대한안과학회지 2010년 제 51 권 제 1 호 J Korean Ophthalmol Soc 2010;51(1):131-135 ISSN 0378-6471 (Print) ISSN 2092-9374 (Online) DOI : 10.3341/jkos.2010.51.1.131
= 증례보고 =
안와봉와직염의 호전 중 발생한 전두엽의 농양 1예
송현재⋅지미정
가천의과학대학교 길병원 안과학교실
목적: 안와봉와직염의 호전 중 발생한 전두엽의 농양을 경험하였기에 이를 보고하고자 한다.
증례요약: 54세 남자환자가 2일 전부터 발생한 좌안와 부위의 통증, 부종, 시력저하를 주소로 내원하였다. 좌안의 최대 교정시력은 0.3, 안압은 27 mmHg이었으며, 전방향의 안구운동장애가 있었고 4 mm 안구돌출 소견이 있었다. 안와전산화단층촬영상 전 부비동염 과 좌안와봉와직염이 관찰되어 이비인후과에서 부비동 수술을 시행 후 항생제 치료를 하였으나 호전이 없었고 술 후 11일 째 촬영한 안와전산화단층촬영상 안와에 국한된 농양이 있어 절개 및 배농술을 시행하였다. 술 후 좌안 최대 교정시력 0.8, 부종 및 안구운동은 호전 되었으나 15일째 갑자기 발생한 두통을 호소하여 시행한 뇌 자기공명 영상촬영상 좌측 전두엽의 농양이 발견되어 신경외과에 의뢰해서 항생제 및 만니톨 정주 치료 하면서 경과 관찰 하였다. 두통은 점차 소실되었으며, 발병 3개월 째 촬영한 뇌자기공명영상촬영 상 뇌농양도 거의 소실되었고, 발병 6개월째 안구운동 장애 소견 없으며 최대교정 시력은 1.0이었다.
결론: 안와봉와직염의 호전 중에도 신경학적 증상이 동반되는 경우, 뇌농양을 염두에 두어야겠다.
<대한안과학회지 2010;51(1):131-135>
■ 접 수 일: 2009년 5월 25일 ■ 심사통과일: 2009년 10월 19일
■ 책 임 저 자: 지 미 정
인천광역시 남동구 구월동 1198 가천의과학대학교 길병원 안과
Tel.: 032-460-3364, Fax.: 032-460-3358 E-mail: [email protected]
* 본 논문의 요지는 2008년 대한안과학회 제99회 춘계학술대회에서 포스터로 발표되었음.
안와봉와직염은 안와주위의 해부학적 특징으로 인해 부 비동염의 안와내로의 파급이 가장 흔한 원인으로 알려져 있으며 노출각막병증, 안와농양, 경막외 농양, 뇌수막염, 뇌 농양 등의 여러 가지 합병증을 유발할 수 있다. 항생제의 발달 및 사용으로 이러한 합병증의 빈도가 많이 줄어들었 지만, 이로 인해 합병증의 진단이 지연될 수 있고, 뇌농양과 같은 중추신경계의 감염 등이 조기에 진단되지 못하면 생 명을 위협할 수 있다.1
뇌농양의 원발 병소로는 대개 귀, 유양돌기동 혹은 부비 동이며 이 부위의 감염은 뇌농양으로 직접 파급되는 경우 가 많다.2컴퓨터단층촬영 등의 영상진단기술의 발달과, 효 과적인 항생제 사용 및 수술방법의 발달로 뇌농양으로 인 한 사망률은 현저히 줄었지만 진단이 늦어지거나 적절한 처치를 하지 못할 경우 심각한 후유증이나 사망까지 이를 수 있다.3
저자들은 급성 부비동염을 동반한 안와봉와직염이 수술 및 항생제 치료로 호전되던 중 발생한 신경학적 증상을 동반한 전두엽의 농양을 1예 경험하였기에 이를 보고하고자한다.
증례보고
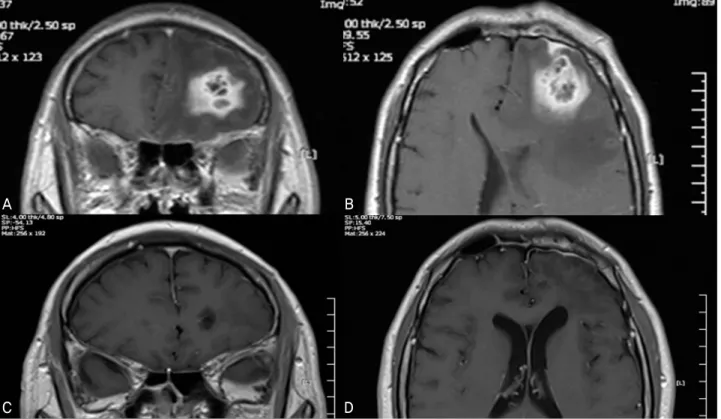
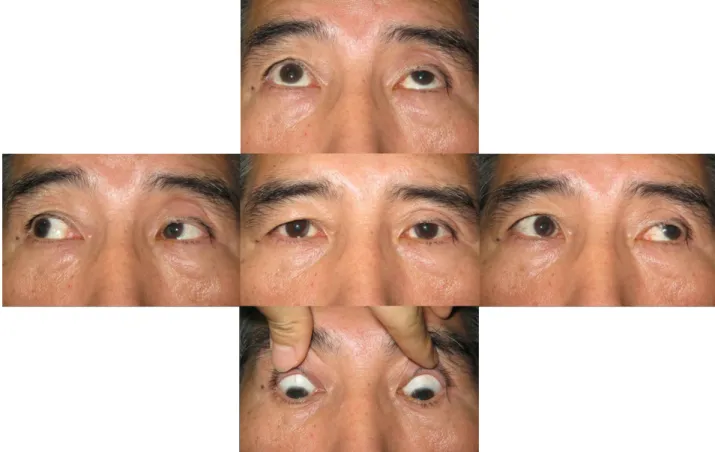
54세 남자환자가 내원 2일전부터 시작된 좌안와 부위의 통증 및 부종, 시력저하를 주소로 내원하였다. 내원 당시 최 대 교정시력은 우안 1.0, 좌안 0.3, 안압은 우안 12 mmHg, 좌안 27 mmHg이었다. 전방향에서 좌안의 안구운동장애 소견을 보였고 우안에 비해 좌안의 4 mm 안구돌출 소견이 있었다(Fig. 1). 안와 컴퓨터단층촬영에서 전 부비동염과 좌안와봉와직염이 관찰되어 본원 이비인후과로 입원하여 같은 날 내시경적 부비동 수술을 시행하였으며, 이후 전신 적인 항생제 치료를 시작하였다(Fig. 2A). 수술적 치료에 도 불구하고 안와부위 부종이 심해져 부비동 수술 후 11일 째 재촬영한 안와 전산화 단층 촬영상 뇌 실질 및 주변부 파급이 없는 안와 농양 소견 있어 절개 및 배농술을 시행하 였다(Fig. 2B, C, D). 농양 분비물은 고린내가 나는 녹황색 소견을 보였으며, 분비물의 세균배양검사상 혐기성균인 Clostridium perfringens가 검출되었다. 술 후 경과는 양호 하여 15일째까지 좌안 최대 교정시력 0.8, 안압 15 mmHg, 안와부위 부종 및 안구 운동 제한이 거의 호전 되어 퇴원을 계획하던 중 환자는 갑자기 심한 두통을 호소하여 뇌 자기공 명 영상촬영을 시행하였고 좌측 전두엽의 농양이 발견되어 신경외과에 의뢰하여 항생제 및 만니톨 정주 치료하면서 경 과 관찰하였다(Fig. 3A, B). 이후 두통은 점차 소실되었으며, 발병 3개월째 마지막으로 촬영한 뇌 자기공명영상 촬영상 뇌 농양도 거의 소실되었고(Fig 3C, D), 발병 6개월째 안구운동
Figure 1. Photographs at admission. These photographs demonstrate periorbital swelling, ptosis, exophthalmos and restriction of eye movement in the left eye.
장애 소견 없었으며 최대교정시력은 1.0이었다(Fig. 4).
고 찰
안와봉와직염은 경미한 경우를 제외한 모든 환자에서 입 원하여 적극적인 치료를 받아야 하는 응급 질환이며 소아 및 성인 모두에게 발병할 수 있다. 원인으로는 안와주위 감 염의 직접적인 전파, 안와의 외상, 원발성 균혈증으로 인한 전이 등이 있으며 이중 부비동염의 안와내로의 전이가 가장 흔하다. Chandler et al5, Bergin and Wright6의 보고에 의하면 안와감염의 70~80%는 부비동염에서 기인하며, Birch‐Hirschfeld7 는 원인이 되는 부비동염의 순서를 전두동, 상악동, 사골동, 접형동, 전부비동 순이라고 했다. 이는 안와벽의 2/3 이상이 부비동으로 둘러싸여 있는 특징적인 해부학적 구조로 인한 주 변 감염 물질의 직접적인 전파 또는 밸브가 없는 안면정맥을 통한 역행성 혈전 정맥염 등을 이유로 생각할 수 있다.4
안와봉와직염이 의심되는 환자가 내원시 안과, 이비인후
과, 감염내과 그리고 신경과적 진찰이 철저하게 시행되어야 하고, 안와 컴퓨터단층촬영 또는 자기공명영상의 촬영과 백 혈구증가증의 확인 및 원인균의 동정을 위해 혈액 검사 및 배양이 필요하다. 본 증례의 환자는 초진 시 시행한 혈액검 사상 백혈구수치가 16, 110으로 상승되었고, 혈액 세균배 양검사에서는 특정 균이 동정되지 않았다. 치료는 이러한 진단적 검사들과 동시에 경험적인 항생제 정주가 즉시 시 행되어야 하며, 추후 배양검사 결과에 따라서 항생제의 변 경 투여를 고려할 수 있다. 원인이 부비동염일 경우 내시경 적 부비동 수술을 치료로써 고려해야 하며, 부비동의 세균 배양검사도 시행되어야 한다. 본 증례의 환자에서는 부비동 의 세균배양검사 결과 부비동염의 흔한 원인 균주인 S.
aureus가 동정되었다. 치료가 늦어지거나 적절한 항생제 사 용을 못할 경우 안와부위의 농양, 시력 상실, 안구 운동의 장애, 해면정맥동 혈전증, 뇌농양 등의 합병증이 발생 가능 하다. 만약 안와부위 농양이 발생했을 경우 농양의 절개 및 배농술, 세균배양검사가 시행되어야 하며 본 증례의 환자는
- 송현재 외 : 안와봉와직염 호전 중 발생한 뇌농양 -
A B
C D
Figure 2. (A) Orbital CT scan at admission. Enhanced soft tissue densities in left orbit and both maxillary sinus, ethmoid, sphenoid, frontal sinus. (B, C, D) Follow up orbital CT scan. Aggravated state of Inflammation in left orbit (abscess formation) and no evidence of intracranial extension of inflammation.
A B
C D
Figure 3.(A, B) T1-weighted MRI scans. Newly developed enhancing multilocular lesion (abscess) and surrounding edema in left forntal lobe. (C, D) Follow up T1-weighted MRI scans. Improved state of brain abscess and atrophic change of left frontal lobe.
Figure 4. Photographs at final visit. Almost recovered restriction of left eye movement.
안와 농양의 절개 및 배농술시 시행한 세균배양검사에서 피부나 연조직의 감염을 유발하는 그람양성, 혐기성 간균인 Clostridium perfringens가 동정되었다.
뇌는 다른 장기들과 비교하여 세균 및 곰팡이 감염에 현 저하게 저항성이 강한 것으로 알려져 있으며, 특히 사람에 서는 명확하거나 잠재적인 균혈증이 흔히 있음에도 뇌농양 이 흔히 발생하지 않는다.8 이는 뇌가 풍부한 혈액 순환이 일어나는 장기이며 모세혈관과 내피세포 사이에 폐쇄연접 (tight junction)으로 혈액-뇌관문(blood-brain barrier)이 상대적으로 높은 비투과성을 가지기 때문이다.하지만 안와 는 배(pear) 모양의 공동으로 눈꺼풀과 안와를 분리하는 얇은 벽인 안와 격막을 포함하고 있고, 안와 격막은 두개골 의 골막에서 기원하며 안와의 골막과 뇌의 경뇌막에 인접 해 있어 안와내의 감염이 발생할 시 두개강내로 직접 파급 될 수 있어 뇌수막염이나 해면정맥동 혈전증, 뇌농양 등의 생명을 위협할 수 있는 치명적인 합병증이 발생할 수 있고 뇌신경을 침범하여 복시를 유발할 수도 있다.9-12안와봉와 직염과 부비동염이 동반된 환자에서의 뇌농양 발생률은 3%에서 45%까지 다양하게 보고되었고,12-16이는 만성 부 비동염 환자에서 점막의 만성적인 변화와 기저부위의 뼈들 의 구조적인 변화 등으로 인해 감염이 직접적으로 전파되 어 발생하는 경우가 가장 흔한 위험인자로 알려져 있으
며,11,16 적절한 시기의 항생제 치료 또는 수술적 치료가 안
되었거나, 치료를 시행했더라도 이에 반응을 보이지 않고 진행하는 경우 발생하는 것이 대부분이다. 하지만 본 증례 에서처럼 항생제 치료 및 수술이 늦지 않게 시행되었고, 이 에 반응을 보여 호전 중이던 안와봉와직염 환자에서 합병 증으로 뇌농양이 발병된 예는 보고된 적이 없었다.
본 증례에서는 성인 안와봉와직염 환자에서 적절한 수술 적 치료와 항생제 투여를 시행했고, 이에 반응을 보이며 호 전 중에 갑작스런 두통을 동반한 전두엽의 농양이 발생했다.
따라서 안와봉와직염 환자에서 수술 및 항생제 치료에 반응 을 보이며 호전 중인 환자라도 고열, 두통, 구토 및 드물지만 등뼈, 목뼈, 척추뼈 통증 등의 신경학적 증상을 호소하는 경 우, 심각한 합병증인 뇌농양을 필히 염두에 두어야 하겠다.
참고문헌
1) Martin-Hirsch DP, Habashi S, Hinton AH, Kotecha B. Orbital cellulitis. Arch Emerg Med 1992;9:143-8.
2) Gallagher RM, Gross CW, Phillips CD. Suppurative intracranial complications of sinusitis. Laryngoscope 1998;108:1635-42.
3) Xiao F, Tseng MY, Teng LJ, et al. Brain abscess: clinical experience and analysis of prognostic factors. Surg Neurol 2005;63:442-50.
4) Lavania A, Sharma V, Reddy NS, Baksh R. Orbital cellulitis-a complication of sinusitis. Kathmandu Univ Med J 2005;3:292-3.
- 송현재 외 : 안와봉와직염 호전 중 발생한 뇌농양 -
=ABSTRACT=
Brain Abscess Formation Accompanied by Improvement of Orbital Cellulitis
Hyun Jai Song, MD, Mi Jung Chi, MD
Department of Ophthalmology, Gachon University, Gil Hospital, Incheon, Korea
Purpose: To present a case of brain abscess formation accompanied by improvement of orbital cellulitis.
Case summary: A 54-year-old male came to our clinic complaining of swelling and pain of the left periorbital area and de- creased visual acuity (VA) of the left eye. Initial best-corrected visual acuity (BCVA) was 0.3 and intraocular pressure was 27 mmHg in the left eye. Eye movement in all directions was restricted and 4 mm of proptosis was observed in the left eye. An orbital CT scan demonstrated pansinusitis and orbital cellulitis of the left eye. The patient underwent endoscopic sinus surgery and was treated with systemic antibiotics. However, periorbital swelling was aggravated and another orbital CT scan was per- formed and analyzed. The CT scan showed localized periorbital abscess of the left eye, and the authors performed an incision and drainage (I&D) of abscess procedure. After the operation, BCVA of the left eye was recovered to 0.8 and eye movement improved and periorbital swelling decreased. However, 15 days after the I&D, the patient complained of a severe headache. Brain magnetic resonance imaging (MRI) was performed and showed an abscess of the left frontal lobe of the brain. The authors con- sulted with a neurosurgeon, and the patient received intravenous antibiotics and mannitol. The headache steadily decreased, and three months after the first visit, a follow-up brain MRI was performed. The MRI showed almost complete disappearance of the abscess and six months after the first visit, BCVA was recovered to 1.0 and eye movement was full in all directions.
Conclusions: Although orbital cellulitis is improved by treatment of antibiotics and surgery, if the patient complains of neurologic symptoms such as headache, other complications such as brain abscess formation should be considered.
J Korean Ophthalmol Soc 2010;51(1):131-135
Key Words: Brain abscess, Complication, Orbital cellulitis, Sinusitis
Address reprint requests to Mi Jung Chi, MD
Department of Ophthalmology, Gachon University, Gil Hospital
#1198 Guwol-dong, Namdong-gu, Incheon 405-760, Korea
Tel: 82-32-460-3364, Fax: 82-32-460-3358, E-mail: [email protected] 5) Chandler JR, Langenbrunner DJ, Stevens ER. The pathogenesis of orbital complications in acute sinusitis. Laryngoscope 1970;80:
1414-28.
6) Bergin DJ, Wright JE. Orbital cellulitis. Br J Ophthalmol 1986;
70:174-8
7) Birch-Hirschfeld. Textbook of ophthalmology, Vol. 5. St. Louis:
Mosby, 1952;5420-43.
8) Mathisen G, Johnson JP. Brain abscess. Clin Infect Dis 1997;
25:763-81
9) Betz CS, Issing W, Matschke J, et al. Complications of acute fron- tal sinusitis: a retrospective study. Eur Arch Otorhinolaryngol 2008;265:63–72
10) Shinagawa Y, Ando I, Kukita A, et al. Cellulitis of the eyelids ass- ociated with sinusitis and brain abscess. J Eur Acad Dermatol Ven- ereol 998;11:74-7
11) Tole DM, Anderton LC, Hayward JM. Orbital cellulitis demands
early recognition, urgent admission and aggressive management. J Accid Emerg Med 1995;12:151-3
12) Osborn MK, Steinberg JP. Subdural empyema and other suppur- ative complications of paranasal sinusitis. Lancet Infect Dis 2007;
7:62-7.
13) Giannoni CM, Stewart MG, Alford EL. Intracranial complica- tions of sinusitis. Laryngoscope 1997;107:863-7.
14) Singh B, Van Dellen J, Ramjettan S, Maharaj TJ. Sinogenic intra- cranial complications. J Laryngol Otol 1995;109:945-50.
15) Maniglia AJ, Goodwin WJ, Arnold JE, Ganz E. Intracranial absc- esses secondary to nasal, sinus, and orbital infections in adults and children. Arch Otolaryngol Head Neck Surg 1989;115:1424-9.
16) Reynolds DJ, Kodsi SR, Rubin SE, et al. Intracranial infection ass- ociated with preseptal and orbital cellulitis in the pediatric patient.
J AAPOS 2003;7:413-7.