투고일: 2010년 12월 15일, 심사일: 2010년 12월 20일, 게재확정일: 2011년 1월 3일 책임저자:최승호, 서울시 송파구 풍납2동 388-1
(138-736) 울산대학교 의과대학 서울아산병원 이비인후과학교실 Tel: 02) 3010-3710, Fax: 02) 489-2773
E-mail: shchoi@amc.seoul.kr
Copyrights ⓒ The Korean Dysphagia Society, 2011.
연하장애의 수술적 치료
한명월ㆍ최승호
울산대학교 의과대학 서울아산병원 이비인후과학교실
Surgical Management of Dysphagia
Myung Woul Han, M.D., Seung-Ho Choi, M.D.
Department of Otolaryngology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Dysphagia, or difficulty swallowing, occurs commonly, especially in elderly and debilitated patients. Dysphagia en- compasses a wide range of etiologies. Its proper evaluation and treatment uses tools and expertise from a variety of specialties working toward the common goals of safety and satisfactory quality of life. The head and neck sur- geon can be an important member of the dysphagia rehabilitation team. Most causes of dysphagia do not require surgical intervention to accomplish these goals; however, several entities warrant surgery to treat a specific problem or to augment medical/therapeutic management. The role of surgery in the management of dysphagia is clear in some areas and controversial in others. Evaluation for the causes of dysphagia elucidates conditions that have been shown to benefit from surgery for safety, for improved quality of life, or both. Surgical therapy, when indicated, is safe and effective for many causes of dysphagia. (JKDS 2010;1:39-46)
Keywords: Dyshagia, Surgery
서론
연하는 상부 소화호흡기를 지배하는 여러 신경과 근육 들의 조화로운 조절에 의해 음식물을 하부 호흡기를 보호 하며 구강으로부터 인두를 거쳐 식도로 진행시키는 일련 의 생리적 과정으로 제5, 7, 9, 10, 12번 뇌신경이 관여한 다. 이러한 연하기능에 장애가 발생하는 경우 정상 음식 물 섭취가 불가능할 뿐 아니라 하부호흡기에 흡인을 초래 하여 폐렴 등의 합병증으로 위험에 빠질 수 있다. 이러한 연하장애의 원인은 매우 다양하며 치료의 목적은 삶의 질 의 향상과 안전이 될 것이다1-3. 연하장애는 노인과 쇠약
한(debilitated) 환자에서 대부분 발생하고, 또한 두경부 암환자에서 치료 후 발생하는 후유증의 흔한 증상이다2,3. 대부분의 연하장애는 수술적 치료를 필요로 하지는 않지 만, 성대 부전이나 윤상인두 부전(cricopharyngeal dys- function), 인두식도 협착(pharyngoesophageal stric- ture) 등이 원인이 되어 연하장애가 발생하는 경우는 일 반적으로 수술적 치료를 필요로 한다.(Table 1) 반대로, 진행성 신경근육 질환, 뇌경색, 또는 다발성신경병증(poly- neuropathy) 등에 의한 연하장애의 경우는 수술의 역할 이 논란의 여지가 있다1. 저자는 수술적 치료가 필요한 연하장애의 원인과 각각의 원인에 따른 수술방법에 대해
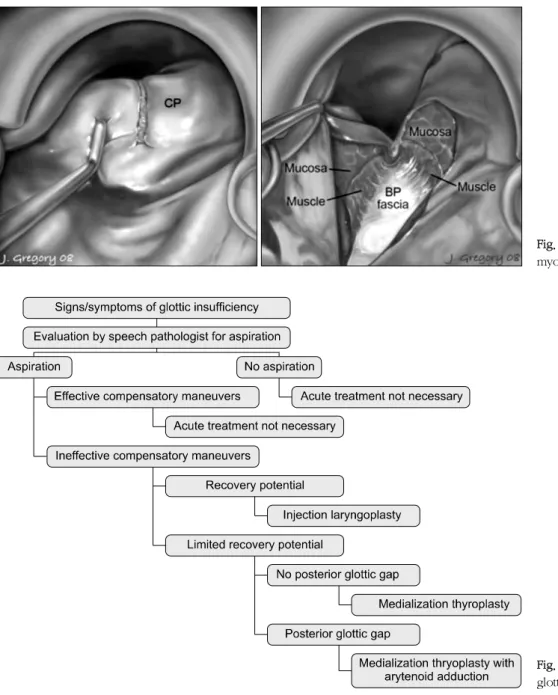
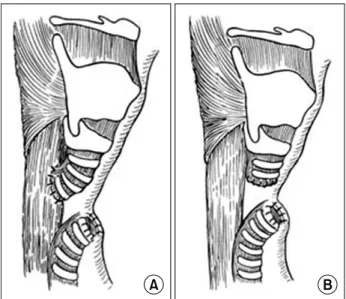
Fig. 1. External criopharyngeal myotomy. It should be trans- ect all fibers as close to posterior median raphe as possible.
논의하고자 한다.
윤상인두 부전(Criopharyngeal dysfuction) 윤상인두근은 하인두와 식도의 접합부에 위치하고 있고 복잡한 연하운동에서 중요한 역할을 한다. 이 근육은 인두 기의 연하운동 동안에 지속적인 수축과 일시적인 이완을 유지하면서 식괴가 식도로 이동하게 한다. 따라서 이 근육 의 수축과 이완이 식도기의 연하운동에 중요한 역할을 한 다는 것을 알 수 있다. 윤상인두 부전은 중증 근무력증, 근 육 위축증, 뇌경색 등의 질환에서 발생하며, 윤상인두근이 수축이 조화롭게 일어나지 못하면 연하장애를 유발한다.
그리고, Video Fluoroscopic Swallowing Study (VFSS) 의 측면 사진에서 윤상인두의 bar나 부조화된 근육의 수축 등의 소견을 보인다1.
윤상인두 부전의 치료에서 먼저 상부 식도 괄약근의 이 완을 유도할 수 있는 Botulinum toxin의 주입을 고려할 수 있으나 효과는 일시적이어서 반복적인 주입이 요구된 다4. Botulinum toxin의 주입이 효과가 없는 경우는 윤 상인두근 절개술을 고려해야 한다. 수술 전에 굵은 기도 삽관 튜브나 위세척용 튜브를 식도 내에 넣어 놓으면 수 술 중에 윤상연골 뒤에 위치하는 이 근육을 쉽게 확인할 수 있으며 절개할 수 있다. 근육을 절개할 때는 원위부 하인두수축근, 윤상인두근, 식도근의 상부 환상근을 모두 포함해야 하고 반회신경의 손상을 피하기 위하여 후두를 반대방향으로 돌리고 가능한 한 뒤쪽에 절개해야 한다4-6. (Fig. 1.) 현수 직달내시경하에서 레이저나 전기소작기를 이용하여 수술할 수도 있는데 이 방법은 수술시간이 짧고 외부 접근법보다는 덜 침습적이지만 종격동염이 발생할 가능성이 있다는 단점이 있다5,7.(Fig. 2.)
윤상인두근 절개술의 유용성에 대해서는 논란의 여지
가 있으나 뇌졸증 후에 오는 흡인환자에게 효과적이라고 알려져 있다1,2.
성대 부전(Glottic insufficiency)
후두는 기도 보호, 호흡, 발성이라는 3가지의 기본적인 기능을 가지고 있다. 성대부전은 성대 주름이 완전히 닫 히지 못해서 호흡이나 발성 동안 하부기도를 보호하지 못 하게 되는 것을 말한다. 보통 성대마비에 의해 발생하고,
Fig. 2. Endoscopic criopharyngeal myotomy with CO2 laser.
Fig. 3. Algorithm for treatment of glottic insuffiency.
신경손상의 위치(상부 미주신경 또는 되돌이 후두신경의 단독 손상)에 따라 감각 및 운동 손상이 발생할 수 있다.
이러한 상황은 일시적일 수도 영구적일 수도 있는데 일시 적 손상의 원인은 뇌경색이나 삽관 후 외상 그리고 수술 에 의해 발생할 수 있다. 이러한 원인들이 또한 영구적 손상을 유발할 수도 있다. 성대부전의 수술적 치료는 매 우 다양하고 치료방법의 선택은 회복가능성이나 성대 마 비의 정도, 음성이나 연하장애 정도, 흡인성 폐렴의 위험 성 등을 고려하여 결정하게 된다1,8.(Fig. 3.)
후두내 주입술(injection laryngoplasty)
후두내 주입술은 다른 술식에 비하여 간단하게 병변쪽 성대 유리연을 내측으로 이동시킴으로써, 성문틈을 교정 할 수 있어 환자에게 부담이 적은 술식이다. 성대내 주입 은 보통 피부를 통해서 하거나 구강을 통해서 시행하게 된다9. 주로 경피적 주입술이 사용되며, 이 방법은 윤상갑 상막을 통해 곧은 주사침을 찌른 후 외측으로 갑상피열근 방향으로 바늘을 진행시킨다. 테프론이나 hydroxyap- atitie와 같은 비흡수성 물질의 경우에는 성대근의 깊숙한 부위에 질러 성대 점막부위의 변형과 강직, 돌출 등을 예
Table 2. CTCAE 3.0 aspiration grade.
Grade Description
I II
III
IV
Asymptomatic; clinical or diagnostic observations only;
intervention not indicated
Altered eating habits; coughing or choking episodes after eating or swallowing; medical intervention indicated (e.g., suction or oxygen)
Dyspnea and pneumonia symptoms (e.g., aspiration pneumonia); hospitalization indicated; unable to aliment orally
Life-threatening respiratory or hemodynamic compromise; intubation or urgent intervention indicated
Table 3. Surgical management of chronic aspiration.
Reversible procedures Irreversible procedures Laryngotracheal separation Subperichondrial
cricoidectomy
Tracheoesophageal diversion Narrow-field laryngectomy Epiglottic flap laryngeal closure Glottic closure
Endolaryngeal stent Partial cricoidectomy
Vertical laryngoplasty Fig. 4. A. Endolaryngeal stent. B. Vented endolaryngeal stent.
점이 있다. 실리콘, vocom, Gortex 등의 이식물을 선택 해서 사용할 수 있다1,8,10.
피열연골 내전술(arytenoid adduction)
원통형의 윤상피열관절의 해부학적 특징 때문에 마비 된 성대는 건측 성대보다 높게 위치하는 경우가 많다. 이 러한 경우 갑상성형술로는 만족할 만한 결과를 얻을 수 없고 피열연골 내전술이 우선적으로 적용할 수 있는 술식 이다. 피열연골 내전술은 기술적인 어려움이 있으나 생리 적인 방식으로 피열연골의 성대돌기를 내전 및 회전시켜 줌으로써 넓은 성문 후부틈이나 높아진 마비측 성대를 충
의 원인과 정도, 연하기능의 회복가능성, 환자나 가족의 요구 등 여러 가지를 고려하여 결정해야 한다.
항흡인 스텐트(Endolaryngeal stents)
하부기도를 스텐트를 이용하여 보호하려는 시도가 여 러 사람들에 의하여 시도되었다. 이는 기관절개술을 하고 마치 포도주병의 코르크 마개처럼 후두를 막아서 하부기 도를 보호하고 음식물이 타액이 하인두로 흘러 들어가게 하는 방법이다. Weisberger와 Huebsch 등은 딱딱한 실 리콘을 사용하였고, Eliachar 등은 두 가지 형태의 구멍이 있는 실리콘 스텐트를 보고하였는데,(Fig. 4.) 스텐트 크 기가 맞지 않아 주위로 음식물이 새거나 스텐트가 빠질 우려가 있고 장시간 착용하면 후두 내에 스텐트 압력으로 인하여 합병증이 생길 수 있으므로 단기간만 사용해야 한 다10,11.
성문 폐쇄술(Glottic closure)
Montgomery는 진성대, 가성대, 후두실, 후연합부의 점막을 제거하고 진성대와 가성대를 접합하는 방법을 소
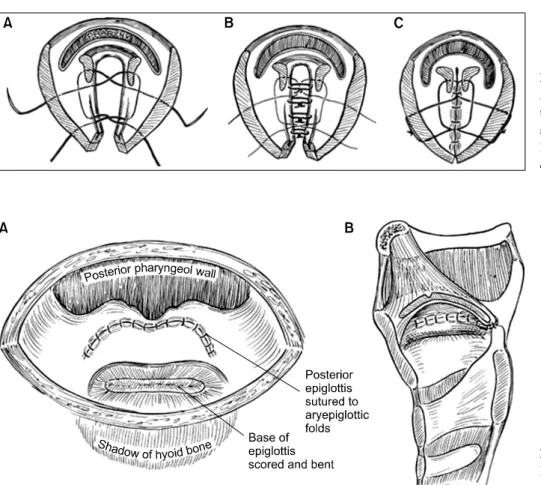
Fig. 5. Glottic closure procedure.
A. Midline thyrotomy, removal of the glottic mucosa and transglottic sutures placed for closure. B.
False vocal cords are approximat- ed. C. The glottis is closed.
Fig. 6. Epiglottic flap closure of larynx. A. Superior view. B. Lateral view.
개하였다.(Fig. 5.) 이 방법은 음성은 소실되나 성공률은 95%이다12-14.
후두 거상법(laryngeal suspension)
설골이나 갑상연골의 lamina를 하악에 거상하는 방법 으로 후두를 앞쪽 및 위쪽으로 위치시켜 식도입구를 열어 서 음식물이 이동하도록 도와주게 하는 술식이다6. 후두개피판폐쇄술
후두개, 피열후두개주름, 피열연골의 끝을 박리하고 접 합하는 방법이다.(Fig. 6.) 진성대를 보호할 수 있고 가역 적으로 사용할 수 있다는 장점이 있으나 수술 후에 접합 한 부위가 벌어지는 경우가 많고 성문상부 협착 등의 합 병증이 올 수 있다10.
수직 후두성형술(vertical laryngoplasty)
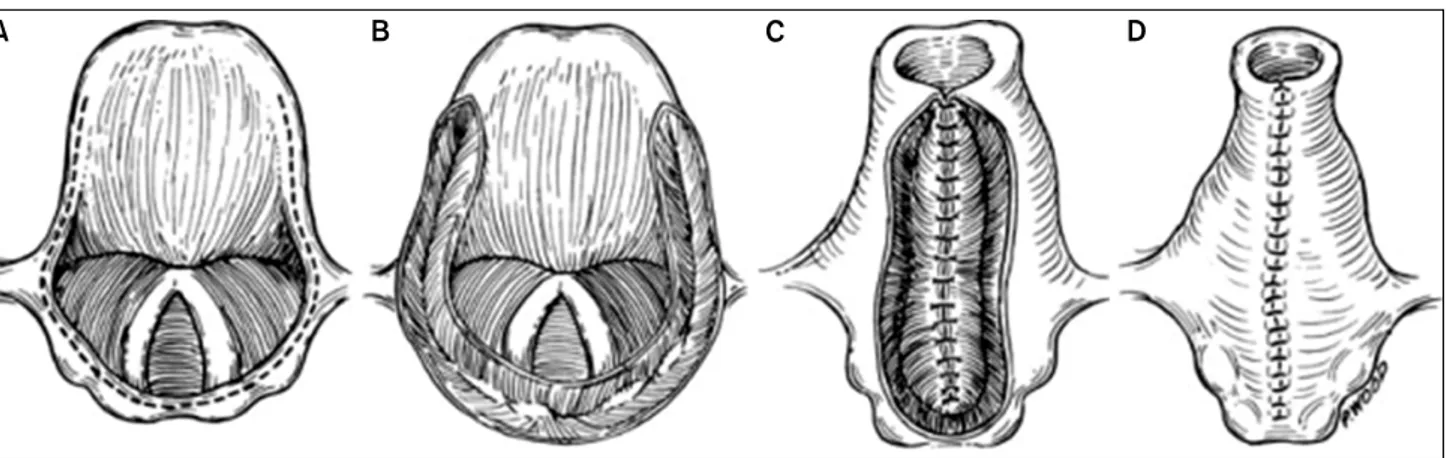
설 전절제술 후 흡인을 막기 위하여 Biller가 소개한 술 식으로, 외측 구인두 절개술 후 후두개의 외측연을 다라 절개를 가하고 피열후두개주름, 피열간극까지 절개선을 연장하여 윗부분은 열린 상태로 두고 두 층으로 관 형태
를 만들어 봉합하는 방법이다.(Fig. 7.) 음성을 보존할 수 있으며 성공률이 60-70% 정도이다1,10.
부분 윤상연골절제술(partial cricoid resection) 윤상연골의 후방부위를 점막아래로 박리하고 윤상연골 의 후방부위를 제거하여 하인두를 넓히고 기도부위를 좁 게 만들어 연하작용을 돕고 흡인되는 것을 방지하는 방법 이다. 음성은 보존할 수 있으나 영구 기공이 필요하고 오 랫동안 추적 관찰된 결과가 없어 성문하 협착 등의 합병 증이 얼마나 오는지에 대해서는 분명하지 않다1,10. 협영역 후두전절제술(narrow-field total laryngectomy)
협영역 후두전절제술은 이미 음성을 소실한 환자에서 진행하거나, 지속적으로 생명을 위협하는 만성흡인이 있 을 때 가장 효과적인 수술법이다. 후두암수술에서 통상 시행되는 후두전절제술과 달리 설골, 피대근, 그리고 가능 한 많은 하인두 점막을 보존하여 점막의 긴장이 없는 상 태에서 접합하여야 인두피부누공 등의 술 후 합병증을 예 방할 수 있다1,10.(Fig. 8.)
Fig. 8. Narrow-field laryngectomy. A. Outline of larynx removal; the hyoid is preserved. B. Closure of the pharynx. C. Closure is reinforced with sternohyoid muscles. D. A tracheostoma is created.
Fig. 7. Vertical laryngoplasty. A. Incision along epiglottis, aryepiglottic folds, arytenoids, and interarytenoid area. B. Submucosal flaps are created. C. Inner layer closure. D. Outer layer closure.
연골막하 윤상연골절제술(subperichondrial cricoidectomy)
후두전절제술보다 간단하고 합병증도 적으며 효과가 있는 술식이다.(Fig. 9.) 이 방법은 후두전절제술보다 선 호되는 방법이나 영구기관구가 남고 비가역적인 수술 방 법이다15.
기관식도 전환술(tracheoesophageal diversion)과 후두기관 분리술(laryngotracheal seperation) 기관식도전환술의 술식은 기관연골 네 번째와 다섯 번 째 사이를 수평으로 자르고 근위부는 식도에 단측으로 접 합하고 원위부는 후두전절제술에서 영구 기관절개창을 만 드는 것과 같은 방법이다. 또 이미 기관절개술을 한 환자 에게는 식도와 문합하는 것이 어려워 기관의 기시부를 맹 관으로 닫아버리는 변형된 방법인 후두기관분리술을 시행
한다. 발성의 회복이 이론적으로 가능하며 환자가 신경학 적으로 회복하였을 때 다시 이전상태로 복구가 가능한 가 역적인 방법이다16-20.
기관절개술과 연하장애
기관절개술은 기관 삽관이 필요한 환자에게 편안하게 기도를 유지할 수 있고, 분비물이 많은 경우 적절히 제거 할 수 있는 흡인 치료 중 가장 고전적인 방법이다. 그러 나, 기관캐눌러의 기낭만으로 흡인을 효과적으로 막을 수 있는 것은 아니다. 즉, 기관절개술을 하고 있으면 연하반 사가 일어났을 때 후두의 상승을 막고, 기낭에 공기를 넣 으면 식도에 압력이 전해져, 연하작용을 방해할 수 있으 며, 인두의 압력발생으로 인하여 연하작용을 방해할 수 있고, 성문하압을 낮추어서 흡인을 일으킨다. 따라서 가 능한한 기관캐뉼러를 장기간 장착하지 않도록 해야 한 다1,21. 즉, 기관절개술은 연하장애의 치료를 위한 것이 아
Fig. 10. A. Trachoesophageal diversion, B. Laryngotracheal se- peration.
Fig. 9. Subperichondrial cricoidectomy. A. Cricoid incision. B. The cricoid cartilage is opened. C. Outer cricoid perichondrial dissection. D. Inner cricoid perichondrial dissection. E. The inner perichondrium and mucosa are divided and closed. F. Cut ends of the inner mucosal tube are folded in, and the sutured end is closed. G. The sternohyoid muscle is insinuated into the cricoid space. H. Closure with the outer perichondrium closed over muscle.
니라 호흡기계의 유지를 위해서 고려되어야 할 방법이다.
타액분비 과잉증(Sialorrhea)
타액 분비 과잉증의 타액의 과도한 생성과 타액의 조절 실패의 두 가지 의미를 모두 포함한다. 뇌성마비를 가진 소 아나 파킨슨병이나 뇌졸증의 가진 성인에서 흔히 발생한 다. 수술적 치료는 일반적으로 지속적인 침흘림이 있을 때 시행할 수 있는데 신경차단부터 침샘의 제거까지 다양하게 수술이 이루어질 수 있다. 심한 침흘림에서는 침샘의 제거 가 가장 효과적이며 최선의 치료가 될 수 있다22-24. 결론
연하장애에서는 원인을 정확히 진단하는 것이 예후나 치 료방법을 결정하는데 가장 중요하다. 환자의 생명을 위협 할 만한 흡인이 있다고 판단되면 보존적 치료를 시도해 본 후 효과가 없다고 판단되면 즉시 적절한 수술적 방법으로 이를 교정해야 한다. 난치성의 만성흡인이 신경계의 이상 과 동반되어 있고 회복가능성이 없다면 연골막하 윤상연골 절제술이나 협영역 후두전절제술을 고려해야 한다. 하지만 회복이 가능한 환자라면 가역적인 수술방법인 후두기관분
리술을 먼저 시행하여 만성흡입을 막아야 할 것이다.
REFERENCES
1. Shama L, Connor NP, Ciucci MR, McCulloch TM. Surgical
Head Neck Surg. 2006;14:437-41.
6. Fujimoto Y, Hasegawa Y, Yamada H, Ando A, Nakashima T. Swallowing function following extensive resection of oral or oropharyngeal cancer with laryngeal suspension and cricopharyngeal myotomy. Laryngoscope. 2007;117:
1343-8.
7. Pitman M, Weissbrod P. Endoscopic CO2 laser cricophar- yngeal myotomy. Laryngoscope. 2009;119:45-53.
8. Flint PW, Purcell LL, Cummings CW. Pathophysiology and indications for medialization thyroplasty in patients with dysphagia and aspiration. Otolaryngol Head Neck Surg.
1997;116:349-54.
9. Courey MS. Injection laryngoplasty. Otolaryngol Clin North Am. 2004;37:121-38.
10. Pletecher SD, Eisele DW. Chronic aspiration. In: Cummings CW, Fredrickson JM, Harker LA, Krause CJ, Schuller DE, ed. Otolaryngolgoy-head and neck surgery. 4th ed. St Louis:
Mosby Year Book; 2005:2077-87.
11. Weisberger EC. Treatment of intractable aspiration using a laryngeal stent or obturator. Ann Otol Rhinol Laryngol.
1991;100:101-7.
12. Sato K, Nakashima T. Surgical closure of the larynx for intractable aspiration: surgical technique using closure of the posterior glottis. Laryngoscope. 2003;113:177-9.
13. Qu S, Su Z, He X, Li M, Li T. Closure of laryngotracheal cavity and tracheostomy for intractable aspiration secon- dary to radiation encephalopathy or radiation damage of
Laryngol. 1988;97:471-5.
17. Eisele DW, Yarington CT, Jr., Lindeman RC, Larrabee WF, Jr. The tracheoesophageal diversion and laryngotracheal separation procedures for treatment of intractable aspi- ration. Am J Surg. 1989;157:230-6.
18. Wang D, Dulguerov P. Laryngeal diversion and tracheo- tracheal speech fistula for chronic aspiration. Ann Otol Rhinol Laryngol. 2000;109:602-4.
19. Tomita T, Tanaka K, Shinden S, Ogawa K. Tracheoeso- phageal diversion versus total laryngectomy for intractable aspiration. J Laryngol Otol. 2004;118:15-8.
20. Zocratto OB, Savassi-Rocha PR, Paixao RM, Salles JM.
Laryngotracheal separation surgery: outcome in 60 pati- ents. Otolaryngol Head Neck Surg. 2006;135:571-5.
21. Goldsmith T. Evaluation and treatment of swallowing dis- orders following endotracheal intubation and trache- ostomy. Int Anesthesiol Clin. 2000;38:219-42.
22. Meningaud JP, Pitak-Arnnop P, Chikhani L, Bertrand JC.
Drooling of saliva: a review of the etiology and manage- ment options. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:48-57.
23. Reychler H. Treatment of drooling: review of the literature.
Rev Stomatol Chir Maxillofac. 2006;107:445-8.
24. Molloy L. Treatment of sialorrhoea in patients with Parkin- son's disease: best current evidence. Curr Opin Neurol.
2007;20:493-8.