Tuberc Respir Dis 2010;69:191-195
CopyrightⒸ2010. The Korean Academy of Tuberculosis and Respiratory Diseases. All rights reserved.
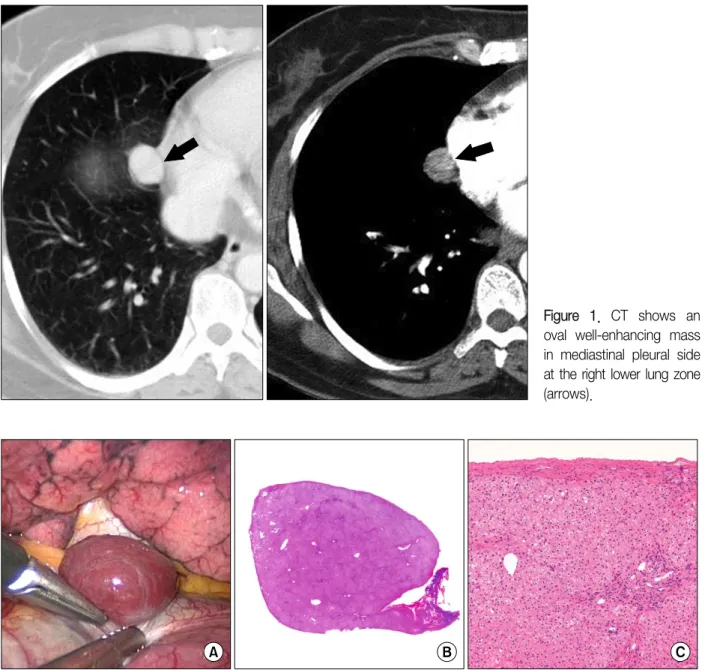
Supradiaphragmatic Heterotopic Liver Presenting as a Pleural Mass:
A Case Report
Jungsuk An, M.D.
1, Joungho Han, M.D.
2, Kyung Soo Lee, M.D.
3, Yong Soo Choi, M.D.
41