INTRODUCTION
Congenital factor X (FX) deficiency is a rare autosomal recessive genetic disease that induces bleeding disorder.
Patients with moderate-to-severe FX deficiencies may have symptoms similar to that of hemophilia A and B, in- cluding hemarthrosis, intracranial hemorrhage, and gastro- intestinal bleeding [1,2]. The diagnosis can be confirmed by an FX assay. Fresh frozen plasma (FFP) and prothrom- bin complex concentrates have been used as a temporary
treatment for bleeding symptoms.
We previously reported our first case of liver trans- plantation (LT) for correction of severe congenital FX defi- ciency in a 17-month-old baby with recurrent hemorrhagic episodes [3]. In our previous case, the patient underwent portal vein (PV) stenting due to anastomotic stenosis one day after LT operation. We herein present the 10-year posttransplant course of the same patient with a focus on long-term maintenance of coagulation function and long- term patency of PV stenting.
Pediatric split liver transplantation for
congenital factor X deficiency: first 10-year follow-up of a case with portal vein stenting
Jung-Man Namgoong
1, Shin Hwang
1, Dae-Yeon Kim
1, Tae-Yong Ha
1, Gi-Won Song
1, Dong-Hwan Jung
1, Kyung Mo Kim
2, Seak Hee Oh
21Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
2Department of Pediatrics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Congenital factor X (FX) deficiency is a rare autosomal-recessive disease that induces bleeding disorder. Herein, we present the 10-year posttransplant course of a pediatric patient who underwent liver transplantation (LT) with portal vein (PV) stenting for cor- rection of severe congenital FX deficiency, with focus on long-term maintenance of coagulation function and patency of PV stenting. A 17-month-old infant with recurrent hemorrhagic episodes due to FX deficiency underwent split LT using a left lateral sec- tion graft. The graft-recipient weight ratio was 2.2%. The graft implantation procedures were performed by following the standard pediatric split LT procedure. Nevertheless, a wall stent was inserted due to PV anastomotic stenosis on posttransplant day 1. Graft function recovered slowly because of partial parenchyma infarct, and the patient was discharged at 46 days after LT operation. The FX activity started to increase soon after LT and gradually normalized; the coagulation profiles have been maintained well for the past 10 years. The patient has been doing well for the past 10 years after LT without any episodes of abnormal bleeding. Due to the risk of vascular complications owed to PV stenting, life-long follow-up is mandatory with special attention until attainment of com- plete physical growth to adolescent and adulthood.
Keywords: Coagulation factor; Autosomal-recessive genetic disease; Portal vein; Stent;
Split liver transplantation
Received September 4, 2020 Revised November 5, 2020 Accepted November 9, 2020 Corresponding author: Shin Hwang Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa- gu, Seoul 05505, Korea
Tel: +82-2-3010-3930 Fax: +82-2-3010-6701 E-mail: [email protected]
© The Korean Society for Transplantation This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
pISSN 2671-8790
eISSN 2671-8804
CASE REPORT
This study was approved by the Institutional Review Board of Asan Medical Center, and the re quirement for informed consent was waived.
The patient was born through a full-term normal spon- taneous vaginal delivery. At 1 month of age, generalized tonic-clonic seizure developed due to subdural hemor- rhage and abscess. She underwent craniectomy for remov- al of brain abscess, and at that time she was diagnosed with factor X (FX) deficiency. Preoperative laboratory tests revealed severe coagulation prolongation (prothrombin time, 4.2%; international normalized ratio [INR], 13.5; and activated partial thromboplastin time [aPTT], 106.4 sec- onds). The coagulation factors analysis revealed FX activ- ity as 1%, but activities of other coagulation factors were within the normal range. After treatment with craniectomy, she experienced another episode of subdural hematoma with a seizure. Thereafter, the patient also suffered from recurrent hematochezia and received a frequent transfu- sion of FFP. Prothrombin complex concentrates are not available at that time in Korea, thus we decided to perform liver transplantation (LT) at the age of 10 months.
The patient’s parents were not able to donate their liver as her mother had deceased FX activity and her fa- ther was ABO-incompatible and the size of the left lateral section was too large for this patient. The genetic study of FX showed a novel nonsense mutation, c.[310C<T] (p.[Gl- n104X]), which was inherited from her mother. The patient was enrolled at the pediatric waiting list for deceased do- nor LT.
After waiting for 7 months in the waiting list, split LT was allocated at the age of 17 months with a body weight of 11.4 kg. The donor was a 21-year-old 50 kg-weighing male. The left lateral section graft weighed 245 g; thus, the graft-recip- ient weight ratio was 2.2%. The surgical procedures were performed by following the standard pediatric split LT for left lateral segment graft implantation, which was the same as that of pediatric living donor LT. The recipient PV appeared to be normal (Fig. 1), thus the recipient PV stump was di- rectly anastomosed to the graft PV. The hepatic artery was reconstructed under surgical microscopy. The duct-to-duct anastomosis was performed for biliary reconstruction. The explant liver showed normal-looking hepatic parenchyma with occasional intracytoplasmic cholestasis (Fig. 2).
Doppler ultrasonography performed at posttransplant day 1 showed weak portal flow implicating anastomotic stenosis. Dynamic liver computed tomography revealed segmental stenosis of the PV anastomosis site and het- erogeneous low attenuation of the hepatic parenchyma (Fig. 3). Emergency laparotomy was performed and a 10 mm×40 mm-sized wall stent was inserted across the PV stenosis (Fig. 4). Follow-up computed tomography and Doppler ultrasonography showed restoration of the PV blood flow (Fig. 5). Graft function recovered slowly be- cause of partial parenchyma infarct, and the patient was discharged at 46 days after LT operation. The FX activity started to increase soon after LT and gradually normalized HIGHLIGHTS
• We present the posttransplant course of a pediatric patient who underwent split liver transplantation with portal vein stenting for correction of severe congenital factor X deficiency.
• The patient has been doing well for the past 10 years after transplantation without any episode of abnormal bleeding or vascular complication.
Fig. 1. Pretransplant computed tomography
scan showing normal looking hepatic paren- chyma (A) and perihilar vascular anatomy
A B (B).
at the time of discharge.
At 3 months after LT, she was readmitted due to Ep- stein-Barr virus hepatitis, which was uneventfully treated.
She has been undergoing Doppler ultrasonography annu- ally to check the patency of the PV stent, and it was ob- served that PV flow was patent with an intrastent diameter
of 6–8 mm (Fig. 6). She has also received liver elastogra- phy annually to check the parenchymal status due to the potential risk of PV insufficiency from significant luminal narrowing of the PV stent, in which the consistency of the liver parenchyma appeared to be not fibrotic. The patient has been doing well for the past 10 years after LT without any episodes of abnormal bleeding. The most recent coag- ulation test showed prothrombin time 77.2%, INR 1.15, and aPTT 30.8 seconds. We plan to follow up the flow of PV stent at least until full physical growth to adolescent and adulthood is achieved.
DISCUSSION
FX is a vitamin K-dependent, liver-produced serine protease that serves a pivotal role in blood coagulation as the first enzyme in the common pathway to fibrin formation [1,2].
FX deficiency is a rare autosomal recessive coagulation disorder [1]. The estimated prevalence of FX deficiency is about 1/1,500,000 or 2,000,000, therefore the condition is considered as one of the rarest coagulation disorders [4].
Fig. 2. Gross photographs of the explant liver showing normal-looking
hepatic parenchyma.
A B
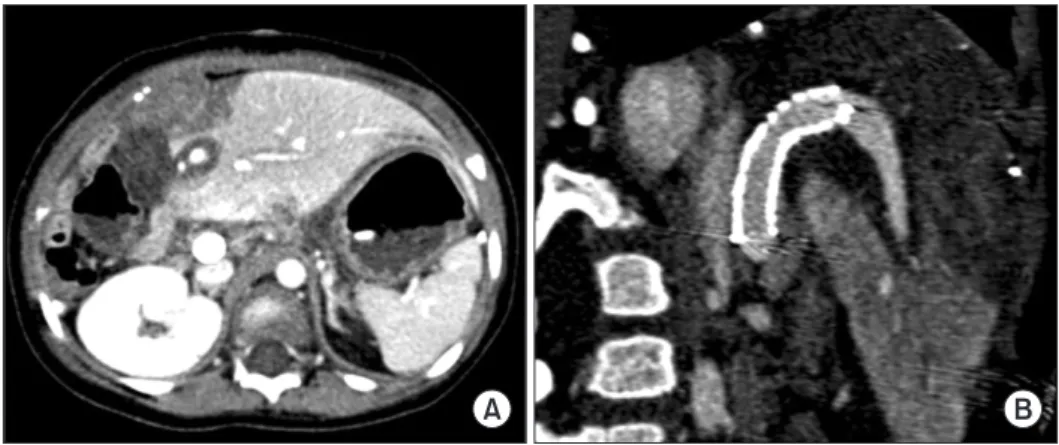
Fig. 3. Posttransplant computed tomography
scan taken at 1 day after transplantation.
Heterogeneous low attenuation of the hepat- ic parenchyma (A) and segmental stenosis of the portal vein anastomosis site (B) are identified. Arrows indicate the site of anas- tomotic stenosis.
A B C
Fig. 4. Posttransplant portal vein stenting
performed at 1 day after transplantation.
(A) A significant stenosis portal vein anas-
tomosis site is identified. (B) A 10 mm×40
mm-sized wall stent is inserted across the
stenosis. (C) The stenotic site is expanded
after stenting. Arrows indicate the site of
anastomotic stenosis.
Based on the plasma levels of FX coagulant activity measured through prothrombin time-based assay, patients have been classified into three groups: severe (FX:C, <1%), moderate (FX:C, 1%–5%), and mild (FX:C, 6%–10%). Severe clinical symptoms, such as intracranial hemorrhage, gas- trointestinal bleeding, and hemarthrosis are uncommon in patients with FX:C level of >2% [1]. Intracranial hemorrhage is the most severe complication and an important cause of death in patients with FX deficiency. Intracranial hem- orrhage usually occurs in infants between 1 and 5 months of age without any history of trauma [5]. Our patient had moderate FX deficiency (FX:C level is 1%) and experienced subdural hematoma episodes without trauma as the initial presentation and thereafter frequent development of he- matochezia was observed.
FX can be replaced with FFP or prothrombin complex concentrate, but at that time, prothrombin complex con- centrate was not available in Korea. Prothrombin complex concentrate is a medication made up of blood clotting fac- tors II, IX, and X. After LT, severe coagulation prolongation and FX activity were completely corrected in our patient.
To the best of our knowledge, there exists no other report on LT performed solely for FX deficiency in the literature probably because FX deficiency can be conservatively managed with FFP or prothrombin complex concentrate.
There was only one case of a 54-year-old man with FX de- ficiency and hepatitis C cirrhosis, who underwent LT owing to hepatic encephalopathy [6]. Currently, congenital FX de- ficiency is not regarded as an eligible indication of LT.
The LT procedures with a split left lateral section graft was successful in this patient, but early PV stenting was required due to severe stenosis of the PV anastomotic site. In pediatric LT, PV stenosis is one of the most com- mon but most critical complications. Our patient had the normal PV anatomy, unlike PV hypoplasia in pediatric
patients with biliary atresia, thus direct PV anastomosis can be regarded as the standard technique. Analysis of 1-day computed tomography and direct portography sug- gested that the underlying causes of PV stenosis were sharp narrowing at the anastomotic site per se and anas- tomotic site tension at the reconstructed PV, which were not recognized during LT operation probably due to lack of the surgeons’ experience on pediatric LT. There exists no incidence of the occurrence of this type of PV stenosis for a long time in our pediatric LT program after our adoption of funneling venoplasty and interposition of vein conduit homograft for PV reconstruction [7-9]. If there is a great discrepancy in sizes of the graft and recipient PVs or anas- tomotic site tension is anticipated, the interposition of a
A B
Fig. 5. Posttransplant computed tomography
scan taken at 2 days after transplantation.
(A) Heterogeneous low attenuation of the hepatic parenchyma was slightly improved.
(B) The configuration of the reconstructed portal vein with an internal stent implicates the presence of tension and acute angle bending at the anastomosis site before sten- ting.
Fig. 6. Follow-up Doppler ultrasonography taken at 9 years after trans-