35
통신저자:송 인 수
301-725, 대전 중구 목동 10-7번지 대전선병원 서관 2층 정형외과 의국 TEL: 042-220-8460, FAX: 042-254-4955 E-mail: [email protected]
동종 반월상 연골 이식 후 이차 관절경 소견 및 MRI를 이용한 임상적 결과
대전선병원 정형외과
전재균ㆍ송인수ㆍ김준범ㆍ정현윤ㆍ이창수
The Clinical Results Using the Second Look Arthroscopic Findings and MRI after Allogenic Meniscal Transplantation
Je-Gyun Chon, M.D., In-Soo Song, M.D., Jun-Beom Kim, M.D., Hyun-Yoon Jeong, M.D., Chang-Soo Lee, M.D.
Department of Orhopedic Surgery, Sun General Hospital Daejeon, Daejeon, Korea
Purpose: The purpose of this study was to evaluate the clinical results and the changes of allogenic meniscal transplantation by using the second look arthroscopic findings and the MRI changes after surgery.
Materials and Methods: From July 1997 to February 2007, among the patients that underwent allogenic meniscal transplantation, we chose 25 patients who underwent secondary arthroscopic evaluation. 16 of these 25 patients were men and 8 were women. Secondary arthroscopic evaluation was done without MRI in 3 cases. The mean age was 36.1 yr and the average follow up period was 28 months. Biopsy by the secondary arthroscopic evaluation was done in 2 cases. We evaluated the clinical results by the Lysholm knee scoring scale, the Knee Society Score (KSS) system and the Hospital for Special Surgery (HSS) knee score.
Results: Second-look arthroscopy after allogenic meniscal transplantation revealed that 23 cases seemed normal at the probing procedure. 5 cases showed a decreased posterior horn size. The MRI findings and secondary arthroscopic findings matched in all cases. The clinical Lysholm score improved from preoperative 65.4 points to postoperative 80.6 points, the Knee Society Score (KSS) improved from preoperative 64.6 points to postoperative 82.6 points, the functional score improved from preoperative 70.2 points to postoperative 85.6 points and the Hospital for Special Surgery (HSS) knee score improved from preoperative 66.4 points to postoperative 82.5 points (p=0.000). The function after surgery improved on all the tests and this was proved by paired t-tests.
Conclusion: Allogenic meniscal transplantation showed good results on the second look arthroscopy and the follow-up MRI and according to the clinical functional outcome. We think that confirmation through arthroscopy after follow-up MRI for the patients with clinical knee problems seems to be necessary.
Key Words: Arthroscopy, MRI, Allogenic meniscal transplantation
서 론
슬관절의 반월상 연골 손상은 최근 생활 습관의 변화,
스포츠 활동의 보편화 등으로 증가추세에 있다. 반월상 연
골은 관절연골의 영양 공급, 하중의 전달, 충격의 흡수, 슬
관절의 윤활작용, 관절 위치 감각의 담당, 슬관절의 안정
성 등의 기능을 가진다
3,6,16). 반월상 연골이 외상, 수술 등
Fig. 1. The figure shows fixation methods of meniscal transplantation: Bone-plug method.
Fig. 2. The figure shows fixation methods of meniscal transplantation: Key-hole method.
의 이유로 손실되면 체중 부하의 전이 능력 상실과 Hoop stress의 소실로 슬관절의 퇴행성 변화를 일으킨다는 것은 이미 알려진 사실이다
11,12,14). Fairbank
5)은 반월상 연골 전 절제술 후 10년 추시결과 80%의 환자에서 퇴행성 변화가 관찰됨을 보고하였고, Levy 등
15)은 반월상 연골의 전절제 술 후 회전 불안정성이 발생한다고 보고하였으며, Rangger 등
23)은 반월상 연골의 부분 또는 전절제술 후에 슬관절의 이차적인 퇴행성 관절염이 발생한다고 보고하였 다. 이에 따라 반월상 연골 손상에 대한 치료로서 반월상 연골 봉합술, 동종 반월상 연골 이식술, 자가 슬개하 지방 또는 슬개건을 이용한 이식술 및 Scaffold와 세포 배양을 이용한 반월상 연골 이식술 등의 이용이 활발하게 진행되
고 있다
18,19,24). 저자들은 동종 반월상 연골 이식술 후 자
기공명영상 결과와 이차 관절경 소견 및 임상적 결과를 통해 이식술에 대한 평가를 하고자 하였다.
대상 및 방법
저자들은 1997년 7월부터 2007년 2월까지 반월상 연골 동종 이식술을 시행한 25예의 환자를 대상으로 하였고 이 중 남자는 16명(16예), 여자는 8명(9예)이었다. 평균 연령 은 36.1세(17.0∼45.0세)였다. 내측 반월상 연골이 15예, 외측 반월상 연골이 10예였고 반월상 연골 절제술 후 동 종 반월상 연골 이식술 시행까지의 기간은 평균 5.8년(5 개월∼25.0년)이었다.
내측 반월상 연골은 경골극과 전방십자인대의 손상을
방지하기 위하여 전후방 골편(bone plugs)을 이용한 고정
을 사용하였고(Fig. 1), 외측 반월상 연골은 열쇠 구멍
(key hole) 수기를 사용하였다(Fig. 2). 연골의 전각부는
outside-in 술식, 후각부는 all-inside 술식, 체부는 in-
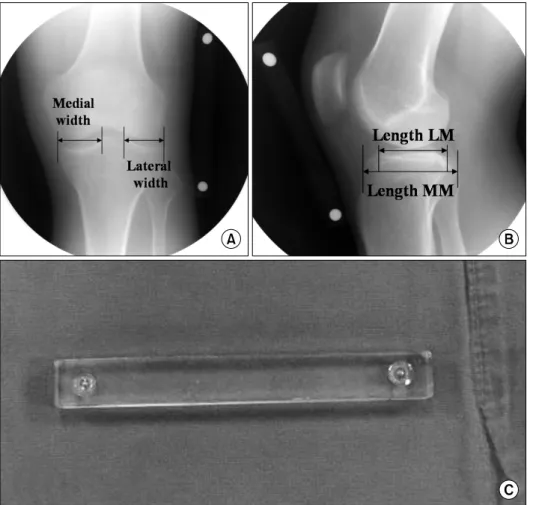
Fig. 3. Preoperative sizing of meniscal allografts. (A) The true AP radiograph was used to measure meniscus width.
Width is measured by obs- taining the distance from the most medial or lateral aspect of the tibia at the level of the plateau to its respective inter- condylar eminence peak. (B) The true lateral radiograph was used to measure meniscus length. Length is measured by obstaining the AP distance from the anterior-most insertion of the lateral or medial meni- scus to the posterior most in- sertion. (C) This figure shows magnification marker that con- sists of two ball bearings em- bedded 10 cm apart in plastic.
side-out 술식과 outside-in 술식의 혼합 방법을 이용하였다.
일차적으로 반월상 연골 절제술을 시행한 원인은 스포 츠 손상이 11예, 원판형 연골판이 7예, 작업 중 손상이 4 예, 추락 손상 1예, 넘어지며 수상한 경우가 1예, 원인을 알 수 없는 경우가 1예였다. 동반된 손상으로는 전방 십자 인대 손상이 7예, 연골손상이 5예, 후방 십자인대 손상이 3예, 퇴행성 관절염이 3예였다.
동종 반월상 연골 이식술의 적응은 50세 이하의 비교적 젊은 연령의 환자, 반월상 연골 아전절제술 혹은 전절제술 시행 받고 증상이 지속된 환자, 내, 외측 반월상 연골 중 한 측의 손상, 방사선 소견상 1 또는 2등급의 관절 연골 퇴행성 변화가 있는 환자 중 하지정렬이 정상범위 내에 있는 환자를 대상으로 하였고
9,25), 전례에서 신선 냉동 보 존(fresh-frozen type) 동종 연골을 사용하였고, 이식물은 측정치보다 약간 큰 이식물을 선택하였다.
반월상 연골의 크기 측정 위해 우선 10 cm 간격으로 놓 인 두 개의 볼(ball bearing)로 구성된 길다란 플라스틱의
확대 표시기(magnification marker)(Fig. 3C)를 대상자의 환측 슬관절에 부착한 후 슬관절의 정 전후면 사진과 측 면 사진을 촬영하였다. PACS (picture archiving and communication system)를 이용하여 방사선 사진에서 보 이는 두 개의 볼 간격이 10 cm가 되도록 확대한 후 연골 크기를 측정하였다. 정 전후면 사진상을 통해 너비(width) 로 측정하고, 이는 경골 고평부(tibial plateau)의 내측 또 는 외측 경계면에서 각각의 내측 또는 외측 과간극까지의 거리로 하였다. 측면 사진상에서는 길이(length)를 측정하 였는데, 외측 또는 내측 연골의 가장 앞쪽 부착 부위에서 각각의 가장 뒤쪽 부착 부위까지의 전후 거리로 하였다
26)(Fig. 3A, B). 환측 연골 크기를 단순 방사선 사진을 통해 술 전과 술 후 모두 측정하여 변화를 관찰하였다(Table 1, 2).
또한 술 후 추시 자기 공명 영상과 이차 관절경 검사상 반 월상 연골 이식물의 변화를 관찰하였다.
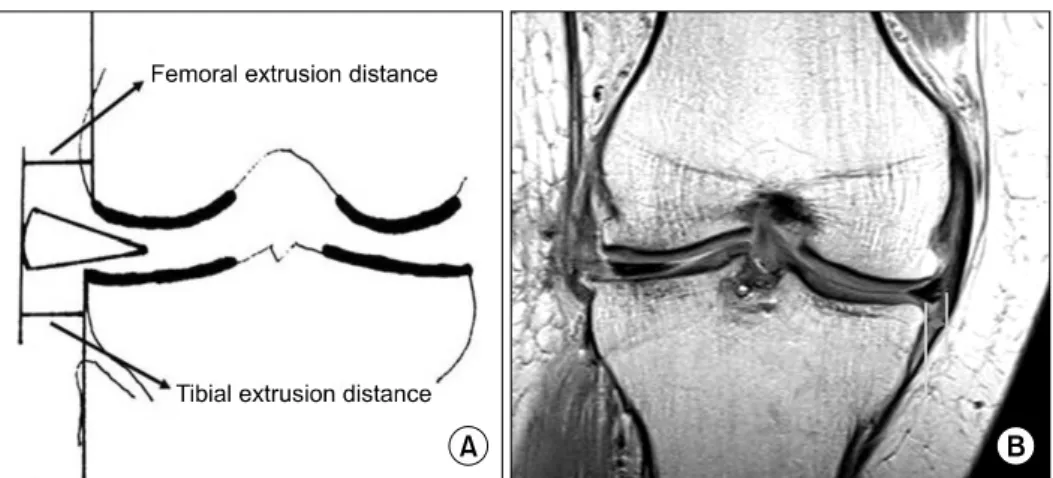
이식 반월상 연골의 변연부 아탈구(subluxation)는 경골
고평부의 변연 경계면에서 연골의 바깥쪽 경계면(outer
Fig. 4. Meniscus extrusion in the MRI study was assessed on coronal sections by drawing a line perpendicular to a horizontal line connecting both distal surfaces of the femoral condyles, and touching the outer edge of the articular cartilage of the femoral condyle, the tibial plateau and meniscal outer edge. Extrusion was defined as the distance from the femoral condyle or tibial plateau to the outer edge of the meniscus (described by Verdonk et al.). We was assessed the distance from the tibial plateau to meniscal outer edge (A: schematic, B: MRI).
Table 1. Preoperative Meniscal Size AP (mm)
Transverse (mm) Ant. Mid. Post.
Male Female
Lat.
Med.
Lat.
Med.
33.2 41.5 30.5 37.2
6.2 6.6 5.2 5.5
7.5 10.2 6.8 10.0
12.8 13.7 12.1 12.6
Table 2. Postoperative Meniscal Size (average 28.0 months) AP (mm)
Transverse (mm) Ant. Mid. Post.
Male Female
Lat.
Med.
Lat.
Med.
31.2 40.1 29.6 36.7
5.8 6.2 4.9 5.1
6.8 9.9 5.8 9.6
11.8 13.1 10.6 11.5
edge of the meniscus)까지의 거리로 정의하였고
7), 3 mm 이상 아탈구 된 경우를 변연 탈구(extrusion)로 정의하였 다
4). 측정방법은 Verdonk 등
31)이 제시한 방법을 이용하 였다(Fig. 4).
첫 이식술 후 재활 치료는 첫 4주는 목발 착용한 상태에 서 20%의 체중부하만 허용하고, CPM (지속성 수동적 운
동)을 하였다. 4∼6주가 지나면 앉아서 하는 일을 할 수 있게 하고 보조기를 제거하였다. 8주 이후에는 자전거 타 기, 대퇴 사두근 강화 운동을 추가했으며, 3개월 후부터는 환자가 목발이나 보행기 없이 걸을 수 있도록 단계적으로 허용하였다.
임상적 평가와 기능적 평가는 Lysholm score, Knee so- ciety knee score (KSS) system, The hospital for special surgery (HSS) knee score를 이용하였고
1,10,30), 술 후 평균 28개월에 25예 중 22예는 이차 관절경 검사와 자기 공명 영상 촬영을 모두 시행하였고, 3예는 이차 관절경 검사만 시행하였다.
결 과 1. 이학적 및 기능적 평가
술 후 1예에서 관절내 삼출과 관절면의 압통소견이 보
였고, 전방십자인대 손상, 후방십자인대 손상이 있는 10예
에서 십자인대 재건술을 시행하였고 전례에서 슬관절의
불안정성이 소실되었다. Lysholm score 평가 지수는 술
전 65.4점에서 술 후 80.6점, KSS system에서는 슬관절
점수가 64.6점에서 82.6점, 기능적 점수가 70.2점에서
85.6점, HSS knee score에서는 66.4점에서 82.5점으로 향
상되었다(Table 3). 기능적 평가의 향상은 paired t-test상
에서 통계학적 유의성을 보였다(p=0.000).
Table 3. Preoperative Meniscal Size
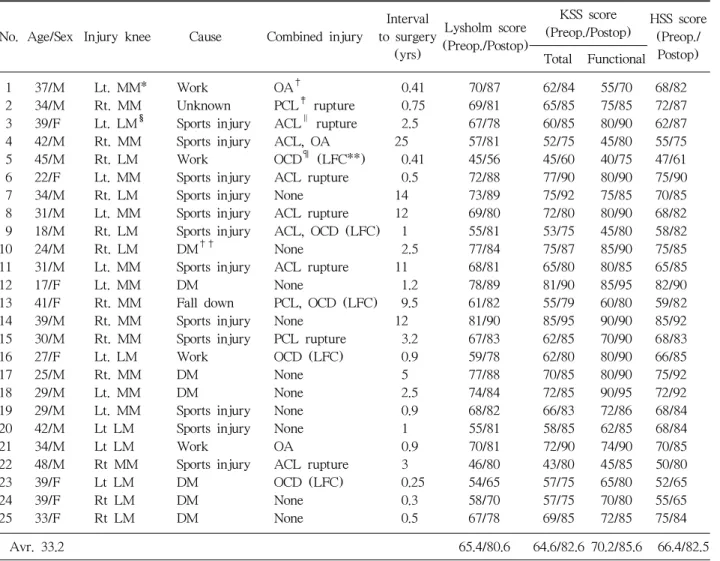
No. Age/Sex Injury knee Cause Combined injury
Interval to surgery (yrs)
Lysholm score (Preop./Postop)
KSS score
(Preop./Postop) HSS score (Preop./
Postop) Total Functional
1 37/M Lt. MM* Work OA† 0.41 70/87 62/84 55/70 68/82
2 34/M Rt. MM Unknown PCL‡ rupture 0.75 69/81 65/85 75/85 72/87 3 39/F Lt. LM§ Sports injury ACL∥ rupture 2.5 67/78 60/85 80/90 62/87
4 42/M Rt. MM Sports injury ACL, OA 25 57/81 52/75 45/80 55/75
5 45/M Rt. LM Work OCD¶ (LFC**) 0.41 45/56 45/60 40/75 47/61
6 22/F Lt. MM Sports injury ACL rupture 0.5 72/88 77/90 80/90 75/90
7 34/M Rt. LM Sports injury None 14 73/89 75/92 75/85 70/85
8 31/M Lt. MM Sports injury ACL rupture 12 69/80 72/80 80/90 68/82 9 18/M Rt. LM Sports injury ACL, OCD (LFC) 1 55/81 53/75 45/80 58/82
10 24/M Rt. LM DM†† None 2.5 77/84 75/87 85/90 75/85
11 31/M Lt. MM Sports injury ACL rupture 11 68/81 65/80 80/85 65/85
12 17/F Lt. MM DM None 1.2 78/89 81/90 85/95 82/90
13 41/F Rt. MM Fall down PCL, OCD (LFC) 9.5 61/82 55/79 60/80 59/82
14 39/M Rt. MM Sports injury None 12 81/90 85/95 90/90 85/92
15 30/M Rt. MM Sports injury PCL rupture 3.2 67/83 62/85 70/90 68/83
16 27/F Lt. LM Work OCD (LFC) 0.9 59/78 62/80 80/90 66/85
17 25/M Rt. MM DM None 5 77/88 70/85 80/90 75/92
18 29/M Lt. MM DM None 2.5 74/84 72/85 90/95 72/92
19 29/M Lt. MM Sports injury None 0.9 68/82 66/83 72/86 68/84 20 42/M Lt LM Sports injury None 1 55/81 58/85 62/85 68/84
21 34/M Lt LM Work OA 0.9 70/81 72/90 74/90 70/85
22 48/M Rt MM Sports injury ACL rupture 3 46/80 43/80 45/85 50/80 23 39/F Lt LM DM OCD (LFC) 0.25 54/65 57/75 65/80 52/65 24 39/F Rt LM DM None 0.3 58/70 57/75 70/80 55/65 25 33/F Rt LM DM None 0.5 67/78 69/85 72/85 75/84
Avr. 33.2 65.4/80.6 64.6/82.6 70.2/85.6 66.4/82.5
*MM: medial meniscus, †OA: osteo arthritis, ‡PCL: posterior cruciate ligament, §LM: lateral meniscus, ∥ACL: anterior cruciate ligament, ¶OCD: osteochondral defect, **LFC: lateral femoral condyle, ††DM: discoid meniscus
2. 방사선적 소견
전례에서 슬관절 직립 전후방 사진과 45도 슬관절 굴곡 후전방 사진 및 단순 측방 사진을 촬영하였고, 술 후 평균 5.3개월 후에 자기공명영상을 촬영하였다. 반월상 연골의 크기는 술 전과 술 후를 비교하였을 때 남자에서 내측 반 월상 연골의 전후방 길이는 수술 전 평균 41.5 mm에서 수술 후 평균 40.1 mm로 1.4 mm, 전각부는 수술 전 평균 6.6 mm에서 수술 후 평균 6.2 mm로 0.4 mm, 후각부는 수술 전 평균 13.7 mm에서 수술 후 평균 13.1 mm로 0.6 mm 감소된 결과를 보였고, 외측 반월상 연골의 전후방 길이는 수술 전 평균 33.2 mm에서 수술 후 평균 31.2 mm로 2.0 mm, 전각부는 수술 전 평균 6.2 mm에서 수술
후 평균 5.8 mm로 0.4 mm, 후각부는 수술 전 평균 12.8
mm에서 수술 후 평균 11.8 mm로 1.0 mm 감소된 결과를
보였고, 여자에서는 내측 반월상 연골의 전후방 길이는 수
술 전 평균 37.2 mm에서 수술 후 평균 36.7 mm로 0.5
mm, 전각부는 수술 전 평균 5.5 mm에서 수술 후 평균
5.1 mm로 0.4 mm, 후각부는 수술 전 평균 12.6 mm에서
수술 후 평균 11.5 mm로 1.1 mm로 감소하였고, 외측 반
월상 연골의 전후방 길이는 수술 전 평균 30.5 mm에서
수술 후 평균 29.6 mm로 0.9 mm, 전각부는 수술 전 평균
5.2 mm에서 수술 후 평균 4.9 mm로 0.3 mm, 후각부는
수술 전 평균 12.1 mm에서 수술 후 평균 10.5 mm로 1.6
mm 감소된 결과를 보였다(Table 2). 7예에서 관절 간격
의 협소화가 있었다.
Fig. 5. Follow up MRI after meniscal transplantation: It demonstrate increased signal intensity in peripheral regions on posterior horn (arrow).
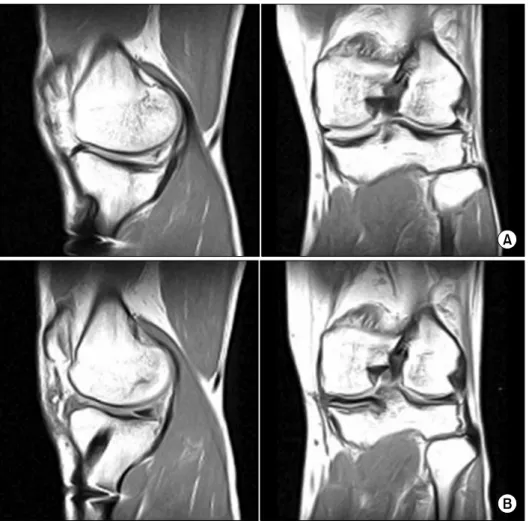
Fig. 6. Preoperative and Pos- toperative MRI: coronal MRI image shows normal meniscal position. (A) Before meniscal transplantation MRI: MM total meniscectomy & ACL recon- struction state. (B) After meniscal transplantation MRI:
using Bone-plug method.
3. 자기 공명 영상 촬영 및 관절경 소견
자기 공명 영상 촬영상 9예에서 이식 반월상 연골 변연 부, 전, 후각 모두에서 신호 강도의 증가 소견이 보였고 (Fig. 5), 최종 자기공명영상에서 5예에서 이식된 반월상 연골의 봉합사로 관절막에 부착된 중간부위에서는 이식한 반월상 연골 측면부의 아탈구 소견이 보였으나, 이식골에 부착된 전각부, 후각부에서는 관찰되지 않았다. 관상면상 이식된 연골이 변연부에서 잘 고정되어 있었고, 비해부학 적 위치에서의 골교 고정(bone bridge fixation) 소견은 관찰되지 않았다(Fig. 6).
술 후 2차 관절경 검사는 평균 28개월에 25예에서 시행
하였다. 1예를 제외한 24예(96%)에서 관절막에 봉합된
연골부의 완전 치유 소견과 양호한 혈관 분포 소견을 보
였고(Fig. 7), 18예(72%)에서 위축 소견 없었다. 7예
(28%)에서 외측 반월상 연골 이식부의 후각부에서 이식
된 반월상 연골의 위축 소견이 관찰되었고, 모두 자기 공
Fig. 7. Second look arthroscopic finding at 7 months after meniscal transplantation: it shows complete healing with firm attachment around the entire circumference of the meniscal rim and no shirinking meniscal size.
명 영상 촬영상 증가된 신호 강도 소견을 보였던 예이다.
봉합사 파열로 고정되지 않은 1예에서 재봉합을 시행하였 다. 동종 이식 반월상 연골의 파열이나 퇴행성 변화는 관 찰되지 않았다.
고 찰
슬관절내 반월상 연골은 간엽 조직(mesenchyme)에서 분화하여 섬유성 콜라겐 그물망과 proteoglycan gel로 구 성된 섬유 연골 세포로 형성된다
3,17,22,33). 그러나 아전절제 술 및 전절제술 후 반월상 연골의 재생은 활액막 세포에 서 분화되는 섬유 조직으로 이루어져 기능 수행에 장애를 일으킨다
28). 따라서, 현재 반월상 연골의 손상에 대한 치 료는 봉합술, 부분 절제술 등의 연골을 보전할 수 있는 술 기가 보편화되어 있다. 하지만 반월상 연골을 보전하기 힘 든 경우 반월상 연골의 동종 이식술은 대안이 될 수 있다.
반월상 연골 동종 이식술의 성공을 위해서는 적당한 크기 의 이식물을 정확한 해부학적 위치에 고정하는 것이 중요 하다. Chen 등
2)은 pressure-sensitive film을 이용하여 하 중분산(load distribution) 실험에서 안정적인 반월상 연골 이식의 골 부착 또는 전, 후각을 단단히 고정한 경우는 정 상 관절과 같은 접촉 면적과 최대 접촉 압력을 가지며, 반 월상 연골의 전, 후각 중 한곳만 고정한 경우는 정상 반월
상 연골과 반월상 연골 전절제술의 중간 결과를 보이고, 고정하지 않은 경우는 반월상 연골 전절제술과 같은 결과 를 보인다고 보고하였다. 따라서 연부조직 고정 방법이나, 골조각 고정 방법은 반월상 연골 고유의 hoop tension을 유지할 수 없어 하중 분산의 정상 기능을 하지 못하는 것 으로 보고하였다. 반월상 연골의 이식술은 변연부를 봉합 하는 연부조직 고정방법(soft tissue fixation), 전후각에 원통 모양의 골조각을 붙여 경골 구멍에 고정하는 골편 고정법(bone plug fixation), 그리고 전후각을 골교(bone bridge)로 연결하여 경골의 도랑에 고정하는 골교 고정법 (bone bridge fixation), 반월상 연골과 경골의 부착부위를 포함하여 좁은 경골편을 경골 홈에 끼워 고정하는 열쇠 구멍 수기(key hole method) 등의 방법이 있다
8,20,27,29). 저자들은 내측 반월상 연골 이식 전례에서 골편 고정법 (bone plug fixation)을 사용하여 경골극과 전방십자인대 기시부의 손상을 방지하였으며, 또한 전방십자인대 재건 술을 시행한 7예에서는 관절 내에서부터 경골하부 방향으로 경골 터널을 위한 유도기를 이용하여 관절선에서 10 mm 홈을 만들어 전방십자인대 재건을 위한 홈과의 간섭을 방 지하고, 불필요한 긴 홈으로 인한 골 소실을 최소화 하였 다. 외측 반월상 연골 이식 전례에서 열쇠구멍 수기(key hole method)를 이용하여 술기를 단순화시켰다. 반월상 연골의 보존 방법 역시 다양하여 신선(fresh), 신선-냉동 (fresh-frozen), 심냉동(deep-frozen), 냉동 건조(freeze- dried) 및 초냉동(cryo-preserved) 등이 있다
8). 저자들은 전례에서 신선-냉동 연골을 사용하였는데 이는 기술적으 로 간단하며, 저비용의 장점이 있으나, 냉동으로 이식 연 골의 크기가 변화할 수 있으며 보존 시 탈수와 해빙 과정 에서 조직 파괴가 될 수 있다는 단점이 있다
27). 저자들이 관절경으로 추시 관찰한 25예 중 7예에서 이식된 반월상 연골의 위축 소견이 관찰되었다. 이식된 반월상 연골의 위 축은 내측보다는 외측 반월상 연골에서, 전각부보다는 후 각부의 위축이 두드러졌으며, 그 이유는 내측 및 외측 반 월상 연골의 해부학적 형태의 차이와 반월상 연골의 후각 부 파열 시 All- inside 봉합기술이나 봉합기구를 사용하 여 봉합을 시행하고, 전방 및 측방 부위 봉합을 한 후 후 각부를 봉합할 때 연골이 전방 및 측방부위로 전위가 되 고 이를 보상하기 위해서 불가피하게 더 긴장된 봉합이 이루어져 외측 후각부에서 위축이 심한 것으로 생각된다.
따라서, 후각부를 먼저 봉합함으로써 후각부의 긴장된 봉
합을 최소화하고, 측정된 이식 연골보다는 약간 큰 이식물 을 선택함으로써 봉합으로 인한 긴장을 최소화하려고 노 력하였다.
일부 연구에서는 반월상 연골 이식술 후 약 30∼40%의 반월상 연골 아탈구를 보고하고 있으며 본 연구에서는 5 예(20%)에서 추시 자기공명영상에서 이식된 반월상 연골 측면부의 아탈구 소견이 관찰되었다. 이는 저자들이 강한 봉합(tension suture)을 피하고 술 전 단순 방사선 사진상 의 주형(template) 크기보다 약간 큰 이식물을 삽입함으 로써 나타난 결과라고 생각된다.
이식된 동종 반월상 연골의 술 후의 자기공명영상의 신 호 강도는 술 후 초기에는 정상측과 구별할 수 없는 저신 호 강도였다가 시간이 지남에 따라 반월상 연골의 변연부 에서 신호강도가 증가하여 술 후 6주에 고강도의 신호 강 도를 보이며 시간이 경과함에 따라 다시 신호강도가 감소
한다
13,21). 저자들은 술 후 평균 28개월에 자기공명영상을
추시한 결과 9예에서 증가된 신호 강도가 관찰되었다. 신 호강도의 증가는 신생 혈관의 증식(neovascularization), 연골 점액성 변성(chondromucoid degeneration) 등에 의 한 것으로 판단된다
32).
총 25예 중 1예에서 관찰된 후각부 봉합사의 파열은 술 후 환자의 조기 과활동으로 사료되며 재봉합 후 증상은 소실되었지만, 조기 과운동 및 회전 운동을 삼가고 최소 6 주 이상 보호를 함으로써 좋은 결과를 얻을 수 있을 것으 로 생각된다.
술 전 시행한 슬관절 직립 전후방 사진과 45도 슬관절 굴곡 후전방 사진에서 대퇴 경골간 관절 간격이 16예에서 는 정상 7예에서는 관절 간격의 협소화가 있었다. 추시 상 이식된 반월상 연골의 크기 및 관절 간격의 변화를 측정 하였으며 최종 추시상 술 전 관절 간격이 정상인 군에서 보다 술 전 관절 간격의 협소화를 보인 7예에서 더욱 심 한 연골 위축 소견을 보였다. 그러나 대상 환자수가 적고 추시 기간이 짧아 더욱 적극적인 연구가 필요할 것으로 생각된다.
결 론
반월상 연골 이식술은 연골 손상 후 나타나는 퇴행성 변화를 최소화하고 젊고 활동적인 환자에게 유용한 시술 이나 이식 연골의 위축, 변연부 아탈구, 관절 간격의 협소
화, 봉합사의 파열 등을 관찰할 수 있었다. 이식 후 임상 적 문제를 가진 환자의 경우 단순 방사선상의 관절 간격 협소화 및 추적 MRI상의 신호 강도 변화 등을 주의 깊게 관찰하고, 이후 이차 관절경술을 통해 정확한 평가가 이루 어져야 한다고 생각된다.
REFERENCES
1. Binazzi R, Soundry M, Mestriner LA, Insall JN:
Knee arthroplasty rating. J Arthroplasty, 7: 145-148, 1992.
2. Chen MI, Branch TP, Hutton WC: Is it important to secure the horns during lateral meniscal transplantation? A cadeveric study. Arthroscopy, 12:
174-181, 1996.
3. Clark CR, Ogden JA: Development of the menisci of the human knee joint. Mophological changes and their potential role in childhood meniscal injury. J Bone Joint Surg Am, 65: 538-547, 1983.
4. Costa Cr, Morrison WB, Carrino JA: Medial meniscus extrusion on knee MRI: is extent associated with severity of degeneration or type of tear? AJR Am J Roentgenol, 183: 17-23, 2004.
5. Fairbank TJ: Knee joint changes after meniscectomy.
J Bone Joint Surg Am, 30: 664-670, 1948.
6. Fukubayashi T, Kurosawa H: The contact area and pressure distribution pattern of the knee. A study of normal and osteoarthritis knee joints. Acta Orthop Scand, 51: 871-879, 1980.
7. Gale DR, Chaisson CE, Totterman SM, Schwartz RK, Gale ME, Felson D: Meniscal subluxation:
association with osteoarthritis and joint space narrowing. Osteoarthritis Cartilage, 7: 526-532, 1999.
8. Goble EM, Kane SM: Meniscal allograft transp- lantation. In: James CY chow ed. Advanced arthro- scopy. 1st ed. New York, Springer Inc: 367-380, 2001.
9. Henning CE, Lynch MA: Current concepts of meniscal function and pathology. Clin Sports Med, 4:
259-265, 1985.
10. Insall JN, Dorr LD, Scott RD, Scott WN: Rationale of the knee society clinical rating system. Clin Orthop Relat Res, 248: 13-14, 1989.
11. Johnson RJ, Kettlekamp DB, Clark W, Leaverton P:
Factors affecting late results after meniscectomy. J Bone Joint Surg Am, 56: 719-729, 1974.
12. Jørgensen U, Sonne-Holm S, Lauridsen F, Rosenklint A: Long term follow-up of menisectomy in athletes. A prospective longitudinal study. J Bone Joint Surg Br, 69: 80-83, 1987.
13. Kuhn JE, Wojtys EM: Allograft meniscus transplan- tation. Clin Sports Med, 15: 536-537, 1996.
14. Kurosawa H, Fukubayashi T, Nakajima H:
Load-bearing mode of the knee joint: physical behavior of the knee joint with or without the menisci. Clin Orthop Relat Res, 149: 283-290, 1980.
15. Levy IM, Torzilli PA, Warren RF: The effect of medial meniscectomy on anteior-posterior motion of the knee. J Bone Joint Surg Am, 64: 883-888, 1982.
16. Lysholm J, Hamberg P, Gilquist J: The correlation between osteoarthrosis as seen on radiographs and on arthroscopy. Arthroscopy, 3: 161-165, 1987.
17. McDevitt CA, Wabber RJ: The ultrastructure and biochemistry of meniscal cartilage. Clin Orthop Relat Res, 252: 8-18, 1990.
18. Mikic ZD, Brankov MZ, Tubic MV, Lazetic AB:
Allograft meniscus transplantation in the dog. Acta Orthop Scand, 64: 329-332, 1993.
19. Milachowski KA, Weismerir K, Wirth CJ:
Homologous meniscus transplantation. Experimental and clinical results. Int Orthop, 13: 1-11, 1989.
20. Min BH, Kim HS, Jang DW, Kang SY: Technical note of meniscal allograft transplantation using minimal incision. J Korean Arthroscopy Soc, 3: 54-61, 1999.
21. Patten RM, Rolfe BA: MRI of meniscal allografts. J Comput Assisttomogr, 19: 243-246, 1995.
22. Peters TJ, Smillie IS: Studies on the chemical composition of the menisci of the knee joint with special reference to the horizontal cleavage lesion. Clin Orthop Relat Res, 86: 245-252, 1972.
23. Rangger C, Klestil T, Gloetzer W, Kennleer G, Benedetto KP: Osteoarthritis after arthroscopic partial meniscectomy. Am J Sports Med, 23: 240-244, 1995.
24. Rath E, Richmond JC, Yassir W, Albright JD, Gundogan F: Meniscal allograft transplantation.
Two-to eight-year results. Am J Sports Med, 29:
410-414, 2001.
25. Rodeo SA: Meniscal allografts-where do we stand?
Am J Sports Med, 29: 246-261, 2001.
26. Shaffer B, Kennedy S, Klimkiewicz J, Yao L:
Preoperative sizing of meniscal allografts in meniscus transplantation. Am J Sports Med, 28: 524-533, 2000.
27. Shelton WR, Dukes AD: Meniscus replacement with bone anchors: a surgical technique. Arthroscopy, 10:
324-327, 1994.
28. Smillie IS: Observation on the regeneration of the semilunar cartilage in man. Br J Surg, 31: 398-401, 1944.
29. Stone KR, Rosenberg T: Surgical technique of meniscal replacement. Arthroscopy, 9: 234-237, 1993.
30. Tegner Y, Lysholm J: Rating system in the evaluation of knee ligament injuries. Clin Orthop Relat Res, 198:
43-49, 1985.
31. Verdonk P, Depaepe Y, Desmyter S, et al: Normal and transplanted lateral knee menisci: evaluation of extrusion using magnetic resonance imaging and ultrasound. Knee Surg Sports Traumatol Arthrosc, 12:
411-419, 2004.
32. Verstraete KL, Verdonk R, Verstraete P, De Rooy J, Kunnen M: Current status and imaging of allogarft meniscal transplantation. Eur J Radiol, 26: 16-22, 1997.
33. Yasui K: Three dimensional architecture of normal human menisci. JJph OrthopAssoc, 52: 391-399, 1978.
= 국문초록 =
목적: 동종 반월상 연골 이식술 후 이차 관절경 소견 및 자기공명영상을 통해 이식물의 변화를 관찰하고
그 임상적 결과를 보고하고자 하였다.
대상 및 방법: 1997년 7월부터 2007년 2월까지 동종 반월상 연골 이식술을 시행 받은 환자에서 이차 관절 경 검사와 자기공명영상 추시가 가능하였던 25 예를 대상으로 하였다. 이 중 남자는 16명, 여자는 8명이 었다. 3예는 자기공명영상 추시 없이 이차 관절경 검사만 시행하였다. 평균 연령은 36.1세, 평균 추시기간 은 28.0개월(6.0개월∼7.0년)이었다. 이차 관절경 검사 시 2예에서는 조직검사를 시행하였다. 환자의 기 능적 평가는 Lysholm score, Knee society score (KSS) system, The hospital for special surgery (HSS) knee score를 이용하였다.
결과: 이차 관절경 검사상 25예 중 23예에서 이식물이 변연부와 완전한 치유소견을 보였다. 25예 중 5예 에서 후각부의 크기가 감소되어 있었다. 자기공명영상에서는 전 예에서 이차 관절경 검사와 일치된 소견 을 보였다. Lysholm score는 술 전 평균 65.4점에서 술 후 평균 80.6점, Knee society score (KSS) system 에서는 슬관절 점수가 평균 64.6점에서 평균 82.6점, 기능적 점수가 평균 70.2점에서 평균 85.6점, The hospital for special surgery (HSS) knee score에서는 평균 66.4점에서 평균 82.5점으로 향상되었다. 모든 기능 테스트에서 수술 후에 기능이 향상되었고, 이는 paired t-test로 평가되었다(p=0.000).
결론: 동종 반월상 연골 이식술은 이식된 연골이 주변조직과 함께 완전히 치유되었고 임상적으로도 호전
되어 반월상 연골 결손환자의 치료에 유용한 방법이라고 생각되고, 임상적으로 문제가 있는 환자의 평가 에 있어서는 MRI 검사 후 관절경술을 통한 확인이 필요하다고 생각된다.
색인 단어: 관절경 검사, 자기 공명 영상, 동종 반월상 연골 이식