30
서 론
2000년에 들어 우리나라도 65세 이상의 인구가 7%를 넘 어서는 고령화 사회로 접어들었으며, 동시에 평균수명도 76세를 넘어가고 있고, 특히 여자의 경우 이미 평균수명이 80세를 넘어섰다.(1) 이런 현실에서 80세 이상의 위암환자 를 임상에서 만나는 것은 더 이상 어려운 일이 아니다. 전체 적인 위암환자가 줄고 있는 이웃나라 일본에서도 고령층의 위암환자는 계속 늘고 있다. 고령의 위암환자에게 적절한 치료전략 및 수술 범위를 제안하기 위한 많은 연구들이 진 행되었으나, 지금까지의 연구는 주로 70세 이상을 대상으 로 하였거나, 다른 연령층과의 임상병리학적 특성의 비교, 그리고 수술의 안정성에 대한 연구가 대부분이었다.(2-19) 하지만 이 연령층의 주된 사망원인이 심장질환이나 뇌혈관 질환임을 고려할 때, 자연경과를 이해하고 수술 후 사망원 인을 분석하는 일이 이들 연령층의 치료 및 수술계획을 세 워나가는 데 중요하다고 판단하였다. 이에 저자들은 근치 적 위절제가 시행된 고령의 위암환자들의 자연경과 및 사 망원인을 분석함으로써 적절한 치료계획을 제시하고자 본 연구를 고안하였다.
방 법
서울 아산병원 외과에서 1990년 1월부터 2002년 2월까지 만 12년간 근치적 위절제술을 시행 받은 위암환자 중, 수술 당시 80세 이상이었던 총 44명을 대상으로 하였다. 이들 중 추적이 불가능하였던 3예를 제외한 41명을 대상으로 전화 연락과 외래추적을 통해 사망원인을 분석하였다. 연구 종 료 시점은 2004년 2월 29일로 정하였다.
재발 확인은 추적검사 상 가장 먼저 나타난 장소를 표기 하였고, 이를 근거로 위암관련 사망으로 정의하였다. 노쇠 (senility)로 사망원인을 표기한 경우는, 다른 원인에 의한 사
사망원인의 분석을 근거로 한 80세 이상 위암환자의 치료전략
울산대학교 의과대학 외과학교실 서울아산병원 외과 김용진․오성태․최원용․임정택․육정환․김병식
Treatment Strategy of Gastric Cancer in Pa- tients Older than 80 Years of Age
Yong Jin Kim, M.D., Sung Tae Oh, M.D., Won Yong Choi, M.D., Jung Taek Lim, M.D., Jung Hwan Yook, M.D. and Byung Sik Kim, M.D.
Purpose: The geriatric population will continue to increase in the coming decades, and the number of gastric cancer patients who are over 80 years of age is increasing. The aim of this study was to suggest optimal treatment in these patients on the basis of the cause of death.
Methods: Forty-four patients who underwent curative resec- tion in the course of gastric cancer treatment and were over 80 years of age at Asan Medical Center between January 1990 and February 2002 were included in this study. The cause of death of those patients was retrospectively ana- lyzed by checking medical record or calling to relatives.
Results: Average age of 41 patients was 81.41 years old and follow up duration was 49 months. Until February 2004, overall mortality was 23 patients (56%). The mortality from gastric cancer-related and from other disease was 12 pa- tients (52%) & 11 patients (48%), respectively. The most common cause of death from other disease was senility.
Median survival time of 11 patients from cancer none-related death was 57 months. Median survival time of 32 patients corresponding stage I & II was 52.5 months.
Conclusion: We, therefore, conclude that a standard gas- trectomy is basically appropriate for patients older than 80 years of age, as long as they demonstrate a good risk. (J Korean Surg Soc 2005;68:30-34)
Key Words: Gastric cancer, The elderly, Cause of death, Gastrectomy
중심 단어: 위암, 고령, 사망원인, 위절제술
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Department of Surgery, University of Ulsan College of Medicine and Asan Medical Center, Seoul, Korea
책임저자:오성태, 서울시 송파구 풍납동 388-1 ꂕ 138-736, 서울아산병원 외과 Tel: 02-3010-3508, Fax: 02-474-9027 E-mail: [email protected]
접수일:2004년 6월 7일, 게재승인일:2004년 10월 22일 본 논문의 요지는 2004년 대한외과학회 춘계학술대회에서 포스터 구연되었음.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 망을 명백히 증명할 수 없으면서, 추적 검사 상 재발의 증거 가 없는 경우로 하였으며, 이는 가족들의 증언과 통계청에 등록된 사인을 근거로 하였다.
결 과
1) 임상적 특징
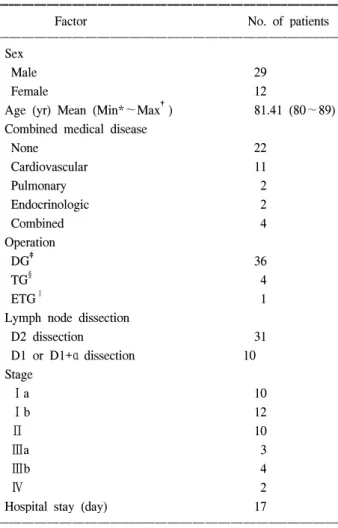
환자의 평균연령은 81.41세(최소 80세, 최대 89세)였으며, 남자 29명, 여자 12명이었다. 평균 추적기간은 49개월이었 으며, 생존환자의 추적기간은 64개월이었다. 수술 방법은 36명의 환자에서 하부위절제가, 4명의 환자에서 위 전절제 가, 그리고 1명의 환자에서는 확대 위 전절제가 시행되었으 며, 31명의 환자에서 D2 이상의 림프절곽청술이 이루어졌 다. 1예에서 동반된 복부 대동맥류를 함께 절제했으며, 4예 에서 담낭절제술이 이루어졌다. 수술 당시 11명에서 고혈 Table 1. Clinicopathologic characteristics
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Factor No. of patients
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Sex
Male 29
Female 12
Age (yr) Mean (Min*∼Max†) 81.41 (80∼89) Combined medical disease
None 22
Cardiovascular 11
Pulmonary 2
Endocrinologic 2
Combined 4
Operation
DG‡ 36
TG§ 4
ETG∥ 1
Lymph node dissection
D2 dissection 31
D1 or D1+α dissection 10
Stage
Ⅰa 10
Ⅰb 12
Ⅱ 10
Ⅲa 3
Ⅲb 4
Ⅳ 2
Hospital stay (day) 17
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*MIN = minimum age; †MAX = maximum age; ‡DG = distal gastrectomy; §TG = total gastrectomy; ∥ETC = extended total gas- trectomy.
Table 3. Clinical features and postoperative course of gastric cancer-related death
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Survival time
No. Age Sex Operation date Operation name TNM Cause of death
(Mon) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
1 81 M 1996-07-25 DG T1N0M0 Operation related 2
2 80 M 1992-11-04 DG T2N1M0 Lymph node metastasis 24
3 82 M 2000-11-30 DG T2N1M0 Peritoneal seeding 12
4 82 M 2001-07-24 DG T2N1M0 Local recurrence 31
5 80 F 1999-09-14 DG T2N1M0 Peritoneal seeding 10
6 84 F 1994-07-27 DG T3N1M0 Peritoneal seeding 39
7 80 F 1996-12-31 DG T3N1M0 Peritoneal seeding 39
8 82 F 1997-07-08 TG T3N2M0 Peritoneal seeding 5
9 80 M 1993-03-08 DG T3N2M0 Operation related 2
10 80 M 1999-04-07 DG T3N2M0 Liver metastasis 8
11 80 M 1995-01-19 DG T2N3M0 Lymph node metastasis 24
12 80 M 1997-10-24 TG T3N3M0 Lymph node metastasis 15
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Table 2. Number of gastric cancer-related death and none gastric
cancer-related death
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ No. of No. of Total No. of
Stage gastric cancer none gastric death patients
-related death cancer-related death ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Ia 2 1 1
Ib 5 0 5
II 7 4 3
IIIa 3 2 1
IIIb 4 3 1
IV 2 2 0
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Total 23 12 11
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 압, 허혈성 심장질환, 그리고 부정맥 등의 심혈관계 질환이
동반되어 있었다. 대상 환자 중 22명이 위암 1기로 판정되 었고, 위암 4기로 판정된 2예는 림프절 전이가 16개 이상인 환자였다. 수술 후 입원기간은 평균 17일이었으며, 이 중 수 술관련 사망과 재수술이 시행된 5예를 제외한 36명의 입원 기간은 15일이었다. 총 4예에서 수술관련 합병증이 발생하 여 3예에서 재수술이 시행되었고, 수술관련 사망은 2예에 서 있었다(Table 1).
2) 병기별 사망원인 분석
2004년 2월 현재, 대상 환자 중 23명(56%)이 사망하였으 며, 이중 수술관련 사망 2예를 포함한 위암 관련 사망은 12 명이었고, 다른 원인에 의한 사망은 11명이었다. 병기에 따 른 사망환자는, 1기 22명(53%) 중 7명이 사망하였고, 2기는
10명(24%) 중 7명 사망, 3기와 4기 9명(22%)은 전원이 사망 하였다. 이들 사망환자 중 위암 관련 사망은 1기 7명 중 1명, 2기 7명 중 4명, 그리고 3,4기의 환자는 7명이 위암과 관련 하여 사망하였다(Table 2).
위암 1기와 2기에 해당하는 32명의 중앙생존기간 및 평 균생존기간은 52.5개월이었다.
3) 위암관련 사망환자의 임상적 특징 및 수술 후 경과 수술 관련 사망 2예는 모두 흡인성 폐렴이 원인이었으며, 다른 10명 모두는 방사선학적 혹은 개복소견으로 재발이 확인된 경우였다. 재발양상은 복막전이가 5명으로 가장 많 았으며 이들의 중앙생존기간은 13.5개월이었다(Table 3, Fig. 1).
Fig. 1. Cause of death in cancer related death.
Table 4. Clinical features and postoperative course of none gastric cancer-related death
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Operarion Operation Survival time
No. Age Sex TNM Cause of death
date name (Mon)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
1 80 M 1990-01-29 DG T1N0M0 Senility 59
2 84 F 1991-10-01 DG T2N0M0 Senility 11
3 82 M 1994-11-22 TG T2N0M0 Senility 94
4 80 M 1999-09-14 DG T2N0M0 Senility 13
5 82 M 1996-05-30 TG T2N0M0 Pneumonia 51
6 82 M 1997-10-29 DG T2N0M0 Colorectal cancer 22
7 80 F 1995-05-16 DG T2N1M0 Senility 113
8 81 M 1997-06-11 DG T2N1M0 Colorectal cancer 73
9 80 M 1990-04-25 DG T3N0M0 Unknown 88
10 80 M 1994-07-12 DG T3N1M0 Senility 113
11 82 M 1999-07-07 ETG T4N1M0 Senility 4
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Fig. 2. Cause of death in none related death.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 4) 다른 원인에 의한 사망 환자의 임상적 특징 및 원인
분석
이들 모두는 재발의 증거는 없었고, 11명 중 7명이 노쇠 로, 그리고 1명은 원인미상으로 사망하였다. 원인미상으로 분류된 환자는 가족들의 증언 내용으로는 수술 후 7년간 건강히 생존했으나 통계청자료상 원인미상으로 분류되어 다른 원인에 의한 사망환자에 포함시켰다. 노쇠로 인한 사 망환자 중 2예에서 생존기간이 1년 미만이었는데, 1예에서 는 수술 후 장폐색으로 재수술이 시행되었고, 다른 1예는 확대위전절제가 시행되었다. 이들의 중앙생존기간은 57개 월이었다(Table 4, Fig. 2).
고 찰
고령의 위암환자에서 근치적 위 절제 후 사망원인을 추 적한 결과 첫째, 가장 많은 사망원인은 역시 위암과 관련된 재발이었으며, 이에 영향을 미치는 요인은 타 연령층과 마 찬가지로 병기가 가장 중요하였다. 둘째, 7명이 노쇠로 사 망하였으나, 이들을 포함한 다른 원인에 의한 사망환자의 중앙생존기간이 57개월로 위절제로 인한 생존의 이득은 얻 었다고 할 수 있다. 셋째, 전체 대상 환자 중 32명이 위암 1기와 2기였으며 이들의 평균생존기간 및 중앙생존기간이 모두 52.5개월이었다.
현재까지의 연구결과 고령의 환자에서 동반된 질환과 고 령 그 자체가 하나의 불량한 예후인자가 될 수 있어 수술 범위를 축소해야 한다는 주장과(4-9) 그 반대로 많은 수술 술기의 발달 및 수술 후 관리능력의 증가로 위절제술이 안 전하게 시행될 수 있으며, 또한, 근치적 절제가 이루어진 경 우는 생존율도 차이가 없으므로 적극적인 위 절제를 시행 해야 한다는 주장이 엇갈린 상태였다.(10-15) 하지만 대부 분의 연구 결과 근치적 위 절제가 시행된 환자를 대상으로 하였을 경우는 다른 연령층과 비교하여 생존율의 차이를 보이지 않았으며, 또한 다른 원인에 의한 사망률이 높다하 더라도 연령을 고려하여 생존율을 산출했을 경우, 역시 차 이를 보이지 않았다. 본 연구의 경우, 연구목적상 타 연령층 과 비교하지는 않았으나, 다른 원인으로 사망한 경우 그리 고 위암 제 1기와 2기의 경우 양호한 생존기간을 나타내어 연령이 위 절제를 결정하는 데 제한요인이 되지 않음을 확 인하였다.
수술의 안전성과 관련된 합병증률에 대한 과거 보고를 살펴보면, 국내의 경우 일반적인 위암수술에 따른 합병증 률은 이 등(2)은 13.5%, 조 등(20)은 5.9%내외로 보고하고 있으며, 고령층을 대상으로 한 경우 이 등(2)은 15.1%로 보 고하고 있다. 고령층을 대상으로 한 외국보고의 경우, 보고 마다 많은 차이를 보이고 있으나, 적게는 18.2%에서 많게는 78.0%까지 보고하고 있으며,(2,11,16,17) 본 연구의 경우 전
체 44예 중 4명(9%)의 환자에서 합병증이 발생하여 다른 연 구에 비해 낮게 나타났으나, 이는 비근치적 절제 혹은 고식 적 우회로 설치 등의 환자를 제외하였기 때문으로 판단되 었다.
수술관련 사망에 대해 적게는 0%에서 많게는 23%까지 보고하고 있으며,(8,9,15-17,21) 본 연구의 경우 2명의 환자 에서 수술관련 사망이 발생되어 4.5%를 보였다. 대개 수술 관련 사망의 원인에 대해서는 보고자마다 다르기는 하나, 초창기는 주로 기술적인 문제인 문합부 누출이 가장 많았 고,(15,22) 최근 보고들은 동반된 내과적 질환이 주된 사망 의 원인이라고 보고하고 있다.(16,23) 본 연구에서는 2명 모 두 호흡기계 합병증으로 사망하였는데, 그 중 1예는 수술 후 6일째 발생한 흡인성 폐렴이 호흡부전으로 진행되면서 인공호흡기를 동반한 보존치료에도 불구하고 수술 후 2개 월만에 사망하였고, 다른 1예 역시 흡인성 폐렴이 발생하여 보존치료로 증상이 호전되어 수술 후 28일경 퇴원하였으 나, 3주 뒤 응급실로 호흡곤란과 청색증을 주소로 내원하여 사망하였다. 이는 고령 환자에게 있어서 상복부 수술시 가 장 중요한 수술 후 관리가 호흡기계 관리임을 다시 한 번 일깨워 주는 결과를 보였다.
또한 본 연구에서 노쇠로 사망한 2명의 환자에서 수술 후 생존기간이 각각 4개월 및 11개월로 낮게 나타났는데, 이 중 4개월간 생존한 경우는 췌미부를 함께 절제하는 확대위 전절제가 시행되어 술 후 2주에 건강히 퇴원하였고, 사망 2주 전인 술 후 3개월경 외래 진찰결과도 이상소견이 없었 으며 가족들의 증언과 통계청자료를 토대로 노쇠로 분류하 였다. 또 다른 예인 11개월간 생존한 경우는 수술 후 유착으 로 재수술이 시행되면서 입원기간이 2달 이상으로 길어진 경우였으나 이후 마지막 외래 방문일인 사망 1개월 전까지 건강히 생활하였다. 하지만, 수술범위가 커지거나 합병증으 로 재수술이 시행되는 경우는, 젊은 연령층에서도 환자에 게 많은 스트레스가 가해짐은 당연하므로, 전신상태가 전 반적으로 약화되어 있는 고령층에서는 생존과 직결될 수 있음을 항상 염두해 두어야 할 것이다.
점차 노인층이 증가하고 있는 현실에서 고령의 위암환자 를 만나게 되는 것은 어쩌면 당연한 일일 것이다. 만일 이러 한 환자들에게, 당장 수술의 위험과 고통은 제외하더라도, 삶의 질을 떨어뜨릴 수 있는 위절제술을 시행 받고, 장기생 존의 이득 없이 다른 이유로 사망하게 된다면 이는 환자, 가족, 및 담당의 모두에게 정말로 안타까운 일일 것이다. 다 행히 본 연구결과는 저자들이 우려하던 바와는 달리, 일부 의 환자만 다른 원인으로 사망했으며 그들 또한 재발의 증 거 없이 일정기간 생존하였으므로 위 절제가 도움이 됨을 확인하였다. 물론 대상 환자 수가 적고, 다른 연령층과 기대 여명에 대한 비교가 없어 이를 그대로 수용하기에는 무리 가 있으리라 여겨지나, 고령의 인구가 기하급수적으로 증 가하고 있는 현실에서 이들 연령층의 자연경과를 이해하는
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 데 있어서 본 연구결과가 중요한 기초 자료가 될 것이다.
결 론
위암으로 근치적 위절제술을 결정하는 데 있어서 연령은 제한 요인이 되지 않으므로, 동반된 순환기계 및 호흡기계 질환이 전신마취와 개복수술에 문제가 되지 않은 한, 적극 적인 위 절제를 시행해야 한다고 판단하였다.
REFERENCES
1) Korea national statistical office. Korean statistical information system. 2001.
2) Lee JH, Hyung WJ, Noh SH, Min JS. A comparison of cancer related survival rate in extreme aged gastric cancer patients.
J Korean Surg Soc 2000;59:609-20.
3) Kwon SJ, Choi DH, Park YS, Lee HC, Lee GJ, Kwon OJ, et al. Comparative studies on clinicopathologic characteristics and surgical results in senile and young patients with gastric cancer.
J Korean Surg Soc 1997;52:535-42.
4) Ishigami S, Natsugoe S, Hoity S, Iwashige H, Saihara T, Tokushige M, et al. Strategy of gastric cancer in patients 85 years old and older. Hepatogastroenterology 1999;46:2091-5.
5) Eguchi T, Takahashi Y, Ikarashi M, Kasahara M, Fujii M. Is extended lymph node dissection necessary for gastric cancer in elderly patients? Eur J Surg 2000;166:949-53.
6) Viste A, Haugstvetd T, Eide GE, Soreide O, Norweigian stom- ach cancer trial members. Postoperative complications and mortality after surgery for gastric cancer. Ann Surg 1988;207:
7-13.
7) Morel P, Egeli RA, Wachtl S, Rohner A. Results of operative treatment of gastrointestinal tract tumors in patients over 80 years of age. Arch Surg 1989;124:662-4.
8) Damhuis RAM, Tilanus HW. The influence of age on resection rates and postoperative mortality in 2773 patients with gastric cancer. Eur J Cancer 1995;31A:928-31.
9) Franco R, Daniele M, Alfonso S, Angelo M, Enrico P, Alfonso C. Complication after surgery for gastric cancer in patients aged 80 years and over. Jpn J Clin Oncol 1998;28:116-22.
10) Kaoru K, Keizo S, Motonori S. Evaluation of surgical treat- ment for patients with gastric cancer who are over 80 years of age. Hepatogastroenterology 1999;46:2074-80.
11) Hanazaki K, Wakbayashi M, Sodeyama H, Miyazawa H, Yokoyama S, Sode Y, et al. Surgery for gastric cancer in patients older than 80 years of age. Hepatogastroenterology 1998;45:268-75.
12) Korenaga D, Baba H, Kakeji Y, Orita H, Haraguchi M, Maehara Y, et al. Comparison of R1 and R2 gastrectomy for gastric cancer in patients over 80 years of age. J Surg Oncol 1991;48:
136-41.
13) Maehara Y, Oshiro T, Oiwa H, Oda S, Baba H, Akazawa K, et al. Gastric carcinoma in patients over 70 years of age. Br J Surg 1995;82:102-5.
14) Bandoh T, Isoyama T, Toyoshima H. Total gastrectomy for gastric cancer in the elderly. Surgery 1991;109:136-41.
15) Tsujitani S, Katano K, Oka A, Ikeguchi M, Maera M, Kaibara N. Limited operation for gastric cancer in the elderly. Br J Surg 1996;83:836-9.
16) Korenaga D, Moriguchi S, Baba H, Kakeji Y, Orita H, Haraguchi H, et al. Surgery for gastric carcinoma is feasible for patients over 80 years of age. World J Surg 1991;15:
642-8.
17) Takeda J, Tanaka T, Koufuji K, Kodama I, Tsuji Y, Kakegawa T. Gastric cancer surgery in patients aged at least 80 years old.
Hepatogastroenterology 1994;41:516-20.
18) Houry S, Amenabar J, Rezvant A, Huguier M. Should patients over 80 years old be operated on for colorectal or gastric cancer? Hepatogastroenterology 1994;41:521-5.
19) Ishigami S, Natsugoe S, Saihara T, Hokita S, Tokushige M, Watanabe T, et al. Cilincal and pathological features of early gastric cancer in elderly patients. Hepatogastroenterology 1997;44:1164-8.
20) Cho SH, Kim BS, Kim YH, Lee CH, Yook JH, Oh ST, et al. Clinical analysis of postoperative complications in gastric tumors. J Korea Surg Soc 2001;61:498-503.
21) Fielding JWL, Powell DJ, Allum WH, Waterhouse JAH, McConKey CC. Cancer of the stomach. Clinical cancer mono- graphs. vol. 3. London:Macmillan Press, 1991.
22) Inberg V, Heinonen P, Lauren R, Rantakokko V. Total and proximal gastrectomy in the treatment of gastric carcinoma.
World J Surg 1981;5:249-57.
23) Bittner R, Schirrow H, Butlers M, Roscher R, Krautzberger W, Oettinger W, et al. Total gastrectomy: a fifteen-year expe- rience with particular experience to the patients over seventy years of age. Arch Surg 1985;120:1120-225.