원 저
Korean Circulation J 2004;34(10):930-936
스텐트내 미만성 재협착 환자에서 죽상경화반 절제술 후
188 Re-MAG 3 을 이용한 방사선 치료의 장기적 결과
울산대학교 의과대학 서울아산병원 내과학교실,1 핵의학과학교실2
오성주
1·박성욱
1·홍명기
1·김영학
1·이승환
1·김민규
1이봉기
1·문대혁
2·오승준
2·이철환
1·김재중
1·박승정
1Long-Term Outcomes after Treatment of Diffuse In-Stent Restenosis with Rotational Atherectomy Followed by Beta-Radiation Therapy with a
188Re-MAG
3-Filled Balloon
Sung-Joo Oh, MD1, Seong-Wook Park, MD1, Myeong-Ki Hong, MD1, Young-Hak Kim, MD1, Seung-Whan Lee, MD1, Min-Kyu Kim, MD1, Bong-Ki Lee MD1, Dae Hyuk Moon, MD2, Seung Jun Oh, PhD2, Cheol Whan Lee, MD1, Jae-Joong Kim, MD1 and Seung-Jung Park, MD1
1Departments of Medicine and 2Nuclear Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
ABSTRACT
Background and Objectives:Intracoronary radiation therapy for in-stent restenosis has been demonstrated to reduce restenosis and major adverse cardiac events. However, the long-term angiographic and clinical outcomes after beta radiation therapy have not been sufficiently evaluated. Subjects and Methods:The long- term angiographic and clinical outcomes of 50 consecutive patients who had received beta-radiation therapy with an 188Re-MAG3-filled balloon after rotational atherectomy for diffuse in-stent restenosis (lesion length
>10 mm) in native coronary arteries were evaluated. The radiation dose was 15 Gy at a depth of 1.0 mm into the vessel wall. Results:The mean lesion length was 25.6±12.7 mm. Radiation was delivered successfully to all patients, without any procedural or in-hospital complications. At the 6-month angiogram, the restenosis rate was 10% (5/50). There were no major adverse cardiac events (MACE), such as death, myocardial infarction or target lesion revascularization (TLR), by the 6-month follow-up. Long-term clinical data were obtained from all patients during 30.1±4.5 months of follow-up. No myocardial infarction and one noncardiac death occurred during follow-up. A two-year follow-up angiogram was performed in 26 (58%) of 45 patients that showed a patent radiation segment at the 6-month angiogram. Significant narrowing of the diameter stenosis greater than 50% occurred in 6 (23%) of 26 patients between 6- and 24-months after the beta-radiation. Late TLR was performed in 6 patients. The rate of 30-month death-free survival and MACE-free survival were 98.0±2.0 and 86.9±5.0%, respectively. Conclusion:Beta-radiation using an 188Re-MAG3-filled balloon after rotational atherectomy is associated with favorable long-term angiographic and clinical outcomes. (Korean Circulation J 2004;34(10):930-936)
KEY WORDS:Coronary restenosis;Brachytherapy;Atherectomy, coronary.
논문접수일:2004년 3월 13일 심사완료일:2004년 6월 18일
교신저자:박성욱, 138-736 서울 송파구 풍납동 388-1 울산대학교 의과대학 서울아산병원 내과학교실 전화:(02) 3010-3150·전송:(02) 486-5918·E-mail:[email protected]
서 론
1977년 Gruentizig에 의해서 최초 관동맥성형술이 시술된 이후, 재협착을 낮추기 위해 여러 노력이 있었다.
관동맥내 스텐트 시술은 단순 풍선 도자 관동맥 성형술 (plain old balloon angioplasty)에 비하여 재협착을 감 소시킨다.1)2) 그러나 스텐트내 재협착(in-stent res- tenosis:ISR)이 일부 환자에서 발생하며, 특히 여러 개의 스텐트를 시술한 환자나 긴 스텐트을 사용한 환자 그리고 반복된 관동맥 성형술이 시행된 환자에게서 높 은 재협착율을 보여 또 하나의 문제로 제시되었다.3-9) 최근 여러 임상 연구에서 스텐트내 재협착이 있는 환자 에서 국소적인 γ 혹은 β 방사선 치료가 재협착이나 중 대한 심장 관련 부작용(major adverse cardiac event:
MACE)의 발생을 줄일 수 있음을 보고하였다.10-12) 저 자들 또한 재협착을 가진 환자에서 회전죽종절제술(ro- tational atherectomy) 후에 188Re-MAG3을 이용한 β 방사선 치료의 안전성과 효율성을 보고한 바 있다(R4 registry).13) 그러나 방사선치료의 장기적 효율성과 안 정성에 관하여는 지금까지 잘 알려져 있지 않다. 이에 저자들은 앞서 보고한 R4 registry 환자군의 장기적인 (2년) 임상적 그리고 관동맥 조영상의 결과를 알아보고 자 하였다.
대상 및 방법
대 상
본 연구는 1993년 3월부터 2000년 2월까지 서울 아 산병원에 내원한 미만성의 스텐트내 재협착을 가진 환 자 중 본 연구에 동의한 연속적인 50명을 대상으로 하 였다. 방사선 치료 대상의 기준은 협심증이나 객관적인 허혈성 심질환의 증거를 보이는 관동맥 병변들 중 미만 성의(병변 길이>10 mm, 내경협착>50%) 스텐트내 재 협착으로 하였다. 제외 대상은 72시간내의 급성 심근경 색증, 신기능 저하(혈청 creatinine>3.0 mg/dL), 임신, 항혈소판 치료에 금기를 가진 환자, 그리고 다른 장기에 심각한 병이 동반되어 생존 가능성이 2년 미만으로 예 상되는 환자들로 하였다. 부가적인 새로운 스텐트 삽입 술은 비록 금기는 아니지만, 가능한 시행하지 않았다.
본 연구는 저자들 병원의 임상 윤리위원회(Institutional Review Board)에서 승인을 받은 후 시행되었다.
방 법
방사선 치료 이전에 만족할 만한 혈관 조영상의 결과 (diameter stenosis<20%)를 얻기 위해 회전죽종절제 술(rotational atherectomy)과 보조적인 풍선 성형술을 시행하였다. 풍선 도자는 시술에 의한 손상을 입지않 은 가장자리의 원위부와 근위부를 최소 5 mm까지 포함 하여 방사선 조사를 할 수 있도록 긴 길이의 도자를 사 용하였다. 방사선 조사 시간은 1.0 mm 혈관벽 깊이에 15 Gy의 방사선이 조사되는데 걸리는 시간을 계산하여 결정하였다. 모든 환자는 200 mg의 아스피린과 500 mg의 ticlopidine 그리고 200 mg의 cilostazol을 시술 2일전부터 매일 투여 받았으며, 이후 ticlopidine은 1달 동안, 아스피린과 cilostazol은 방사선 치료 후 지속적으 로 투여하였다.13)
정량적 관동맥 조영 소견의 분석(Quantitative coronary an- giography;QCA)
정량적 관동맥 조영 시스템(ANCOR version 2.0, Sie- mens, Germany)을 사용하여 분석을 시행하였다. 계측 은 관동맥을 통하여 니트로글리세린을 투여 후 이완기 에 이루어 졌다. 유도 도자(guiding catheter)의 직경과 의 비율을 이용하여 가장 심한 내경협착을 보이는 부위 의 직경(minimal lumen diameter)과 참조혈관(refer- ence vessel)의 직경을 비교하였다.
임상적 및 관동맥 조영의 추적관찰(Clinical and angiographic follow-up)
모든 환자는 방사선 치료후 1, 3, 6개월에 외래에 방 문하도록 하였으며 그 이후로 3개월마다 방문하도록 하였다. 관동맥 조영술은 6개월과 2년에 시행하였으나 일부 임상적으로 필요한 경우에는 조금 더 일찍 시행 하였다. 추적 관찰 기간 중 사망, 비치명적인 심근 경색, 그리고 재시술 등을 포함한 중대한 심장 관련 부작용 (Major adverse cardiac events:MACE)을 조사하였 다. 심근경색은 심근 효소가 3배 이상 증가하 거나 30 분 이상 지속되는 흉통, 혹은 심전도상 새로 생긴 변 화로 진단하였다. 2년 추적 혈관조영술상의 재협착은 내경이 50%이상 좁아진 것을 기준으로 하여 QCA를 통하여 측정되었다. 2년 추적 혈관조영술의 분석은 6 개월 추적에서 재협착이 없었던 환자군만을 대상으로 하였다.
통계적 분석
범주형 변수는 빈도 및 퍼센트로, 연속형 변수는 평 균±표준 편차로 나타내었다. 연속형 변수는 paired Student’s t-test와 ANOVA 및 post-hoc analysis 를 시행하여 비교하였고, p 값이 0.05 미만일 때 통계학 적으로 유의하다고 판정하였다. Kaplan-Meier법을 이 용하여 생존 곡선을 구하였다.
결 과
입원 경과 및 시술 결과
50명의 환자가 회전죽종절제술과 보조적인 풍선 도 자 시술을 시행 받은 후에 방사선 치료를 시행받았다. 위 험 인자로는 고혈압이 38%, 당뇨가 26%, 고콜레스테 롤혈증이 24%, 흡연이 62%이었다. 8명의 환자(16%)
는 진구성 심근경색을 가지고 있었으며 7명의 환자는 스텐트내 재협착으로 인해 적어도 한번 이상의 시술을 시행받은 환자들이었다. 회전죽종절제술의 평균 burr size는 2.06±0.21 mm이었고 burr/artery ratio는 0.72±0.09이었다. 병변의 길이와 방사선이 조사된 길 이의 평균은 각각 25.6±12.7 mm, 37.6±11.2 mm이 었고 평균 조사시간은 201.8±61.7초였다. 6명의 환자 에서는 방사선 조사를 분할하여 시행하였으며(fractio- nation), 7명의 환자에서는 병변의 길이가 길어서 30 mm의 풍선 도자를 단계적으로(manual stepping) 사 용하였다(Table 1). 부가적인 새로운 스텐트 삽입술 이 필요하여 시행된 환자는 없었으며, 시술과 연관된 합병증이나 입원기간 중에 MACE는 관찰되지 않았다.
경과 관찰
모든 생존한 환자에서 평균 30.1±4.5개월간 임상적 추적이 이루어졌으며, 임상적 결과는 Table 2에 제시하 였다. 이전에 저자들은 6개월 추적에서 5명의 환자에서 재협착이 나타났음을 보고하였는데, 이들 모두에서 증상 이 경미하거나(3명) thallium 스캔 소견상 이상 소견이 없었기 때문에(2명) 재시술이 시행되지 않았었다. 이들 중 2명은 증상이 악화되어 시술 후 10, 12개월에 재시 술이 시행되었고, 또한 1명은 2년 추적 조영술에서 내 경협착이 진행되었고 흉통의 악화소견이 있어 관동맥 우 회수술을 시행 받았다. 그리고 나머지 2명은 지속적으 로 약물치료를 받고 있다.
2년 추적 조영술에서 새로이 6명의 환자에서 재협착 이 발견되었으며 이 중 3명이 재시술(target lesion re- vascularization)을 시행받았다. 따라서 전체환자 50명 Table 1. Baseline clinical and angiographic characteristics
Characteristics n=50
Age (years) 56±90
Male (%) 42 (84)
Risk factors (%)
Hypertension 19 (38)
Diabetes mellitus 13 (26)
Total cholesterol ≥240 mg/dL 12 (24)
Current smoker 31 (62)
Prior myocardial infarction 08 (16)
Unstable angina 33 (66)
Left ventricular ejection fraction (%) 60±7 Rotablation procedure
Mean burr size (mm) 2.1±0.2
Burr/artery ratio 0.7±0.1
Artery treated (%)
Left main coronary artery 01 (02%) Left anterior descending artery 34 (68%) Left circumflex artery 05 (10%) Right coronary artery 10 (20%) Balloon/artery ratio 1.18±0.14 Lesion length (mm) 25.6±12.7 Reference vessel diameter (mm) 2.89±0.40 Radiation therapy
Length of irradiated segment (mm) 37.6±11.2 Overlap of two balloons 07 (14%)
Fractionation 06 (12%)
Exposure time (sec) 202±620
Table 2. Clinical outcomes of study patients
At 6 months At 6 to 30 months
Death 0 1 (02%)
Noncardiac 0 1 (02%)
Cardiac 0 0
Nonfatal myocardial infarction 0 0 Target lesion revascularization 0 6 (12%) Repeat intervention 0 5 (10%) Cardiac bypass surgery 0 1 (02%)
Late thrombosis 0 0
Combined events 0 7 (14%)
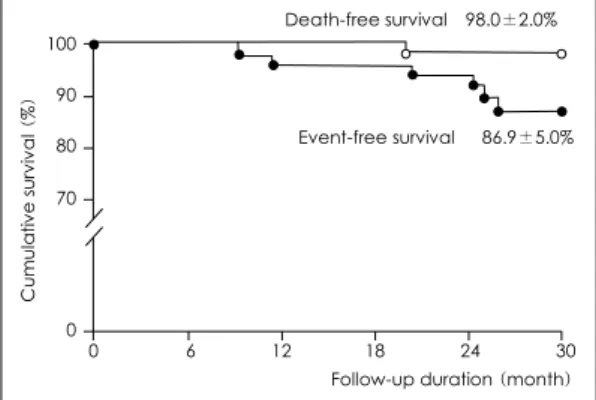
중 6명(12%)에서 재시술이 필요하였으며, 이 중 5명은 cutting balloon을 이용하여 재시술되었고 1명은 관동맥 우회수술을 시행받았다. 추적기간 중 한명의 환자가 악 성종양으로 20개월째 사망하였으며 나머지 환자에서는 MACE가 없었다. 30개월 생존율과 MACE없는 생존율 은 98.0±2.0%와 86.9±5.0% 였다(Fig. 1).
관동맥 조영 소견의 분석(Angiographic analysis)
시술 후 6개월 추적 조영술은 평균 6.0±2.0개월에 시행되었고 재협착율은 10%(5/50)였다. 2년 추적 조 영술은 초기 조영술에서 재협착이 없었던 45명 중 26 (58%)명에서 시행되었다. 시행되지 못한 19명은 증상이 없어 검사를 거부한 환자들로 이들 중 16명에서 thallium SPECT(n=12)와 운동부하심전도(n=4)를 시행하였고 비정상 영상이나 ST분절의 변화는 관찰되지 않았다.2년 추적 조영술에서 재협착 즉“late catch-up”은 6명 (23%, 6/26)에서 보였는데, 가장자리 재협착(edge res- tenosis)과 국소적인 스텐트내 재협착(focal ISR)이 각
각 한명씩 그리고 미만성과 완전 재협착이 각각 2명씩 이였다. 전체 26명의 환자에서의 최소내경(minimal lu- men diameter)은 시술 후가 2.68±0.46 mm, 6개월째 에 2.31±0.56 mm 그리고 2년째에 1.81±0.43 mm 로 점차 감소되는 형태를 보였다(p<0.05). 그러나 2년 추적까지 재협착이 오지 않았던 20명의 환자들의 최소 내경을 분석해보면, 시술직후 2.84±0.41mm에 비하여 6개월추적에서 2.38±0.69 mm로 의미있게 감소됨을 보였지만(p=0.01), 2년추적에서는 2.26±0.61 mm로 6개월 이후로는 의미있는 감소소견이 관찰되지 않았다 (p=0.57, Fig. 2). 참조혈관(reference vessel)의 직경 은 6개월때와 2년추적에서 의미있는 차이를 보이지 않 았고(2.88±0.40 mm vs. 2.80±0.43 mm p=0.56), 동맥류 형성(aneurysm formation)은 관찰되지 않았다.
고 찰
본 연구로 미만성 스텐트내 재협착이 있는 환자를 대 상으로 시행한 회전죽종절제술(rotational atherectomy) 후 188Re-MAG3을 이용한 β 방사선 치료는 안전하며 효과적인 치료임을 알 수 있었고, 2년 추적 조영술상 일 부환자에서 지연 발생된 재협착의 소견이 관찰됨을 알 수 있었다.
이전연구와의 비교
지금까지 미만성 스텐트내 재협착의 치료를 위한 여 러가지 시도들이 있었음에도 불구하고 재협착율은 여전 히 높은 것으로 알려져있다.14-16) 최근 여러 연구에서 이러한 재협착에서 방사선치료가 일반적 치료에 비하 여 재협착을 낮추고 재시술을 줄인다는 6개월 추적 보
고들과11)12) 장기적 효과의 관찰에 대한 보고가 있었
다.17-19)23) 최근 Teirstein 등17)은 SCRIPPS(The Scri- pps Coronary Radiation to Inhibit Proliferation Post- Stenting) 연구에서 3년간의 추적결과를 보고하였는데 표적혈관 재시술율이 15.4%로 비교군의 44.8%에 비 해 의미있게 낮추었음을 보고하였다(p<0.01). 본 연구 에서는 평균 30.1±4.5개월간의 추적 결과 표적혈관 재 시술율이 12%로 나타났는데, 이는 SCRIPPS의 15.4%
와 비슷한 결과라 할 수 있겠다. SCRIPPS 연구에서는 스텐트내 재협착뿐만 아니라 스텐트삽입이 필요한 풍 선성형술 후 재협착 병변과 이식혈관(saphenous vein Fig. 1. Cumulative probability of survival free from any
cause of death and target lesion revascularization.
Minimal luminal diameter (mm) 4 3 2 1 0
p=0.01 p=0.59
2.84±0.41
2.38±0.69
2.26±0.61
Postprocedure 6-month 2-year
Fig. 2. Serial changes of minimal luminal diameter in 20 patients who did not have significant restenosis at 2-year angiographic follow-up. Postprocedure vs. 6-month, p=
0.01; 6-month vs. 2-year, p=0.59.
Event-free survival 86.9±5.0%
Death-free survival 98.0±2.0%
Follow-up duration (month) 0 6 12 18 24 30
Cumulative survival (%)
100 90 80 70
0
graft) 등을 포함 시켰지만 본 연구에서는 스텐트 시술 후 미만성 재협착을 보인 환자들만을 연구대상으로 하 였기 때문에 절대적인 비교는 어려울 것으로 생각된다.
SCRIPPS 연구에서 3년간 재협착율은 비교군에 비해 의미있게 낮았음을 보고하였고(33% vs. 64%, p<0.05), 또한 QCA 분석상 최소내경이 감소되어 방사선이 재협 착을 지연 시키는 것이 아닌가하는 논의가 있었다. 본 연구에서도 2년간 재협착율은 23%(6/26)로 SCRIPPS 연구와 비슷한 결과를 보였다. 그러나 재협착이 없었던 환자군(n=20)을 대상으로한 최소내경은 6개월부터 2 년사이에 큰 변화가 없는 것으로 나타났다. 그러므로 이 는 후기 재협착(late restenosis)가 오지 않았던 환자에 서 방사선이 조사된 혈관은 안정적임을 보여준다 하겠다.
또한 최근 조 등22)도 레늄-188을 이용한 재협착병 변 치료의 3년간의 장기적 성적을 발표하였는데, 표적 혈관 재시술율이 7.4% 였고 비교군과도 의미있는 차이 를 보여 레늄-188이 장기적으로도 안정적으로 재협착 율을 낮춘다는 것을 보고한 바 있다. 본 연구에서는 조 등의 연구에서와 달리 미만성으로 스텐트내에 재협착 온 환자군만을 대상으로 하였고 죽상경화반 절제술을 시행한 이후에 방사선치료를 하였기 때문에 그의 결과 를 직접 비교는 어려우나, 역시 재협착을 줄일 수 있다 는 동일한 결과를 보였음을 알 수 있었다.
가장자리 재협착(Edge restenosis)와 후기 재협착(late res- tenosis“late catch-up”)
지난 연구들에서 6개월째 가장자리 재협착(edge res- tenosis)의 중요한 원은 geographic miss로 나타났
다.20)21) 그러나 지금까지 후기 재협착(late catch-up)
과 geographic miss와의 연관은 잘 알려진 바 없었다.
본 연구에서는 6명의 후기 재협착 환자에서 모두 시술 시기의 geographic miss가 있었다. 그러나 재협착이 일 어난 부위는 geographic miss가 일어난 부위와 연관되 지 않는 것으로 나타났다. 따라서 geographic miss는 후기 가장자리 재협착(late edge restenosis)과는 연관 이 없다고 판단 할 수 있겠다. 그렇지만 이는 조금 더 대규모 연구가 필요할 것으로 사료된다.
후기 혈전증과 동맥류 형성
방사선 치료의 장기적 문제점으로 동맥류 형성(an- eurysm formation)이나 후기 혈전 등이 거론 되어왔다.
본 연구에서는 동맥류의 형성은 발견되지 않았으나 2명 의 완전 폐쇄가 있었다. 후기 완전 폐쇄는 점진적인 협 착이나 혈전에 의하는데, 혈전의 경우 급성 관동맥 증 후군의 임상형태를 보이는 것으로 알려져있다. 본 연구 에서는 급성 관동맥 증후군의 임상형태를 보인 환자가 없어, 무증상 심근경색(silent myocardial infarction)이 나 점진적 폐쇄에 의했을 것으로 생각된다. 하지만 본 연구에서는 항혈소판제인 aspirin과 cilostazol을 모든 환자에서 추적관찰시점까지 사용하고 있어서 본 연구에 서 관찰된 완전폐쇄현상은 혈전에 의한 것이라기 보다 는 신생내막의 증식에 의한 것으로 판단된다. 이전 연구 에서도 장기적인 항혈소판제재의 사용이 후기 혈전증의 발생을 줄일 수 있다는 보고가 있었으나 적정 사용기간 에 대해서는 더 많은 연구가 필요할 것이다.
연구의 한계
본 연구는 몇 가지 제한점이 있다. 첫째 연구대상이 비교적 적은 수였다는 것이고, 비교 대상군이 없었다는 것이다. 둘째 임상적인 추적은 2년 동안 모두 이루어 졌 으나 2년 추적조영술은 단지 58%의 환자에서만 이루 어졌기 때문에 전체환자의 재협착율을 의미한다 할 수 없다는 점이다. 셋째 본 연구에 사용된 188Re-MAG3나 방사선의 조사량은 다른 연구들과 다르기 때문에 직접 적 비교는 불가능하다는 것이다.
결 론
후기 재협착 현상(late catch-up)은 관찰되었으나 재 협착율은 23%로 낮은 재협착의 효과가 유지 되었으며, 후기 혈전이나 동맥류 형성의 현상은 관찰되지 않았다.
따라서 미만성의 스텐트내 재협착이 생긴 환자에서 회 전죽종절제술(rotational atherectomy) 후 188Re-MAG3
을 이용한 β 방사선 치료의 임상적 효용성은 2년까지 지속되었다 할 수 있다.
요 약
배경 및 목적
:스텐트내 생긴 재협착의 치료로 관동맥내 방사선치료는 재협착 및 주요심사건(major adverse cardiac event;
MACE)을 줄이는 것으로 알려져있다. 그러나 임상적 및 관동맥 조형술상의 장기적 결과는 충분히 연구되어 있
지 않다. 본 연구는 β 방사선 치료의 장기적 효율성과 안전성을 평가하기 위하여 시행되었다.
방 법
:미만성의 스텐트내 재협착의 병변을 가진 50명의 환 자들을 대상으로 회전죽종절제술 후 188Re-MAG3을 채운 풍선 도자를 이용한 방사선 치료를 시행하고, 2년 간 임상적 결과 및 추적 조영술상의 변화를 관찰하였다.
방사선 조사량은 혈관벽내 1.0 mm의 깊이에 15 Gy가 조사되도록 하였다.
결 과
:병변의 평균 길이는 25.6±12.7 mm 였으며, 방사선 은 모든 환자에서 성공적으로 조사되었다. 치료중이나 입원중에 부작용은 없었다. 6개월까지의 임상추적 및 조영술상에서 심근경생이나 사망 같은 MACE나 재협착 에 의한 재시술은 없었으며 재협착율은 10%(5/50)였 다. 추적관찰은 평균 30.1±4.5개월간 이루어졌고, 한 명의 비심장사가 있었으나 나머지 환자에서는 심근경색 이나 심장사는 없었다. 2년째 조영술은 6개월째까지 재 발이 없었던 45명 중 26명(58%)에서 이루어 졌으며, 의 미있는 재협착은 26명의 환자 중 6명(23%)에서 발견 되었다. 전체 50명을 대상으로한 임상적 추적상 생존율 은 98.0±2.0%였으며 MACE 없는 생존율 86.9±5.0%
였다. 또한 재시술이 시행된 경우는 6명으로 12%의 환 자들에게 시술되었다.
결 론
:미만성의 스텐트내 재협착이 생긴 환자에서 회전죽종 절제술 후 188Re-MAG3을 이용한 β 방사선 치료의 장 기 임상적 및 혈관 조영상의 결과는 양호하다.
중심 단어
:스텐트 재협착;방사선 치료;회전죽종절제술.본 연구는 한국과학재단의 연구비 1999-2-206-001-3 의 지원으로 시행되었음.
REFERENCES
1) Fischman DL, Leon MB, Baim DS, Schatz RA, Savage MP, Penn I, Detre K, Veltri L, Ricci D, Nobuyoshi M, Cleman M, Heuser R, Almond D, Teirstein PS, Fish RD, Colombo A, Brinker J, Moses J, Shaknovich A, Hirshfeld J, Bailey S, Ellis S, Rake R, Goldberg S. A randomized comparison of coro- nary-stent placement and balloon angioplasty in the treat- ment of coronary artery disease. N Engl J Med 1994;331:
496-501.
2) Serruys PW, de Jaegere P, Kiemeneij F, Macaya C, Rutsch W, Heyndrickx G, Emanuelsson H, Marco J, Legrand V, Ma-
terne P, Belardi J, Sigwart U, Colombo A, Goy JJ, van den Heuvel P, Delcan J, Morel M. A comparison of balloon- expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;
331:489-95.
3) Hoffmann R, Mintz GS, Dussaillant GR, Popma JJ, Pichard AD, Satler LF, Kent KM, Griffin J, Leon MB. Patterns and mechanism of in-stent restenosis: a serial intravascular ult- rasound study. Circulation 1996;94:1247-54.
4) vom Dahl J, Radke PW, Haager PK, Koch KC, Kastrau F, Reffelmann T, Janssens U, Hanrath P, Klues HG. Clinical and angiographic predictors of recurrent restenosis after percu- taneous transluminal rotational atherectomy for treatment of in-stent restenosis. Am J Cardiol 1999;83:862-7.
5) Sharma SK, Duvvuri S, Dangas G, Kini A, Vidhun R, Venu K, Ambrose JA, Marmur JD. Rotational atherectomy for in- stent restenosis: acute and long-term results of the first 100 cases. J Am Coll Cardiol 1998;32:1358-65.
6) Mehran R, Dangas G, Mintz G, Waksman R, Abizaid A, Sa- tler LF, Pichard AD, Kent KM, Lansky AJ, Stone GW, Leon MB. Treatment of in-stent restenosis with excimer laser co- ronary angioplasty versus rotational atherectomy: compa- rative mechanisms and results. Circulation 2000;101:2484-9.
7) Reimers B, Moussa I, Akiyama T, Tucci G, Ferraro M, Mar- tini G, Blengino S, di Mario C, Colombo A. Long-term cli- nical follow-up after successful repeat percutaneous inter- vention for stent restenosis. J Am Coll Cardiol 1997;30:
186-92.
8) Dauerman HL, Baim DS, Cutlip DE, Sparano AM, Gibson CM, Kuntz RE, Carrozza JP, Garber GR, Cohen DJ. Mech- anical debulking versus balloon angioplasty for the treatment of diffuse in-stent restenosis. Am J Cardiol 1998;82:277-84.
9) Lee SG, Lee CW, Cheong SS, Hong MK, Kim JJ, Park SW, Park SJ. Immediate and long-term outcomes of rotational atherectomy versus balloon angioplasty alone for treatment of diffuse in-stent restenosis. Am J Cardiol 1998;82:140-3.
10) Teirstein PS, Massullo V, Jani S, Popma JJ, Mintz GS, Russo RJ, Schatz RA, Guarneri EM, Steuterman S, Morris NB, Leon MB, Tripuraneni P. Catheter-based radiotherapy to inhibit restenosis after coronary stenting. N Engl J Med 1997;
336:1697-703.
11) Waksman R, Bhargava B, White L, Chan RC, Mehran R, Lansky AJ, Mintz GS, Satler LF, Pichard AD, Leon MB, Kent KK. Intracoronary β-radiation therapy inhibits recurr- ence of in-stent restenosis. Circulation 2000;101:1895-8.
12) Waksman R, White RL, Chan RC, Bass BG, Geirlach L, Mintz GS, Satler LF, Mehran R, Serruys PW, Lansky AJ, Fitzgerald P, Bhargava B, Kent KM, Pichard AD, Leon MB.
Intracoronary γ-radiation therapy after angioplasty inhibits recurrence in patients with in-stent restenosis. Circulation 2000;101:2165-71.
13) Park SW, Kim JH, Choi S, Hong MK, Moon DH, Oh SJ, Lee CW, Kim JJ, Park SJ. Treatment of diffuse in-stent reste- nosis with rotational atherectomy followed by radiation therapy with a rhenium-188-Mercaptoacetyltriglycine-filled balloon. Korean Circ J 2001;31:466-75.
14) Dietz U, Rupprecht HJ, de Belder MA, Wijns W, Quarles van Ufford MA, Klues HG, vom Dahl J. Angiographic analysis of the angioplasty versus rotational atherectomy for the treat- ment of diffuse in-stent restenosis trial. Am J Cardiol 2002;
90:843-7.
15) Mehran R, Dangas G, Abizaid AS, Mintz GS, Lansky AJ, Satler LF, Pichard AD, Kent KM, Stone GW, Leon MB.
Angiographic patterns of in-stent restenosis: classification and implications for long-term outcome. Circulation 1999;
100:1872-8.
16) Hamburger JN, Foley DP, de Feyter PJ, Wardeh AJ, Serruys PW. Six-month outcome after excimer laser coronary angio- plasty for diffuse in-stent restenosis in native coronary ar- teries. Am J Cardiol 2000;86:390-4.
17) Teirstein PS, Massullo V, Jani S, Pompa JJ, Russo RJ, Schatz RA, Guarneri EM, Steuterman S, Sirkin K, Cloutier DA, Leon MB, Tripuraneri P. Three-year clinical and angiographic follow-up after intracoronary radiation: results of a rando- mized clinical trial. Circulation 2000;101:360-5.
18) Grise MA, Massullo V, Jani S, Popma JJ, Russo RJ, Schatz RA, Guameri EM, Steuterman S, Cloutier DA, Leon MB, Tripuraneni P, Teirstein PS. Five-year clinical follow-up after intracoronary radiation: results of a randomized clinical trial. Circulation 2002;105:2737-40.
19) Waksman R, Ajani AE, White RL, Pinnow E, Mehran R, Bui
AB, Deible R, Luis G, Mintz GS, Satler LF, Pichard AD, Kent KM, Lindsay J. Two-year follow-up after beta and gam- ma intracoronary radiation therapy for patients with diffuse in-stent restenosis. Am J Cardiol 2001;88:425-8.
20) Sianos G, Kay IP, Costa MA, Regar E, Kozuma K, de Feyter PJ, Boersma E, Disco C, Serruys PW. Geographical miss during catheter-based intracoronary beta-radiation: incid- ence and implications in the BRIE study. J Am Coll Cardiol 2001;38:415-20.
21) Kim HS, Waksman R, Cottin Y, Kollum M, Bhargava B, Me- hran R, Chan RC, Mintz GS. Edge stenosis and geographical miss following intracoronary gamma radiation therapy for in-stent restenosis. J Am Coll Cardiol 2001;37:1026-30.
22) Jo SJ, Kim KI, Koo BK, Lee MM, Park SJ, Seo JB, Lee JH, Chae IH, Kim MA, Kim HS, Sohn DW, Oh BH, Park YB, Choi YS. Long-term follow-up results of intracoronary beta- radiation therapy with a rhenium-188 diethylene triamin penta-acetic acid-filded balloon. Korean Circ J 2003;33:
723-9.