생식세포종(germ cell tumor)은 소아에서 흔하지 않은 질병으로, 전체 소아 종양의 1%를 차지하는 드문 질환이며, 기형종(teratoma)이 가장 흔한 조 직형으로 성숙 기형종과 미성숙 기형종이 여기에 속한다. 치료는 조직형, 위치, 나이 병기에 따라 다르며, 주로 수술요법과 수술 후 보조적 항암화 학요법이 시행되고, 과거에 비해 항암제와 지지요 법의 발달로 생존율이 향상되고 있다1).
대부분의 악성종양에서 치료 중 또는 치료 종료 후에 병변의 크기가 증가하거나 새로운 병변이
발견되면 재발과의 감별이 중요하며 예후에 큰 영향을 줄 수 있다.
그러나, 생식세포종은 예외적으로 항암치료에 효과적으로 반응하고 종양표지자가 정상이 되었 음에도 불구하고 종양의 크기가 증가하는 경우가 있다. 이를 성장 기형종 증후군(growing teratoma syndrome)이라고 한다2). 병리조직소견은 주로 성 숙 기형종으로서 치료는 종양의 수술적 제거이고, 예후는 좋은 것으로 알려져 있다.
저자들은 난소에서 발생한 미성숙 기형종을 수 술로 적출한 후 항암화학요법 중 흉부와 복부에 발생한 재발성의 성장 기형종을 경험하여 문헌고 찰과 함께 보고하는 바이다.
재발성 성장 기형종 증후군 1례
충북대학교 의과대학 소아과학교실, 1병리학교실, 2국립암센터 소아종양클리닉
최종성 임영수 이옥준1 박현진2 김지윤
A Case of Recurrent Growing Teratoma Syndrome during Chemotherapy for Immature Teratoma of the Ovary
Jong Sung Choi, M.D., Young Su Lim, M.D., Ok-Jun Lee, M.D.
1,Hyeon Jin Park, M.D.
2 and Ji Yoon Kim, M.D.Departments of Pediatrics and 1Pathology, Chungbuk National University College of Medicine, Cheongju, 2Pediatric Oncology Branch, National Cancer Center, Goyang, Korea Enlarging masses during or after chemotherapy of malignancy is thought to be the evidence of malignancy recurrence. However, growing teratoma syndrome is defined as enlarging masses of benign mature teratoma following chemotherapy for malignant germ cell tumors. Typically, the histology shows a mature teratoma without any malignant element and it is associated normalization of initially elevated serum tumor markers. We present a case of recurrent growing teratoma syndrome originating from an immature teratoma of the ovary during chemotherapy in a 10-year-old girl.
(Clin Pediatr Hematol Oncol 2007;14:93∼97)
Key Words: Growing teratoma syndrome, Immature teratoma, Chemotherapy
책임저자 김지윤, 충북 청주시 흥덕구 개신동 12번지 충북대학교 의과대학 소아과학교실, 361-763 Tel: 043-269-6043, Fax: 043-264-6620 E-mail: [email protected]
임상소아혈액종양
제 14 권 제 1 호 2007 93
증 례
환 아: 이○○, 10세, 여아
주 소: 내원 10일 전부터 발생한 복통과 복부 팽만
과거력 및 현병력: 평소 건강하게 지내던 중 내 원 10일 전부터 복통과 복부팽만이 발생하였고, 내원 당일 개인병원에서 진찰 및 복부 초음파를 시행한 결과 복부 종양이 의심되어 본원으로 전 원 되었다.
진찰소견: 내원 당시 혈압은 120/90 mmHg, 맥박 수는 70회/분, 호흡수는 22회/분, 체온은 36.5oC였 다. 환아는 아파보이지 않았고 의식은 명료하였 다. 공막과 결막은 특이 소견이 없었고 구강 내 병변은 없었다. 편도비대나 인후발적은 관찰되지 않았고, 촉지되는 경부의 림프절은 없었다. 흉곽 의 이상은 관찰되지 않았고, 호흡음은 깨끗하였 다. 심박동은 규칙적이었으며 심잡음은 없었다.
복부는 팽만되어 보였으며, 배꼽의 우하방에서 직 경 10 cm의 단단한 종괴가 촉지되었다. 장음은 정 상적으로 들렸으며, 복부의 압통 및 반발통은 없 었다. 간과 비장은 만져지지 않았다.
검사소견: 일반 혈액 검사에서 혈색소는 12
g/dL, 백혈구는 10,390/μL, 혈소판 수는 324,000/
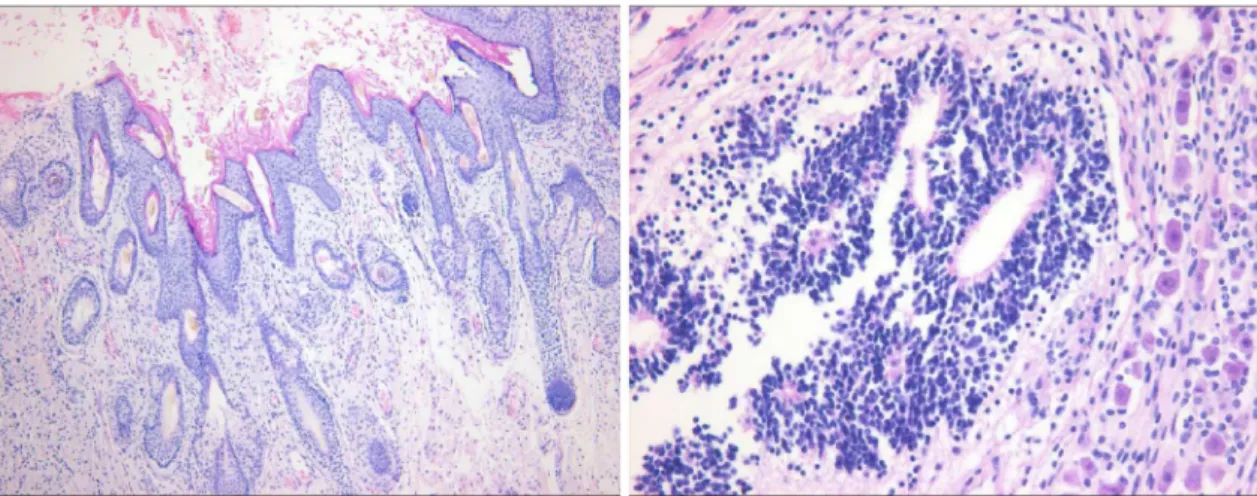
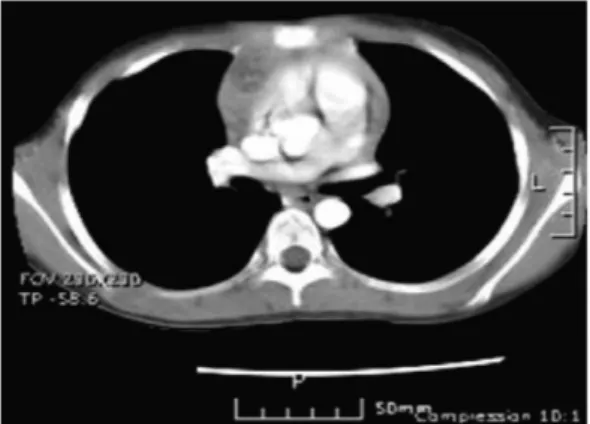
μL이었다. 말초혈액도말 검사결과는 특이소견 없었다. 종양 표지자 수치는 AFP 307 ng/mL, beta-HCG 1.2 mIU/mL, LDH 506 U/L였다. 복부 전산화 단층 촬영에서 우측 난소에 지방과 석회 화 및 낭형성을 동반한 직경 15×15 cm의 종양이 보였고(Fig. 1), 수술을 시행하여 병변을 완전히 절제하였으며, 조직검사 결과 우측 난소의 미성숙 기형종으로 진단되었다(Fig. 2).
Fig. 2. Microscopic findings of the tumor resected by first operation revealed both of mature elements such as hair follicles, sebaceous gland and skin epithelium structures (left, H&E stain, ×100), and immature elements such as primitive neuroepithelial rosettes (right, H&E stain, ×400).
Fig. 1. Preoperative pelvic CT showed the mass occu- pying the right pelvic cavity, with fat, calcifica- tion and cystic portion.
치료 및 경과: 환아는 진단 당시에 흉부 전산화 단층 촬영에서 우측 횡격막 상방의 전측 흉벽에 1 cm의 전이성 종양으로 생각되는 병변이 보였으 나, 수술 및 조직검사가 불가능할 것으로 판단되 어 CCG 8891 (Cisplatin, Etoposide, Bleomycin)에 의한 항암치료 후 반응을 관찰하기로 하였다. 항 암 유지요법(Adriamycin, Vinblastine) 중 종양표지 자는 AFP 2.2 ng/mL, beta-HCG 2.8 mIU/mL로 정 상범위였으나, 복부와 흉부의 전산화 단층 촬영에
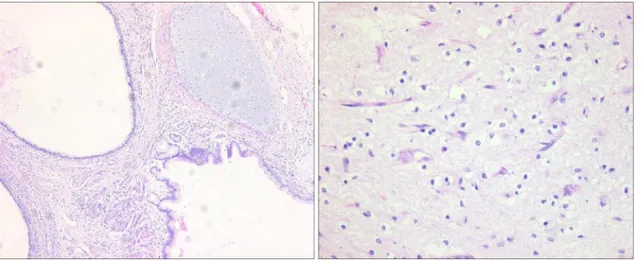
서 우측 횡격막 하방에 2×3×0.8 cm의 새로운 병 변이 발견되었고(Fig. 3), 기존의 전측 흉벽의 병 변이 2×2 cm로 크기가 증가하여 종양의 재발을 의심하였고, 항암요법은 중단하였다. 이차 수술을 시행하여 전측 흉벽과 횡격막 하방의 병변을 절 제하였고, 조직검사 결과는 모두 성숙 기형종의 소견을 보였다(Fig. 4). 이차 수술 후 6개월째 시행 한 흉부 전산화 촬영에서 우측 전 종격에 직경 3×
2 cm 정도의 새로운 병변이 발견되어 삼차 수술 을 시행하였으며(Fig. 5), 조직검사 결과 성숙 기 형종으로 진단되었다. 이후 추적관찰 소견은 현재 항암치료 후 2년 4개월째 및 삼차 수술 후 1년 10 개월째로, 종양표지자 수치는 정상범위를 유지하 고 있으며(Fig. 6), 복부 및 흉부 전산화 촬영에서 더 이상 새로운 병변은 발견되지 않고 있다.
고 찰
성장 기형종 증후군은 생식세포종 환자의 약 1.9∼7.6%에서 발생하는 비교적 드문 증후군으로2∼5), 1981년 Carr 등6)과 1982년 Logothesis 등2)이 보고 하면서 알려지게 되었으며, “chemotherapeutic retro- conversion”, “transformation”, “in-vivo maturation”,
“in-situ destruction” 등의 표현으로 다른 문헌에 기
Fig. 4. Microscopic findings of the tumor resected by second operation revealed only mature elements such as mature cartilage, respiratory (left, H&E stain, ×100), and brain tissue (right, H&E stain, ×400).
Fig. 3. Follow up abdominal CT during chemotherapy (maintenance course) showed the new mass enlarged in the right subphrenic area (yellow circle).
술되기도 하였다7∼9).
이는 항암화학요법 중 혹은 치료종료 후에 종 양의 크기가 증가하거나 새로운 병변이 발생하는 것으로, 이때 종양표지자의 수치는 정상범위 내에 있으며, 병리조직학적으로 악성 요소가 없이 잘 분화된 성숙 기형종의 특징을 나타낼 때 진단할
수 있다2,10). 본 증례의 환아에서는 항암치료 유지
요법 중과 치료 중단 후 4개월째에 각각 전산화 단층 촬영 추적관찰 과정에서 두 차례 종양이 발 견되어 재수술을 반복 시행한 경우로, 재수술 시
제거한 종양들은 병리학적 검사상 모두 성숙 기 형종으로 판명되었다.
성장 기형종 증후군의 원인에 대해서는 정확히 보고되고 있지는 않으나, 현재까지 두 가지 가설 이 제기되고 있다. 첫째 가설은 항암제에 의해 악 성세포가 제거된 후에 남아 있는 양성세포의 성 장에 기인한다는 것이며, 미성숙 기형종에 대한 항암제 투약을 종료한 후 1년 이내에 성숙 기형 종이 발생하는 경우가 이에 해당한다3,11). 두 번째 가설은 투여된 항암제에 의해 악성세포의 분화가 유도되어 성숙한 세포로 변화했다는 설이 제기되 고 있다3).
성장 기형종 증후군이 의심되면, 가능한 종양을 수술적으로 완전 제거를 하고, 반드시 병리조직형 을 확인하여야 한다. 이는 대부분이 성숙 기형종 으로 밝혀지지만, 약 3%에서는 종양의 악성 재발 이 보고되고 있기 때문이다3,12). 종양이 주위 조직 혹은 혈관에 유착되어 있는 경우에는 수술적 완 전 절제가 어려운 경우가 많고, 본 증례의 환아처 럼 종양은 반복적으로 발생이 가능하여 재수술이 필요한 경우도 있다3,12).
결론적으로 미성숙 기형종 환자의 치료 후에 성장 기형종 증후군의 발생 가능성을 염두에 두 고, 주기적으로 전산화 단층 촬영과 종양 표지자 를 추적 관찰하고 병의 재발과 정확히 감별하는 것이 중요하다고 사료된다.
참 고 문 헌
1. Cushing B, Perlman EJ, Marina NM, Castleberry RP. Germ cell tumors. In: Pizzo PA, Poplack DG, editors. Principles and practice of pediatric oncology.
5th ed. Philadelphia. Lippincott Williams & Wilkins, 2006:1116-38
2. Logothetis CJ, Samuels ML, Trindade A, Johnson DE. The growing teratoma syndrome. Cancer 1982;
50:1629-35
3. Andre F, Fizazi K, Culine S, Droz J, Taupin P, Lhomme C, et al. The growing teratoma syndrome:
Results of therapy and long-term follow-up of 33 patients. Eur J Cancer 2000;36:1389-94
4. Maroto P, Tabernero JM, Villavicencio H, Mesia R, Fig. 5. Follow up chest CT at 6 months later after
second operation showed the new mass enlarged in the right mediastinal area.
Fig. 6. Serum AFP (alpha-fetoprotein) changed after the initial operation and chemotherapy and remains normal through after the primary treatment.
Marcuello E, Sole-Balcells FJ, et al. Growing tera- toma syndrome: Experience of a single institution.
Eur Urol 1997;32:305-9
5. Jeffery GM, Theaker JM, Lee AH, Blaquiere RM, Smart CJ, Mead GM. The growing teratoma synd- rome. Br J Urol 1991;67:195-202
6. Carr BI, Gilchrist KW, Carbone PP. The variable transformation in metastases from testicular germ cell tumors: The need for selective biopsy. J Urol 1981;126:52-4
7. DiSaia PJ, Saltz A, Kagan AR, Morrow CP. Chemo- therapeutic retroconversion of immature teratoma of the ovary. Obstet Gynecol 1977;49:346-50
8. Aronowitz J, Estrada R, Lynch R, Kaplan AL.
Retroconversion of malignant immature teratomas of the ovary after chemotherapy. Gynecol Oncol 1983;
16:414-21
9. Lentini JF, Love MB, Ritchie WG, Sedlacek TV.
Computed tomography in retroconversion of hepatic metastases from immature ovarian teratoma. J Comput Assist Tomogr 1986;10:1060-2
10. Afifi HY, Bosl GJ, Burt ME. Mediastinal growing teratoma syndrome. Ann Thorac Surg 1997;64:359- 62
11. Caldas C, Sitzmann J, Trimble CL, McGuire WP 3rd. Synchronous mature teratomas of the ovary and liver: A case presenting 11 years following chemo- therapy for immature teratoma. Gynecol Oncol 1992;
47:385-90
12. Gelderman WA, Scraffordt Koops H, Sleijfer DT, Oosterhuis JW, Oldhoff J. Late recurrence of mature teratoma in nonseminomatous testicular tumors after PVB chemotherapy and surgery. Urology 1989;33:
10-4