pISSN 2765-7833 eISSN 2765-7841
Journal of implantology and applied sciences 2021; 25(2): 84-94
https://doi.org/10.32542/implantology.2021009
Received: March 10, 2021 Accepted: March 30, 2021 ORCID
Youngdeok Chee
전체 글
Received: March 10, 2021 Accepted: March 30, 2021 ORCID
Youngdeok Chee
수치

관련 문서
HEMORRHAGE OF SUBLINGUAL REGION AND AIRWAY OBSTRUCTION THAT OCCURRED AFTER DENTAL IMPLANT PLACEMENT ON MANDIBLE ANTERIOR EDENTULOUS AREA : CASE REPORT.. Seung-Bin Yang,
Table Ⅵ.. Meier cumulative survival rate을 Fig. 보철물에 문제가 발생하는 추정 시점은 9.5년이었다. Kaplan-Meier cumulaltive survival curve of implant
나사-시멘트 보철물(screw-cement prosthesis)은 나사-시멘트 유지형(SCRP: screw and cement retained implant prosthesis)과 시 멘트
Restoration of Mandibular Edentulous Patient By Dental Implant: Case Report.. Ji-Yung Kwon DDS a , Yung-Soo Kim DDS, MSD, PhD,
In this case of partially edentulous patient with crossed occlusion, each edentulous area was restored with implant fixed prosthesis and implant retained partial denture to suit
A computed tomographic scan-derived customized surgical template and fixed prosthesis for flapless surgery and immediate loading of implants in fully edentulous maxillae:
This study shows a case in which implant-supported removable partial denture was fabricated considering residual alveolar bone height after teeth loss in a patient who had been
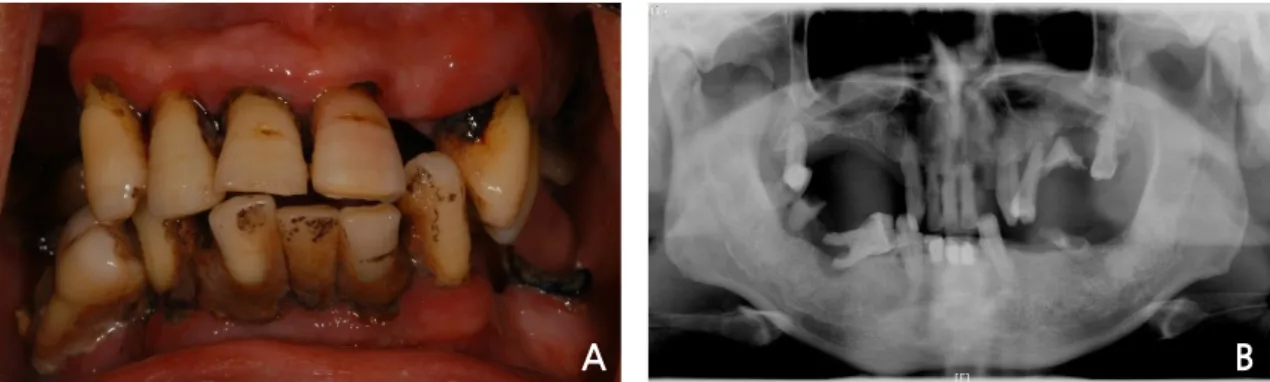
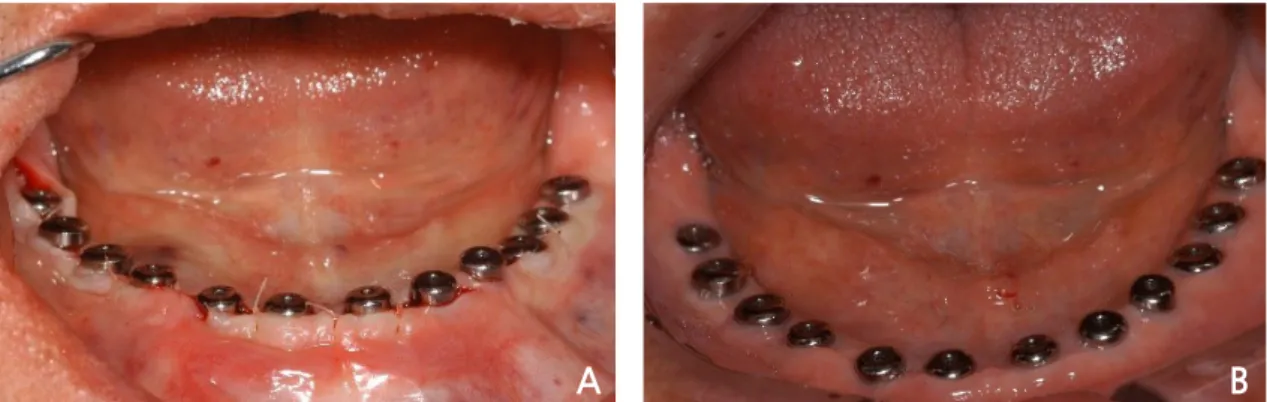
A 61-year-old man was referred for an edentulous maxilla and mandible (Fig. The patient complained of unstable mandibular and uncomfortable maxillary complete