및 흉부 CT, 골스캔 등을 시행하여 전신 전이 여부를 확인할 수 있다. 종양이 방사선요오드 섭 취가 잘되는 경우가 많으므로 131I 스캔이 전이 부위를 확인하는 데 유용하게 사용할 수 있으며, 양전자방출 단층촬영(positron emission tomography, PET)을 통해 서 전신 전이 여부를 확인할 수 있다.10)
부위별 수술
분화갑상선암(Differentiated thyroid cancer)에서 갑 상선 외 국소 침범을 보이는 경우는 약 6-13% 정도로 보고되고 있으며, 국소 재발, 경부 림프절 전이, 원격 전이 등과 관련이 있고, 사망에 이르기도 하기 때문에 예후가 나쁜 것으로 알려져 있다.11,12) 나이가 많거나 남 자, 병리 조직학적으로 변형된 형태의 유두암에서 잘 발생한다. 가장 흔하게 침범하는 구조는 피대근, 반회 후두신경, 기관, 식도, 후두 등이다(Table 1).1,3,7) 이러한 국소 침범의 많은 부분은 갑상선 종양 자체에 의한 직 접 침범이지만, 전이 림프절에 의한 침범을 통해서도 발생할 수 있다.1,13)
1) 기관
갑상선 암종의 후두, 기관 침범의 기전에 대해서 1990년 McCaffrey 등5)은 기관 주변 림프절로 전이된 암 조직이 기관으로 침범하는 것이 주된 경로라고 하였다.
반면에 1993년 Shin 등14)은 전이성 병변이 아닌 갑상선 암종 자체가 기관을 직접 침범한다고 하였고, 그 이유 로 림프관 내에 암 조직이 발견된 경우는 드물고, 대부 분 기관연골 사이의 섬유조직을 밀고 들어오면서 침범 되는 양상을 보이며, 혈관과 신경 등이 통과하는 부분
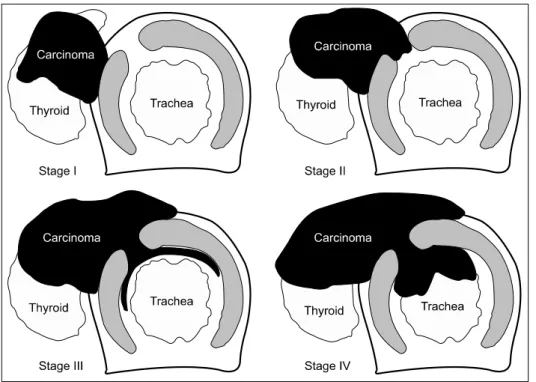
Fig. 1. The staging system for papillary carcinoma of the thyroid invading the trachea, based on the histopathologic extent of invasion. (Adapted from Shin DH, Mark EJ, Suen HC, Grillo HC. Pathologic staging of papillary carcinoma of the thyroid with airway invasion based on the ana- tomic manner of extension to the trachea: a clinicopatho- logic study based on 22 patients who underwent thy- roidectomy and airway resec- tion. Hum Pathol 1993;24(8):
866-70.) 은 약하기 때문에 이 부분을 통과하여 암 조직이 기관
강 내의 점막까지 침범하는 주요 경로가 된다고 하였 다. 그리고 1995년 Ozaki 등15)은 기관 길이방향 침범 (longitudinal spread)은 기관 외막(adventitia of trachea) 쪽의 병변이 기관 점막(tracheal mucosa) 쪽의 병변보다 광범위하며, 기관 둘레방향 침범(circumferential spread) 은 대부분 기관 외막 쪽의 병변이 기관 점막 쪽 병변보 다 크지만 점막 쪽의 병변이 큰 경우도 있다고 하였고, 이를 근거로 둘레방향으로 전체 기관륜을 제거 (circumferential sleeve resection)하고, 단단문합술을 시 행하여야 한다고 하였다.
기관을 침범한 분화갑상선암의 수술은 육안적 종괴 를 모두 제거하는 것이지만, 다른 암에 비해 천천히 자 라고 침습적이지 않으므로 정상 구조물을 가능하면 희 생하지 않고도 치료 효과를 기대할 수 있는 범위의 절 제역을 얻는 것이 목표이다. 특히 후두 및 기관의 침범 은 국소재발, 림프절 전이 등을 증가시키고 결과적으 로 생존율에도 영향을 미치는 것으로 보고되지만 반면 에 후두 및 기관의 제거는 중요한 기능 상실로 이어진 다. 그래서 항상 절제 범위에 대한 논란이 있을 수밖에 없는데, 이는 결과에 대한 평가가 갑상선암의 특성상 장기간의 추적 관찰 후 이루어지기 때문이다. 그래서 수술 방법의 선택은 환자의 나이, 환자의 사회적 활동 성(social activity), 종양 침습의 깊이와 범위, 종양 세포 의 종류, 과거 치료법에 대한 반응 등을 고려하여 정해
진다.
상기도 침범 시 수술적 치료 방법 중 면도 절제술 (shave excision)이 안전한가, 그렇지 못한가는 저자에 따라 의견이 상이하다. 면도 절제술의 정의는 McCaffrey 등16)이 언급한 바와 같이 근육, 식도 또는 후 두, 기관의 연골막을 표재성으로 침범(superficially invaded)했을 때 절제하는 술식으로써 현미경적으로는 종양이 남아있을 가능성이 있지만 육안적으로는 종양 이 완전히 절제된 상태로 정의될 수 있다. McCaffrey 등16)은 기도 침범이 있는 경우 기도 침범이 없는 환자 에 비해 생존율이 확실히 감소하지만, 기도 침범이 있 을 때 육안적으로 완전 절제만 가능하다면 면도 절제 술을 시행한 환자군과 기도의 전층 절제를 시행한 환 자군 간에 생존율 차이가 없음을 발표했다.1,2,5,17) Cody, Segal, Lipton, Fujimoto 등도 이와 비슷한 결과를 발표
하였다.7,18-20) 반면에 면도 절제술을 반대하는 주장들로
는 Friedman, Park, Melliere, Grillo 등의 발표가 있는데, 이들은 면도 절제술을 시행한 환자군에서 재발이 많고 예후가 좋지 않음을 주장하였다.8,9,21-24)
따라서 수술 방법 선택에 대한 저자의 의견은 기관 을 침범한 암 조직을 육안적으로 완전히 절제하는 것 을 목적으로 삼아야 하며 이 과정에서 기관 연골 외막 혹은 연골 일부를 제거하여 점막이 보존된 상태라면 이는 결과적으로 면도 절제술이 되고 이것이 불가능하 면 기관 점막을 포함한 전층을 일부 혹은 둘레 전체를
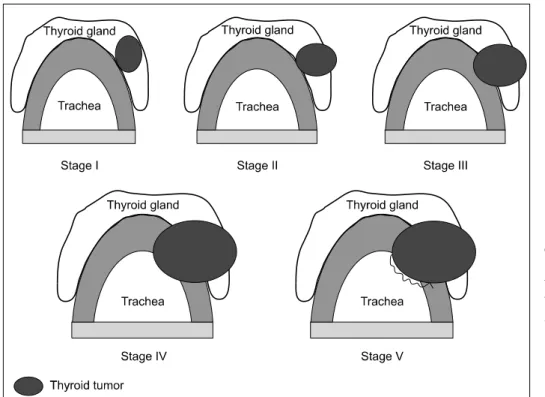
Fig. 2. Five stages of aero- digestive tract involvement by invasive well-differentiated thyroid carcinoma. (Adapted from McCaffrey JC. Aerodi- gestive tract invasion by well- differentiated thyroid carci- noma: diagnosis, manage- ment, prognosis, and biology.
Laryngoscope 2006;116(1):
1-11.) 제거하여야 한다.25-27) 그래서 처음부터 기도를 유지하
기 위해 수술을 시행하여 육안적으로 종양을 남기는 감량수술(debulking operation)이 될 수 있는 오류를 범 하지 않도록 해야 한다. 특히 기관연골 사이의 결체조 직 등에 종양이 남아 있을 가능성이 있다면 동결조직 절편검사를 시행하여 확인하여야 한다.
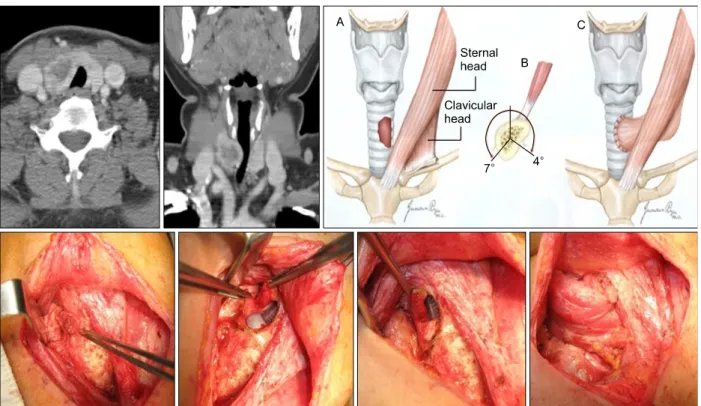
1993년 Shin 등14)은 기관침범의 양상을 분석하여 4 가지 병기분류 체계를 제시하였고, 2006년 McCaffrey 등3)은 Shin 등14)의 분류에 침범이 없는 경우를 포함하 여 5가지로 병기분류를 하고 이에 따른 적절한 수술 방법을 제안하였다(Figs. 1, 2). 기관의 연골막만 침범한 경우(stage I, II)는 면도 절제술로 충분할 것이다. 수술 은 기관을 침범한 부위를 제외하고 갑상선과 함께 종 양을 모두 박리하고 마지막으로 침범된 연골막과 아래 의 연골을 부분적으로 갑상선에 붙여서 절제한다. 그 러나 연골의 일부 혹은 전부, 점막 등의 구조물을 침범 한 경우(stage III to V)에는 완전 절제술이 필요할 것이 다. 단일 기관륜을 침범한 경우에는 window 절제술이 나 쐐기 절제술을 시행할 수 있다. Window 절제술의 경우 기관 절제가 기관연골 둘레의 30% 이내이면 전방 의 결손부위를 기관절개술로 대치하고 기관절개 튜브 를 3-5일 정도 유치한 후 발관하면 자연 치유될 수 있 으나, 30% 이상을 절제한 경우 피대근이나 흉쇄유돌근 의 회전피판을 이용하여 재건한다(Fig. 3). 기관절개술
이 필요한 환자의 경우 이를 기관절개공으로 이용할 수 있으며, 추후 기관삽관(T-cannula)을 제거한 후 닫 을 수 있다(Fig. 4).28) 쐐기 절제술(wedge resection)의 경우에는 절제술 후 흡수 봉합사를 이용하여 봉합을 시행하며, 기관과 기관점막 사이로 봉합사를 통과하여 기관 내측에는 봉합사나 knot 부위가 노출되지 않도록 주의하여야 한다.3)
한 개 이상의 기관륜을 침범한 경우에는 sleeve 절제 술 같은 더 큰 범위의 술식이 필요하다. 절제술을 시행 하기 전에 갑상선과 경부 절제술을 모두 시행한 후에 가장 마지막에 시행하도록 한다. 3 cm 미만의 작은 분 절은 바로 단단문합술을 시행할 수 있으나 3-4 cm 이 상의 분절은 기관 또는 후두의 기동화 이후에 문합하 여야 한다. Suprahyoid release는 geniohyoid, mylohyoid, hyoglossus muscles를 설골에서 박리하는 술식으로 외 측의 설동맥과 설하신경을 손상하지 않도록 주의한다.
추가로 흉곽(hilum) 쪽도 박리하면 추가적인 가동적인 기관을 얻을 수 있는데 외측의 내흉동맥(internal thoracic artery)이나 기관동맥(bronchial artery)을 손상 하지 않도록 주의하여야 한다. 만약 윤상연골이나 후 두의 일부가 같이 절제된 경우라면 아래쪽 기관을 같 은 모양으로 디자인하여 절제한 후 문합하는 방법도 고려할 수 있다. 봉합이 완료되면 봉합부위에 생리식 염수를 부은 후 기관삽관의 공기를 빼고 valsava법 혹
Fig. 4. Trough method and tracheotomy.
Fig. 3. Tracheal window resection and sternocleidomastoid myoperiosteal flap.
Fig. 5. Mechanisms of local invasion of thyroid cancer. (A) Two examples of laryngeal invasion by a thyroid tumor. Direct invasion of the thyroid cartilage is shown on the left. Invasion of the paraglottic space by a thyroid tumor wrapping around the posterior edge of the thyroid cartilage is shown on the right and in the cross-sectional insert. (B) Example of a large thyroid carcinoma invading the pyriform sinus and pharynx by posterior extension around the thyroid cartilage as well as through the substance of the thyroid cartilage. (C) Invasion of the recurrent laryngeal nerve, tracheal wall, and esophagus by extension of thyroid carcinoma from a paratracheal lymph node. (D) Limited anterior tracheal invasion by thyroid carcinoma. Insert on right shows resection with a tracheal window; a "shave" excision in this case would leave behind intraluminal tumor. (Adapted from McCaffrey TV, Bergstralh EJ, Hay ID. Locally invasive papillary thyroid carcinoma: 1940-1990. Head Neck 1994;16(2):165-72.) 은 양압 환기를 시켜 공기가 새어 나오는지 여부를 확
인하여야 한다. 공기가 새어 나오지 않으면 피대근을 원래 위치로 환원시키고, 음압배출관(suction drain)을 유치한 후 chin to chest 봉합을 시행하여 목이 굴곡된 상태를 유지하도록 한다. 기관삽관은 최소한 1일 이상 을 유지하여야 하고 기관절개술은 되도록 시행하지 않 도록 한다. Chin to chest 봉합은 2-3주 후에 제거하도 록 한다.2,29)
2) 후두
갑상선암에 의한 후두 침범은 갑상선 외 침범을 보이 는 환자의 약 1/3에서 나타나며, 애성, 천명, 객혈 등의 증상을 동반할 수 있다. 후두 침범은 3가지 경로로 발생 하는데 앞쪽으로 윤상갑상막 혹은 윤상연골을 통하여 진행하는 경로로 내강 내로 진행하여 후두의 전연 혹은 성문하 종양으로 발현된다. 두 번째 경로는 외측으로
갑상연골판을 통해 진행하는 경로로 성대마비, 점막하 종양 또는 일측 후두 내측의 궤양으로 발현된다. 세 번 째 경로는 갑상연골의 후연으로 돌아 후두주위 공간과 이상와를 통하여 진행하는 경로이다(Fig. 5).1,10)
후두를 침범한 갑상선암의 주된 치료방법은 면도 절 제술, 갑상연골 절제술(excision of the framework, thyroid cartilage), 후두 부분절제술(partial laryngectomy) 과 전후두 절제술(total laryngectomy)이다. 먼저 면도 절 제술은 제한된 적응증에서만 시행하여야 한다. 침윤이 연골막에 국한되고 연골침범이 없는 분화된 암에서만 시행되어야 하고, 갑상선의 다른 부분의 박리를 먼저 시행한 후 실시하여야 한다. 일단 갑상선이 박리되면 외측 연골막과 외측 갑상연골의 일부를 같이 제거한다. 연골 안으로의 육안적 종양 침윤이 발견되면 갑상연골 의 전층을 제거하여야 한다. 수술 전 영상 검사나 수술 중에 부성문 공간(paraglottic space)으로의 침윤이 발견
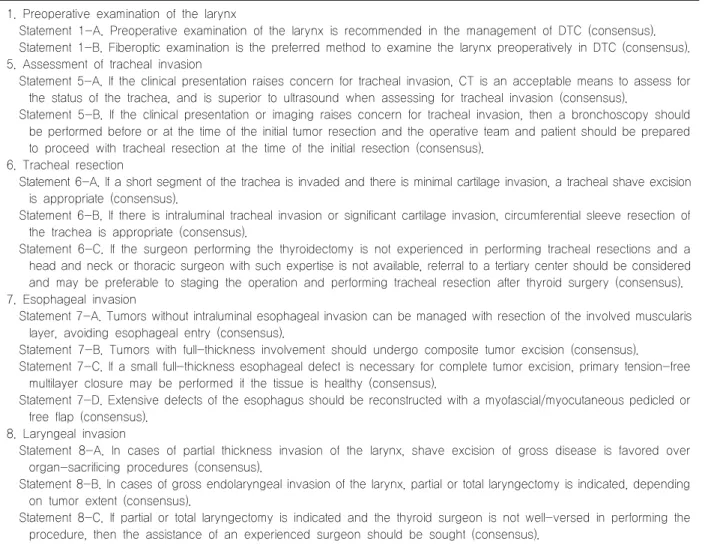
Table 2. Management of invasive well-differentiated thyroid cancer: an American Head and Neck Society consensus statement.
AHNS consensus statement
1. Preoperative examination of the larynx
Statement 1-A. Preoperative examination of the larynx is recommended in the management of DTC (consensus).
Statement 1-B. Fiberoptic examination is the preferred method to examine the larynx preoperatively in DTC (consensus).
5. Assessment of tracheal invasion
Statement 5-A. If the clinical presentation raises concern for tracheal invasion, CT is an acceptable means to assess for the status of the trachea, and is superior to ultrasound when assessing for tracheal invasion (consensus).
Statement 5-B. If the clinical presentation or imaging raises concern for tracheal invasion, then a bronchoscopy should be performed before or at the time of the initial tumor resection and the operative team and patient should be prepared to proceed with tracheal resection at the time of the initial resection (consensus).
6. Tracheal resection
Statement 6-A. If a short segment of the trachea is invaded and there is minimal cartilage invasion, a tracheal shave excision is appropriate (consensus).
Statement 6-B. If there is intraluminal tracheal invasion or significant cartilage invasion, circumferential sleeve resection of the trachea is appropriate (consensus).
Statement 6-C. If the surgeon performing the thyroidectomy is not experienced in performing tracheal resections and a head and neck or thoracic surgeon with such expertise is not available, referral to a tertiary center should be considered and may be preferable to staging the operation and performing tracheal resection after thyroid surgery (consensus).
7. Esophageal invasion
Statement 7-A. Tumors without intraluminal esophageal invasion can be managed with resection of the involved muscularis layer, avoiding esophageal entry (consensus).
Statement 7-B. Tumors with full-thickness involvement should undergo composite tumor excision (consensus).
Statement 7-C. If a small full-thickness esophageal defect is necessary for complete tumor excision, primary tension-free multilayer closure may be performed if the tissue is healthy (consensus).
Statement 7-D. Extensive defects of the esophagus should be reconstructed with a myofascial/myocutaneous pedicled or free flap (consensus).
8. Laryngeal invasion
Statement 8-A. In cases of partial thickness invasion of the larynx, shave excision of gross disease is favored over organ-sacrificing procedures (consensus).
Statement 8-B. In cases of gross endolaryngeal invasion of the larynx, partial or total laryngectomy is indicated, depending on tumor extent (consensus).
Statement 8-C. If partial or total laryngectomy is indicated and the thyroid surgeon is not well-versed in performing the procedure, then the assistance of an experienced surgeon should be sought (consensus).
되면 부분 혹은 전후두 절제술의 적응증이 된다.
갑상선암의 후두 침윤은 대부분 외측에서 발생하기 때문에 대부분은 수직후두 부분절제술(vertical hemila- ryngectomy)로 치료할 수 있다. 부분 후두 절제술은 후 두골격과 윤상연골의 50% 미만을 침범했을 때 시행할 수 있다. 하지만 광범위한 인두침윤, 반대 측 반회후두 신경마비, 후두골격과 윤상연골의 50% 이상 침윤, 내 강 내 출혈 등이 있는 경우에는 전후두 절제술의 적응 증이 된다. 더욱 광범위한 인두와 식도의 근육층을 침 윤한 경우 인두후두 전절제술(total pharyngolarynge- comy)이 필요할 수 있다.2,9,10,30)
수직후두 부분절제술(vertical hemilaryngectomy)은 후두 부분절제술이 적응되는 환자에서 가장 시행하기 좋은 술식으로 수술 과정은 다음과 같다. 갑상선의 다 른 부분을 먼저 박리한 후 후두 침윤부위의 갑상연골 외측 연골막을 절개하고 박리한다. 갑상연골을 내측으 로 견인하여 침윤 측 후방판(lamina)을 노출시키고 내
측 연골막과 후두근육을 박리하고, 내측의 이상와도 같이 박리한다. 전교련(anterior commissure)을 보존하 기 위하여 갑상연골의 중앙부는 보존하면서 약간 외측 으로 절개를 시행한다. 후두 절제를 시행할 때 종양을 건드리지 않도록 주의하여야 하며, 반대 측 정상 성대 를 손상하지 않도록 주의하여야 한다. 윤상연골은 대 부분에서 보존할 수 있어 수술 후 구축이나 흡인 등을 예방할 수 있다. 윤상연골로의 침윤이 발견된다면 하 방으로 윤상연골의 일부를 같이 절제할 수 있다.10)
술 후 재건을 시행할 때에는 대부분의 경우 종양침윤 으로 인하여 피대근이 제거된 경우가 많으므로 다른 재 건법을 고려하여야 한다. 흉쇄유돌근을 이용하는 방법 도 좋은 선택이 될 수 있는데 혈액 공급이 충분치 못하 므로 주의하여야 한다. 국소피부피판, 근막근피판, 유리 피판 등을 이용하여 재건할 수도 있다. 가장 중요한 원 칙은 건강하고 혈액 공급이 충분한 근육이나 근막으로 재건하도록 하여 창상 열개나 누공의 발생을 막고, 음
Fig. 6. Surgical algorithm for management of invasive well- differentiated thyroid carci- noma. (Adapted from McCaffrey JC. Aerodigestive tract in- vasion by well-differentiated thyroid carcinoma: diagnosis, management, prognosis, and biology. Laryngoscope 2006;
116(1):1-11.) 성과 연하작용이 원활하게 일어나도록 하여야 한다.
3) 하인두와 식도
연하곤란은 갑상선암 환자에서 드물지 않은 증상이 지만 실제로 상부소화기계의 침범은 드물다. Cody 등7) 은 3.1%의 식도 침범을 보고하였고, 대부분 하인두나 식도의 침범이 있는 환자는 후두나 기관의 침범이 있 는 환자였다. 다른 보고자들도 호흡기관의 침범보다 적은 것으로 보고하고 있다.1,31)
술 전 식도 내시경으로 내강 내 침윤 여부를 잘 관찰 할 수 있다. 식도 점막은 악성 종양의 침윤에 상대적으 로 저항성이 있어 대부분은 근육층에 국한되어 있기 때문에 점막으로부터 종양을 제거하기가 비교적 쉬운 편이다. 대부분의 환자에서는 외부 근육층까지만 침범 이 있고, 식도강 내의 직접적인 침범은 거의 없는 것으 로 보고되고 있으며, 점막을 보존하고 근육층을 절제 하면 된다고 하였다.10,20,32,33) 하지만 양측 모두 침범이 있거나 식도강 내 침범이 있으면 complete circumfe- rential esophagectomy가 요구되며, 이의 재건에는 근피 판, 전박유리피판,20) 유리공장이식,5) 인두위문합술 (Gastric pull-up)5,34)이 이용되었다. 인두 부분절제술 또 는 이상와 절제술 시에는 보통 후두 전절제술, 후두 부 분절제술 등이 요구되며, 적어도 동측의 갑상연골의 일부는 절제되어야 하고, 점막 내부의 침범이 있거나 후윤상부 침범이 있으면 후두인두 전절제술이 요구되 며 이의 재건에는 인두위문합술(gastric pull-up)이 유용하 다.
종양 주변을 박리하여 종양을 견인하면 쉽게 식도와 전척추 근막(prevertebral fascia) 사이의 층을 확인할 수 있고 같은 방법으로 반회후두신경을 보존하며 기관과 식도 사이의 층도 확인할 수 있다. 종양을 완전히 일괴 (en bloc)로 절제할 수 있는 정도까지 박리하여야 하며 식도는 기관과 반대로 하방에서 상방으로 박리를 시작 하여야 한다. 수술 전 식도침범이 의심되면 비위관 (nasogastric feeding tube)을 삽입하여 수술 중 식도의 인식에 도움을 받을 수 있도록 한다.10) 드물지만 여러 가지 원인으로 인해 수술이 불가능한 환자에서 증상 완화 목적으로 식도 스텐트를 시행할 수 있다.35) AHNS Consensus Statement
2014년 미국두경부외과학회 회원들 중에서 갑상선 수술의 권위자들이 모여 이러한 침습적 분화갑상선암 의 치료에 대한 토론을 통해 진료지침보다는 한 단계 아래인 합의성명서(Consensus Statement)를 발표하였 다. 이는 아직도 논란이 있음을 반영하는 결과라고 할 수 있다. 그러므로 실제 환자에서 기관, 후두, 식도의 상태를 면밀히 파악하여 각각의 환자의 상태에 따른 치료 계획을 수립하는 것이 중요하다(Table 2).36)
결 론
국소 진행성 갑상선암에서 갑상선 주위로 침범이 발 생하면 국소 재발의 위험이 증가하고, 후두 및 기관의 침범은 생존율에도 영향을 미칠 수 있다. 아직까지 국
소 진행성 갑상선암의 주 치료는 수술이며, 암 조직의 완전절제와 주변 중요한 구조물을 보존하여 기능을 유 지할 수 있는 수술 접근이 이루어져야 한다.
수술 중 중요한 구조물을 보존하기 위하여 절제의 범위를 줄이고자 하는 생각을 하게 될 수 있지만, 항상 명심하여야 할 것은 육안적인 잔존 종양을 남기게 될 경우 추후 재수술은 훨씬 어려울 수 있고, 외부 방사선 조사나 방사성 동위원소 치료가 불충분한 수술을 보완 해주지 못한다는 사실이다.
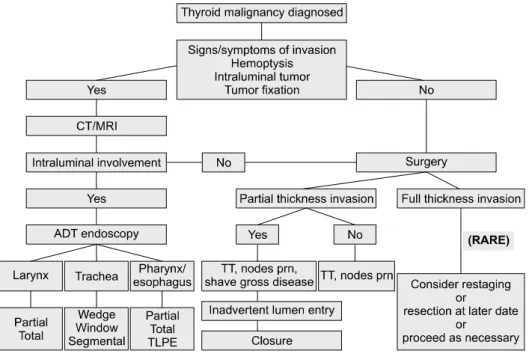
적절한 수술방법의 선택은 환자에게 완치의 기회, 국소제어율, 의미 있는 생존 연장의 기회를 제공할 수 있다. 수술법을 선택할 때에는 완전절제와 수술 후 환 자의 기능적인 측면을 모두 고려하고 환자의 나이, 사 회적 활동, 종양의 침범 정도, 조직학적 아형, 원격전이 의 유무, 과거력, 보조치료, 술자의 술기 등을 종합적으 로 고려하여 수술 범위를 결정하여야 한다(Fig. 6).3) 중심 단어: 국소 진행성 갑상선암, 후두, 기관, 식도.
References
1) McCaffrey TV, Bergstralh EJ, Hay ID. Locally invasive papillary thyroid carcinoma: 1940-1990. Head Neck 1994;16(2):
165-72.
2) Czaja JM, McCaffrey TV. The surgical management of laryngotracheal invasion by well-differentiated papillary thyroid carcinoma. Arch Otolaryngol Head Neck Surg 1997;123(5):484-90.
3) McCaffrey JC. Aerodigestive tract invasion by well-differentiated thyroid carcinoma: diagnosis, management, prognosis, and biology. Laryngoscope 2006;116(1):1-11.
4) Lawson W, Som HL, Biller HF. Papillary adenocarcinoma of the thyroid invading the upper air passages. Ann Otol Rhinol Laryngol 1977;86(6 Pt 1):751-5.
5) McCaffrey TV, Lipton RJ. Thyroid carcinoma invading the upper aerodigestive system. Laryngoscope 1990;100(8):824-30.
6) Breaux GP Jr, Guillamondegui OM. Treatment of locally invasive carcinoma of the thyroid: how radical? Am J Surg 1980;140(4):514-7.
7) Cody HS 3rd, Shah JP. Locally invasive, well-differentiated thyroid cancer. 22 years' experience at Memorial Sloan-Kettering Cancer Center. Am J Surg 1981;142(4):480-3.
8) Grillo HC, Zannini P. Resectional management of airway invasion by thyroid carcinoma. Ann Thorac Surg 1986;42(3):
287-98.
9) Friedman M, Danielzadeh JA, Caldarelli DD. Treatment of patients with carcinoma of the thyroid invading the airway. Arch Otolaryngol Head Neck Surg 1994;120(12):1377-81.
10) Price DL, Wong RJ, Randolph GW. Invasive thyroid cancer:
management of the trachea and esophagus. Otolaryngol Clin North Am 2008;41(6):1155-68, ix-x.
11) Andersen PE, Kinsella J, Loree TR, Shaha AR, Shah JP.
Differentiated carcinoma of the thyroid with extrathyroidal extension. Am J Surg 1995;170(5):467-70.
12) Hay ID, McConahey WM, Goellner JR. Managing patients with papillary thyroid carcinoma: insights gained from the Mayo Clinic's experience of treating 2,512 consecutive patients during 1940 through 2000. Trans Am Clin Climatol Assoc 2002;
113:241-60.
13) Machens A, Hinze R, Lautenschlager C, Thomusch O, Dralle H. Thyroid carcinoma invading the cervicovisceral axis: routes of invasion and clinical implications. Surgery 2001;129(1):23-8.
14) Shin DH, Mark EJ, Suen HC, Grillo HC. Pathologic staging of papillary carcinoma of the thyroid with airway invasion based on the anatomic manner of extension to the trachea: a clinicopathologic study based on 22 patients who underwent thyroidectomy and airway resection. Hum Pathol 1993;24(8):
866-70.
15) Ozaki O, Sugino K, Mimura T, Ito K. Surgery for patients with thyroid carcinoma invading the trachea: circumferential sleeve resection followed by end-to-end anastomosis. Surgery 1995;117(3):268-71.
16) McCaffrey JC. Evaluation and treatment of aerodigestive tract invasion by well-differentiated thyroid carcinoma. Cancer Control 2000;7(3):246-52.
17) Segal K, Shpitzer T, Hazan A, Bachar G, Marshak G, Popovtzer A. Invasive well-differentiated thyroid carcinoma:
effect of treatment modalities on outcome. Otolaryngol Head Neck Surg 2006;134(5):819-22.
18) Segal K, Abraham A, Levy R, Schindel J. Carcinomas of the thyroid gland invading larynx and trachea. Clin Otolaryngol Allied Sci 1984;9(1):21-5.
19) Lipton RJ, McCaffrey TV, van Heerden JA. Surgical treatment of invasion of the upper aerodigestive tract by well-differentiated thyroid carcinoma. Am J Surg 1987;154(4):363-7.
20) Fujimoto Y, Obara T, Ito Y, Kodama T, Yashiro T, Yamashita T, et al. Aggressive surgical approach for locally invasive papillary carcinoma of the thyroid in patients over forty-five years of age. Surgery 1986;100(6):1098-107.
21) Friedman M. Surgical management of thyroid carcinoma with laryngotracheal invasion. Otolaryngol Clin North Am 1990;
23(3):495-507.
22) Park CS, Suh KW, Min JS. Cartilage-shaving procedure for the control of tracheal cartilage invasion by thyroid carcinoma. Head Neck 1993;15(4):289-91.
23) Melliere DJ, Ben Yahia NE, Becquemin JP, Lange F, Boulahdour H. Thyroid carcinoma with tracheal or esophageal involvement: limited or maximal surgery? Surgery 1993;113(2):
166-72.
24) Kasperbauer JL. Locally advanced thyroid carcinoma. Ann Otol Rhinol Laryngol 2004;113(9):749-53.
25) Gaissert HA, Honings J, Grillo HC, Donahue DM, Wain JC, Wright CD, et al. Segmental laryngotracheal and tracheal resection for invasive thyroid carcinoma. Ann Thorac Surg 2007;83(6):1952-9.
26) Nishida T, Nakao K, Hamaji M. Differentiated thyroid carcinoma with airway invasion: indication for tracheal resection based on the extent of cancer invasion. J Thorac Cardiovasc Surg 1997;114(1):84-92.
27) Wada N, Nakayama H, Masudo Y, Suganuma N, Rino Y.
Clinical outcome of different modes of resection in papillary thyroid carcinomas with laryngotracheal invasion. Langenbecks Arch Surg 2006;391(6):545-9.
28) Okada K, Murakami Y, Ikari T, Haraguchi S, Maruyama T, Tateno H. Surgical treatment of laryngotracheal stenosis by a trough technique. Auris Nasus Larynx 1985;12 Suppl 2:S78-80.
29) Kim KH, Sung MW, Chang KH, Kang BS. Therapeutic dilemmas in the management of thyroid cancer with laryngotracheal involvement. Otolaryngol Head Neck Surg 2000;122(5):763-7.
30) Donnelly MJ, Considine N, McShane DP. Upper airway invasion by well-differentiated thyroid carcinoma. J Laryngol Otol 1993;107(8):752-4.
31) Grillo HC, Suen HC, Mathisen DJ, Wain JC. Resectional management of thyroid carcinoma invading the airway. Ann Thorac Surg 1992;54(1):3-9; discussion 9-10.
32) Ishihara T, Kobayashi K, Kikuchi K, Kato R, Kawamura M, Ito K. Surgical treatment of advanced thyroid carcinoma invading the trachea. J Thorac Cardiovasc Surg 1991;102(5):
717-20.
33) Ballantyne AJ. Resections of the upper aerodigestive tract for locally invasive thyroid cancer. Am J Surg 1994;168(6):636-9.
34) Kato H, Iizuka T, Watanabe H, Hirata K, Ono I, Ebihara S, et al. Pull-through esophagectomy without thoracotomy. Jpn J Clin Oncol 1983;13(1):53-9.
35) Ginsberg GG. Palliation of malignant esophageal dysphagia:
would you like plastic or metal? Am J Gastroenterol 2007;
102(12):2678-9.
36) Shindo ML, Caruana SM, Kandil E, McCaffrey JC, Orloff LA, Porterfield JR, et al. Management of invasive well-differentiated thyroid cancer: an American Head and Neck Society consensus statement. AHNS consensus statement. Head Neck 2014;36(10):1379-90.