Journal of the Korean Dysphagia Society 2019;9:89-92 https://doi.org/10.34160/jkds.2019.9.2.006 Case Report
89 Received: February 18 2019, Revised: February 25 2019, Accepted: April 1 2019
Corresponding author: Seong Hoon Lim, Department of Rehabilitation Medicine, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, 93 Jungbu-daero, Paldal-gu, Suwon 16247, Korea
Tel: +82-31-249-7650, Fax: +82-31-251-4481 E-mail: [email protected]
Copyrights ⓒ The Korean Dysphagia Society, 2019.
A Man with Dysphagia after Cervical Esophagogastrostomy: A Case Report
Won Jin Sung, M.D., Bo Young Hong, M.D., Ph.D., Joon Sung Kim, M.D., Ph.D., Jung Jae Lee, M.D., Jae Wan Yoo, M.D., Seong Hoon Lim, M.D., Ph.D.
Department of Rehabilitation Medicine, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Suwon, Korea
Dysphagia caused by a functional gastric outlet obstruction is rare and the natural course of a functional gastric outlet obstruction is unclear. This paper reports a patient with dysphagia and a functional gastric outlet obstruction after a cervical esophagogastrostomy. A 62-year-old man with a history of esophageal cancer and cervical esoph- agogastrostomy presented with dysphagia and discomfort during meals. A videofluoroscopic swallowing study (VFSS) with barium revealed a mild increase in the post-swallow remnants and delayed emptying of the gastric outlet, re- flecting a functional gastric outlet obstruction at the diaphragm. One month later, VFSS revealed a worsened func- tional gastric outlet obstruction at the diaphragm. A delayed chest X-ray showed worsened delayed emptying of the gastric outlet. A cervical esophagogastrostomy for early esophageal cancer can cause functional gastric outlet ob- struction, presenting as dysphagia and discomfort during meals. Physicians should be concerned about dysphagia and the functional changes in the esophagus in patients with a cervical esophagogastrostomy. (JKDS 2019;9:89-92)
Keywords: Esophageal cancer, Cervical esophagogastrostomy, Dysphagia, Gastric outlet obstruction, Hypertensive peristalsis
INTRODUCTION
Functional gastric outlet obstruction is a possible complication after cervical esophagogastrostomy1, and usually results in mild distention of the remnant cervical esophagus. However, the natural course and clinical manifestations of functional gastric outlet obstruction after cervical esophagogastrostomy are not clear.
We report a patient with dysphagia related to functional gastric outlet obstruction after a cervical
esophagogastrostomy. This case illustrates the clinical history and importance of functional gastric outlet obstruction after cervical esophagogastrostomy.
CASE REPORT
A 62-year-old man was referred to our outpatient clinic with a 1-month history of dysphagia and dis- comfort. He had symptoms of dysphagia in asso- ciation with both liquids and solid food, suggesting functional rather than mechanical dysphagia. One
90 Won Jin Sung, et al.:Dysphagia after Cervical Esophagogastrostomy
JKDS Vol. 9, No. 2, 2019
Fig. 3. The findings of esophago- gastroduodenoscopy (EGD). (A) Show- ed no stricture at the anastomosis site. (B) Showed normal findings in the gastric component. The arrow indicated the surgical clip of pre- vious operation.
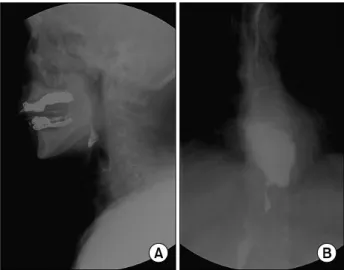
Fig. 1. The initial videofluoroscopic study (VFSS) with barium.
(A) A mild increase in the post-swallow remnants, (B) Distension of the lower esophagus and delayed emptying.
Fig. 2. Delayed chest X-ray (10 minutes after the initial VFSS) showed that most of the barium had disappeared and de- layed emptying of the esophagus was suggested.
month previously, he had undergone a transhiatal esophagectomy and cervical esophagogastrostomy for esophageal cancer (cT2N0M0). Chest computed tomo- graphy revealed no evidence of cancer recurrence or metastasis. Physical and endoscopic examinations were normal. A videofluoroscopic swallowing study (VFSS) with barium performed to evaluate the dysphagia showed a mild increase in the post-swallow remnants, but no penetration or aspiration.(Fig. 1A) VFSS of the esophageal phase in the anteroposterior view revealed delayed emptying of the gastric outlet, i.e., functional gastric outlet obstruction at the diaphragm.(Fig. 1B) Chest X-ray 10 minutes after VFSS showed delayed emptying of the gastric outlet.(Fig. 2) He subsequently
underwent esophagogastroduodenoscopy (EGD),(Fig. 3) which revealed no stricture or structural abnormality at the anastomosis site. Therefore, his symptoms were due to functional gastric outlet obstruction rather than mechanical obstruction. His surgeon decided to ob- serve him without intervention for 1 month. One month later, his dysphagia and discomfort after meals had worsened. A repeat VFSS of the esophageal phase in the anteroposterior view revealed worsened functional gastric outlet obstruction at the diaphragm.(Fig. 4) Chest X-ray 10 minutes after VFSS showed aggravated delayed emptying of the gastric outlet.(Fig. 5) Sub- sequently, the patient was treated conservatively with
Won Jin Sung, et al.:Dysphagia after Cervical Esophagogastrostomy 91
JKDS Vol. 9, No. 2, 2019 Fig. 4. A follow-up VFSS with barium showed marked dis-
tension of the lower esophagus and functional gastric outlet obstruction.
Fig. 5. Chest X-ray 10 minutes after the follow-up VFSS showed that most of the barium remained in the lower esophagus, implying aggravated functional gastric outlet obstruction.
prokinetics and followed in the Cardiac & Thoracic Surgery Outpatient Clinic. However, there was no sig- nificant change in his symptoms; we recommended treatment for the functional gastric outlet obstruction, including intrapyloric injections of botulinum toxin, transpyloric stenting, surgical pyloroplasty, and endo- scopic pyloromyotomy based on the VFSS findings.
DISCUSSION
Cervical esophagogastrostomy has become a standard treatment for early esophageal cancer2. Several studies have examined complications that may occur after this operation, among which dysphagia is important3-6. Among all complications after cervical esophago- gastrostomy, the dysphagia has been an important complication. However, the exact pathophysiology of dysphagia after a cervical esophagogastrostomy is not clear. One possible cause is frequent postoperative pharyngolaryngeal reflux leading to pharyngolaryngitis and a chronic cough, aspiration pneumonia, and dys- phagia7. Another study showed that anatomical changes such as a benign stricture can cause dysphagia6. Functional gastric outlet obstruction, presenting as distention of the remnant cervical esophagus, is another
etiology of dysphagia after cervical esophagogastro- stomy1. Overall, frequent inflammation or mechanical changes may induce functional gastric outlet obstruc- tion after a cervical esophagogastrostomy for esophageal cancer.
The pathophysiology of the dysphagia caused by functional gastric outlet obstruction was suggested to be due to a functional change, such as hypertensive peristalsis, rather than to an anatomical change1. Pyloric outlet dysfunction can result from the bilateral vagotomy performed during the surgery8. Therefore, functional gastric outlet obstruction is thought to be due to functional changes in peristalsis and vagus nerve dysfunction. The effects of a benign stricture after cervical esophagogastrostomy are mainly anato- mical rather than functional3. Therefore, dysphagia related to cervical esophagogastrostomy can have two components: anatomical and functional8.
The natural course of dysphagia after a cervical eso- phagogastrostomy is not clear. In our case, the gastric outlet obstruction progressed over time to near total obstruction of esophageal emptying without treat- ment. Another report showed that even in asympto- matic patients, a contrast swallow can detect anasto- motic leakage that results in an increased risk of
92 Won Jin Sung, et al.:Dysphagia after Cervical Esophagogastrostomy
JKDS Vol. 9, No. 2, 2019
developing anastomotic strictures6. Functional gastric outlet obstruction may be treated by intrapyloric injections of botulinum toxin, transpyloric stenting, surgical pyloroplasty, and endoscopic pyloromyotomy, which we recommended9-11.
This case study had some limitations. First, we could not evaluate the effect of the recommended interventions because the patient was still being treated conservatively. Second, an evaluation of esophageal function, such as manometry, is necessary to prove functional gastric outlet obstruction. In this case, the patient wanted to cease further evaluation and in- vasive treatment, further evaluation was not perform- ed. Mechanical obstruction was ruled out by EGD.
Therefore, we deduced that his symptoms were due to functional gastric outlet obstruction. Based on the limitations of VFSS itself, had a difficulty to estimate gastric emptying time. However, chest X-rays taken 10 minutes after VFSS showed the progression of delayed emptying. Therefore, we concluded that the functional obstruction had worsened.
In conclusion, cervical esophagogastrostomy is one cause of dysphagia and functional gastric outlet obstruction. Without proper treatment, the condition may worsen. Appropriate management is necessary for cervical esophagogastrostomy patients.
ETHICAL APPROVAL
The present study was reviewed and approved by the Institutional Review Board of Catholic University, College of Medicine. Informed consent was waived by the board.
CONFLICT OF INTEREST
The authors declare no financial or other conflicts of interest.
ACKNOWLEDGEMENTS
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science and ICT (grant number:2017R1E1A1A01074324).
REFERENCES
1. Koh P, Turnbull G, Attia E, LeBrun P, Casson AG. Func- tional assessment of the cervical esophagus after gastric transposition and cervical esophagogastrostomy. Eur J Cardiothorac Surg. 2004;25:480-5.
2. Bremner RM, DeMeester TR. Surgical treatment of eso- phageal carcinoma. Gastroenterol Clin North Am. 1991;20:
743-63.
3. Lanuti M, DeDelva P, Morse CR, Wright CD, Wain JC, Gaissert HA, et al. Management of delayed gastric emp- tying after esophagectomy with endoscopic balloon dila- tation of the pylorus. Ann Thorac Surg. 2011;91:1019-24.
4. Larburu Etxaniz S, Gonzales Reyna J, Elorza Orúe JL, Asensio Gallego JI, Diez del Val I, Eizaguirre Letamendia E, et al. Cervical anastomotic leak after esophagectomy:
Diagnosis and management. Cirugía Española (English Edition). 2013;91:31-7.
5. Cho KR, Jo WM. Superior mesenteric artery syndrome after esophagectomy with cervical esophagogastrostomy.
Ann Thorac Surg. 2006;82:e37-8.
6. Honcoop P, Siersema PD, Tilanus HW, Stassen LP, Hop WC, von Blankenstein M. Benign anastomotic strictures after transhiatal esophagectomy and cervical esophago- gastrostomy: risk factors and management. J Thorac Cardiovasc Surg. 1996;111:1141-6.
7. Nishimura K, Fujita H, Tanaka T, Matono S, Nagano T, Murata K, et al. Pharyngolaryngeal reflux in patients who underwent cervical esophago-gastrostomy following eso- phagectomy. Dis Esophagus. 2010;23:353-60.
8. Maus MK, Leers J, Herbold T, Bludau M, Chon SH, Kleinert R, et al. Gastric outlet obstruction after esoph- agectomy: Retrospective analysis of the effectiveness and safety of postoperative endoscopic pyloric dilatation.
World J Surg. 2016;40:2405-11.
9. Ahuja, N. K., Clarke, J. O. Pyloric therapies for gastro- paresis. Curr Treat Options Gastroenterol. 2017;15:230-40.
10. Pasricha, T. S., Pasricha, P. J. Botulinum toxin injection for treatment of gastroparesis. Gastrointest Endosc Clin N Am. 2019;29:97-106.
11. Brewer Gutierrez, O. I., Khashab, M. A. Stent placement for the treatment of gastroparesis. Gastrointest Endosc Clin N Am. 2019;29:107-115.