Received: June 2, 2017 / Accepted: June 7, 2017 Address for correspondence: Kee Hong Park, MD
Department of Neurology, Geongsang National University Hospital, 79 Gangnam-ro, Jinju 52727, Korea Tel: +82-55-750-9785, Fax: +82-55-755-1709, Email: [email protected]
근위부 위약
경상대학교병원 신경과
박 기 홍
Proximal Weakness
Kee Hong Park, MD
Department of Neurology, Geongsang National University Hospital, Jinju, Korea
KEYWORDS Weakness, Myopathy, Myasthenia gravis
Recognition of weakness pattern is important for localization and differential diagnosis. Typical pre- sentation of proximal weakness is difficulty in raising arm, rising from floor, or climbing stairs. Most of muscle diseases present with proximal weakness. Peripheral neuropathy, neuromuscular junc- tion disorder, or anterior horn cell disease can also manifest proximal weakness. In this article, we will review clinical presentation and differential diagnosis of proximal weakness.
서 론
위약(weakness)은 신경과에서 흔히 접하게 되는 증상이 다. 그러나 “weakness”라는 단어의 우리말 용어를 검색해 보면 의학용어위원회에서는 쇠약, 허약, 탈력감으로, 대한 신경과학회 의학용어검색에서는 쇠약, 허약, 위약과 같이 다양하게 번역이 되고 있다. 또한 실제 환자들이 호소하게 되는 증상은 ‘기운이 없다’, ‘힘이 없다’, ‘힘이 빠진다’, ‘마 비가 온다’ 등과 같이 다양하게 표현하기 때문에 이를 객관 적으로 파악하는 것이 중요하다. 위약을 호소하는 환자를 평가할 때에는 다음과 같은 순서를 따른다: (1) 환자가 호소 하는 증상이 의미하는 바를 명확히 한다, (2) 위약이 신경계 질환에 의한 것인지 확인한다, (3) 위약의 위치, 범위를 확 인한다, (4) 원인 질환을 규명한다.1 이 중 위약의 분포가 근 위부에 국한되어 있거나 근위부 위약이 더 우세할 경우 임 상적 소견 및 감별진단에 대해 논하고자 한다.
근위부 위약의 증상 및 검진 소견 1. 상지 근위부 위약
증상 초기에는 손을 머리 위로 하고 수행해야 하는 동작 들에 어려움을 겪게 된다. 이를테면 빗질이나 머리감기, 선 반 위의 물건을 옮기기, 천장의 전구 갈기와 같은 동작을 잘 하지 못하거나 쉽게 피로감을 느끼게 된다. 증상이 진행 하면 자신의 팔 무게도 감당하기 힘들어 팔을 들기가 어려 워진다. 이에 따라 팔을 들 때 몸통을 더 많이 사용하는 양 상을 취할 수 있다.
정상적으로는 어깨가 등 쪽에 고정되면서 차례 자세를 취했을 때 엄지 손가락이 앞으로 향해 있게 되나, 어깨 근 육의 긴장도가 떨어지면 어깨가 앞쪽으로 회전하게 되고 이에 따라 팔이 회전하면서 손등이 앞을 향하게 되는 자세 를 취하게 된다.
Medial winging Lateral winging
Injured nerve Long thoracic Spinal accessary Dorsal scapular
Muscle palsy Serratus anterior Trapezius Rhomboideus
Physical exam Arm flexion; push-up motion against a wall
Arm abduction; external rotation against resistance
Arm extension from full flexion
Position of the scapula compared to normal
Entire scapula displaced more medial and superior
Superior angle more laterally displaced
Inferior angle more laterally displaced
Table 1. Neurogenic causes of scapular winging and the physical exam
날개어깨뼈(winged scapula)가 관찰될 수 있다. 어깨뼈를 몸통에 고정시키는 역할을 하는 앞톱니근(serratus anterior), 등세모근(trapezius), 능형근(rhomboideus)의 위약이 있으면 날개어깨뼈(winged scapula)가 관찰될 수 있다(Table 1).2 2. 하지 근위부 위약
바닥에서 일어나거나 낮은 의자에서 일어날 때 어려움을 느끼고 손이나 무릎을 이용해야 하며, 이는 검진 시 쪼그려 앉아있다가 손을 짚고 일어나는 Gower 징후를 통해 확인할 수도 있다. 계단을 오르내리는 것도 힘들어지는데 엉덩이폄 근이 약한 경우 오르는 것이 힘들어지며, 넙다리네갈래근 (quadriceps muscle)의 위약이 심한 경우에는 계단을 내려가 는 것이 더 힘들고 무릎을 긴장시킨 채로 내려가야 한다.
평지를 걸을 때에는 딛는 다리의 반대측 엉덩이와 동측 몸 통이 무게가 쏠리는 방향으로 기울어지면서 뒤뚱뒤뚱 걷는 오리걸음(waddling gait) 양상을 보이게 된다.
3. 축근육(axial muscle) 위약
복근이 약해지면 윗몸 일으키기가 힘들어지며 척추옆근 육(paraspinal muscle) 위약 시 앉아있거나 서있을 때 곧은 자세를 유지하기가 어려워진다. 목굽힘근이 약해지면 누운 상태에서 베개에서 머리를 떼는 것이 어렵고, 목폄근이 약 해지면 머리 자세를 유지하는 것이 힘들어지면서 심해지면 목을 펴지 못하고 턱이 가슴에 붙게 되는 머리처짐증후군 (dropped head syndrome)이 관찰된다. 호흡근 약화시 호흡 곤란이 유발되나 초기에는 아침에 두통을 호소하거나 수면 장애와 같은 양상으로 나타나기도 한다.
병변위치에 따른 근위부 위약을 유발할 수 있는 감별질환들
1. 근육
근육병의 경우 양측에 대칭적으로 팔다리이음부 위약이
발생하는 것이 가장 흔한 양상이다. 그러나 원위부 위약 이 우세한 근육병들도 있다. 이 유형의 위약은 본 원고에 서는 다루지 않는다. 상지 위약은 근위부에 있으나 하지는 종아리 앞쪽 근육이 주로 침범되는 어깨뼈종아리형 분포 (scapuloperoneal distribution)로 나타나는 경우도 있으며 얼 굴어깨상완근육디스트로피, 어깨종아리근육디스트로피, Emery- Dreifuss근육디스트로피, 팔다리이음부근육디스트 로피 2A, 2C-F, 2I, 네말린근병증, 중심핵병(central core disease), 폼페병 등에서 나타난다.3 반대로 하지는 넙다리 네갈래근이 침범되나 상지는 손목과 손가락 굽힘근이 침범 되는 양상은 봉입체근염에서 특징적으로 나타나며 종종 양 측에 비대칭적이다.3 그 외 근위부 근육병들 중 특이할 만 한 질환들을 소개한다.
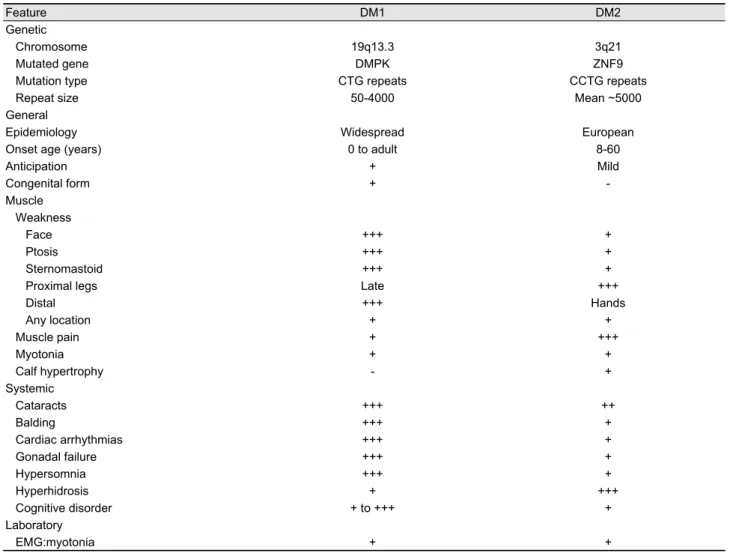
1) 근긴장디스트로피 2형(myotonic dystrophy type 2, DM2) DM2는 근긴장증(90%)과 근위약(82%)을 특징으로 하는 다계통 질환이다.4 원위부 위약이 더 심한 1형(DM1)과 달 리 DM2는 근위부 위약이 특징으로 이전에는 근위부근긴장 근병증(proximal myotonic myopathy)로 불렸었다.5 목근육, 팔꿈치폄근, 엉덩이굽힘근들이 주로 침범된다. 그 외 DM1 과 마찬가지로 백내장, 부정맥, 당뇨와 같은 다른 질환들이 동반되는 경우가 많으며, DM1과의 비교는 Table 2에 정리 하였다.4
2) 후기발병형 폼페병(Late onset Pompe disease, LOPD) 대사성 근육병은 당원 대사 이상, 지질 대사 이상, 미토 콘드리아 이상에 의해 유발되며 대부분은 고정적인 근위약 보다는 운동에 의해 증상이 유발되며 운동못견딤증, 근육 통, 근육경련 등으로 나타난다. 그러나 일부 질환은 고정적 근위약이 주된 증상으로 나타나는데 대표적인 질환이 폼페 병이다. 폼페병은 acid α-glucosidase (GAA) 결핍으로 리소 솜에 당원이 축적되어 발생하는 상염색체열성 질환으로 2 형 당원저장병(glycogen storage disease type II) 혹은 산성 말타아제결핍증(acid maltase deficiency) 등으로 불리기도 한다.6 신생아 시기에 발병하여 1세 이전에 사망하는 영아/
조기발병형과는 달리 LOPD는 1세 이후에 발생하며 노인
Feature DM1 DM2 Genetic
Chromosome 19q13.3 3q21
Mutated gene DMPK ZNF9
Mutation type CTG repeats CCTG repeats
Repeat size 50-4000 Mean ~5000
General
Epidemiology Widespread European
Onset age (years) 0 to adult 8-60
Anticipation + Mild
Congenital form + -
Muscle Weakness
Face +++ +
Ptosis +++ +
Sternomastoid +++ +
Proximal legs Late +++
Distal +++ Hands
Any location + +
Muscle pain + +++
Myotonia + +
Calf hypertrophy - +
Systemic
Cataracts +++ ++
Balding +++ +
Cardiac arrhythmias +++ +
Gonadal failure +++ +
Hypersomnia +++ +
Hyperhidrosis + +++
Cognitive disorder + to +++ +
Laboratory
EMG:myotonia + +
DM1, myotonic dystrophy type 1; DM2, myotonic dystrophy type 2; EMG, electromyography.
Table 2. Comparative features of DM1 and DM2
에서도 나타날 수 있다. 원위부보다 근위부 위약이, 견갑대 (shoulder girdle)보다 골반대(pelvic girdle) 위약이 더 심하 며 횡격막과 척추옆근육의 침범도 흔하다.7 그 외 어깨뼈종아 리형, 날개어깨뼈, 척추옆근육위축 등으로 나타나기도 한다.
2. 신경근육접합부
중증근무력증의 초기 증상으로 가장 흔한 것은 안검하수 나 복시와 같은 안구증상으로 전체의 50% 이상을 차지하 며 구음장애, 삼킴장애, 씹기장애 등의 연수마비(bulbar pal- sy)는 약 15% 정도이다. 사지마비는 근위부 위약이 더 우세 하나 사지마비만으로 발현하는 경우는 10% 미만이다. 이에 비해 근무력증후군(Lambert-Eaton myasthenic syndrome)은 안구 증상은 잘 나타나지 않고 하지 근위약이 우세하여 의 자에서 일어나거나 계단오르기가 힘들어진다.8 중증근무력
증은 근육을 사용할수록 위약이 심해지고 쉬면 호전되며, 일중변동(diurnal variation)이 특징적인 양상이나, 근무력증 후군은 근수축 동안은 일시적으로 근력이 호전되었다가 이 후 피로가 발생하는 양상이다. 두 질환의 감별점에 대해서 는 Table 3에 정리하였다.9
3. 말초신경
다발말초신경병증은 대개 원위부 증상이 더 우세하게 나 타나나 길랑바레증후군이나 만성염증탈수초다발신경병증 (chronic inflammatory demyelinating polyneuropathy)과 같 은 자가면역성 질환의 경우 근위부 위약이 동반된다.10 신 경총병증(plexopathy), 신경근병증(radiculopathy), 단신경병 증(mononeuropathy)의 경우 침범된 부위에 따라 해당 팔이 나 다리의 근위부 위약으로 나타날 수 있다.
Lambert–Eaton syndrome Myasthenia gravis Clinical onset Mild proximal leg weakness, almost all cases
Oculobulbar symptoms, only 5% of patients
Oculobulbar symptoms, 90% of patients Limb weakness uncommon, 12% of patients Pattern of spread Frequently symmetric weakness
Caudally to cranially; proximally to distally
Frequently asymmetric weakness
Craniocaudal direction; proximally to distally Oculobulbar symptoms Later and usually milder
Mild ptosis, symmetrical (more often than diplopia)
Improvement of ptosis after brief upgaze
Usual in early stages and prominent Ptosis (or diplopia) frequently severe,
asymmetrical
Ptosis (and diplopia) exacerbated by prolonged upgaze
Internal ophthalmoplegia Sluggish pupillary reflexes, 69% of patients Possible but more rarely reported
Isolated muscle weakness Rare More common
Muscle fatigability pattern Initial strength improvement during muscle contraction and then fatigue again.
Worsening with use and improving with rest Diurnal variation, worsening in the later part of
the day Clinical profile Gradual onset over months or years
More rapidly in P-LES than in NP-LES
Symptoms may fluctuate, and there may be remissions of variable length, particularly at early stages
Tendon reflexes Diminished/absent at rest, in over 90% of patients
Reappear following a brief MVC
Usually preserved, except in severe limb weakness
May be brisk in clinically weak muscles Autonomic dysfunction Characteristically affected
Parasympathetic >sympathetic dysfunction
Unrecognized feature of MG
Rare cases of coexisting subacute autonomic failure
Serology VGCCAb in 85-90% of NP-LES
VGCCAb in near 100% of P-LES VGCCAb in 5% of patients with SCLC Rare cases of positive AChRAb (low titres)
AChRAb in 85% generalized MG AChRAb in 50% ocular MG
MuSKAb in 40% of AChRAb negative MG Rare cases of positive VGCCAb
Edrophonium tests+ Possible (37%) Majority of cases (90-95%)
Electrophysiology Reduced CMAP amplitudes, decrement with LRS and increment with high-rate RNS or brief MVC
Normal CMAP amplitudes, decrement with LRS
Tumour SCLC, 50%; thymoma possible Thymoma, 10-15%; SCLC possible
Immunotherapies Steroids, immunosuppressives, plasmapheresis or intravenous gamma globulin therapy Symptomatic drugs Guanidine; 3,4-diaminopyridine,
anticholinesterases
Anticholinesterases
P-LES, paraneoplastic LES; NP-LES, non-paraneoplastic LES; MVC, maximal voluntary contraction; MG, myasthenia gravis; VGCCAb, antibodies against voltage-gated calcium channels; AChRAb, acetylcholine receptor antibodies; MuSKAb, muscle-specific kinase antibodies; LRS, low-rate stimulation; RNS, repetitive nerve stimulation; CMAP, compound muscle action potential.
Table 3. Differential diagnosis between Lambert–Eaton syndrome and myasthenia gravis
4. 전각세포(Anterior horn cell)
척수근위축증(spinal muscular atrophy)은 척수의 전각세 포나 뇌줄기핵의 변성 또는 소실로 인해 근위약을 보이는 데 대개 대칭적이며 근위부 위약으로 나타난다.11 질환의 정도는 신생아기에 호흡기능상실이 발생하는 것부터 경도 의 근위부 위약까지 다양하게 나타난다. 따라서 중한 정도, 침범부위, 유전양상 등을 토대로 1형부터 4형까지로 분류 하고 있다.
척수연수근위축증(spinobulbar muscular atrophy)은 Kennedy 병이라고도 불리며, X염색체연관열성유전을 하며 안드로 겐수용체유전자에서 polyglutamine을 표현하는 CAG삼핵 산염기서열 반복확장으로 인해 발생한다. 사지위약은 주로 근위부에 발생하며 때때로 비대칭적으로 나타난다.12 이와 함께 얼굴근육마비, 연수마비, 근다발수축(fasciculation) 등이 발생하며 불임, 고환위축과 같은 내분비계 증상도 동반 된다.
결 론
지금까지 살펴본 바와 같이 다양한 질환에서 근위부 위 약으로 나타날 수 있다. 따라서 위약의 분포 패턴을 정확하 게 파악하고, 동반된 감각 증상, 하위/상위운동신경원 징후, 발현 나이, 가족력 등을 통해 감별진단을 좁힌 후 근전도, 유전자 검사 등을 통해 이를 확인할 필요가 있다. 특히 치 료가 가능한 질환들을 빨리 감별하여 적절한 치료를 통해 환자의 삶의 질을 개선해야 할 것이다.
REFERENCES
1. Dimberg EL. The office evaluation of weakness. Semin Neurol 2011;31:115-130.
2. Martin RM, Fish DE. Scapular winging: Anatomical review, di- agnosis and treatments. Curr Rev Musculoskelet Med 2008;1:
1-11.
3. Barohn RJ, Dimachkie MM, Jackson CE. A pattern recognition approach to patients with a suspected myopathy. Neurol Clin 2014;32:569-593.
4. Turner C, Hilton-Jones D. The myotonic dystrophies: diagnosis and management. J Neurol Neurosurg Psychiatry 2010;81:358- 367.
5. Ricker K, Koch MC, Lehmann-Horn F, et al. Proximal myotonic myopathy: a new dominant disorder with myotonia, muscle weakness, and cataracts. Neurology 1994;44:1448-1452.
6. Winchester B, Bali D, Bodamer OA, et al. Methods for a prompt and reliable laboratory diagnosis of Pompe disease: Report from an international consensus meeting. Mol Genet Metab 2008;93:
275-281.
7. Al-Lozi MT, Amato AA, Barohn RJ, et al. Diagnostic criteria for late-onset (childhood and adult) Pompe disease. Muscle and Nerve 2009;40:149-160.
8. Wirtz PW, Sotodeh M, Nijnuis M, et al. Difference in dis- tribution of muscle weakness between myasthenia gravis and the Lambert–Eaton myasthenic syndrome. J Neurol Neurosurg Psychiatry 2002;73:766-768.
9. Merino-Ramírez MÁ, Bolton CF. Review of the diagnostic chal- lenges of Lambert–Eaton syndrome revealed through Three case reports. Can J Neurol Sci 2016;43:635-647.
10. Köller H, Kieseier BC, Jander S, Hartung HP. Chronic in- flammatory demyelinating polyneuropathy. New England J Med 2005;352: 1343-1356.
11. Arnold WD, Kassar D, Kissel JT. Spinal muscular atrophy: diag- nosis and management in a new therapeutic era. Muscle Nerve 2015;51:157-167.
12. Katsuno M, Tanaka F, Adachi H, et al. Pathogenesis and therapy of spinal and bulbar muscular atrophy (SBMA). Prog NeurobiolZ 2012;99:246-256.