CASE REPORT
ISSN 2508-1926Copyright © 2016 The korean retina society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Retina 2016;1(2):101-104 http://dx.doi.org/10.21561/jor.2016.1.2.101
초진 당시 허혈성 시신경병증으로 오진되었던 매독성 시신경병증
Syphilitic Optic Neuritis Initially Misdiagnosed as Ischemic Optic Neuropathy
이로운, 김태경, 이미연
Rowoon Yi, Tai Kyong Kim, Mee Yon Lee
가톨릭대학교 의과대학 의정부성모병원 안과
Department of Ophthalmology, Uijeongbu St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea
Purpose: To report a syphilitic optic neuritis case, initially misdiagnosed as arteritic ischemic optic neuropathy (AION), in which prior transient posterior placoid chorioretinitis was an important clue to the correct diagnosis.
Case summary: A 50-year-old man presented with blurry vision in the right eye. Funduscopy revealed optic disc swelling. Due to an elevated erythrocyte sedimentation ratio and C-reactive protein, our initial impression was AION. However, the diagnosis was corrected after reviewing a previous fundus photo revealing a large, pale yellow placoid lesion in the macula of the right eye. Serological examina- tions revealed confirmed syphilis infection. After a 2-week treatment with penicillin G, visual symptoms and signs fully resolved.
Conclusions: Optic neuropathy with an elevated erythrocyte sedimentation ratio and C-reactive protein should prompt suspicion for syphilitic optic neuritis. Misdiagnosis as AION could lead to steroid therapy without antibiotics, which can worsen prognosis.
Keywords: Acute syphilitic posterior placoid chorioretinitis; Ischemic optic neuropathy; Ocular syphilis; Optic neuritis; Syphilitic optic neuritis
Introduction
Syphilis is a sexually transmitted disease caused by the spirochete Treponema pallidum. Ocular syphilis is an un- common but diagnostically important manifestation of the disease. It may be silent or present as anterior uveitis, cho- roiditis, interstitial keratitis, retinal vasculitis, retinitis, optic neuritis, dacryoadenitis, or scleritis in both human immuno- deficiency virus (HIV) positive and HIV negative patients [1].
Uveitis is reportedly the most common ocular manifestation of ocular syphilis [1]. Optic nerve involvement in syphilis,
the more infrequent type of ocular syphilis, may be unilater- al or bilateral, and becomes apparent as perineuritis, anterior or retrobulbar optic neuritis, or papilledema [2].
Delayed anti-treponemal therapy can result in permanent visual loss, and steroid therapy without adjunctive antibiot- ic treatment may increase the treponemal load. Thus, it is important to rule out treponemal disease at an early stage.
However, the characteristics distinguishing syphilitic optic neuritis from nonsyphilitic involvement of a similar distribu- tion are unclear.
We present a case of syphilis in an immunocompetent pa-
Address reprint requests to Mee Yon Lee, MD, PhD
Department of Ophthalmology, The Catholic University of Korea Uijeongbu St. Mary’s Hospital, #271 Cheonbo-ro, Uijeongbu 11765, Korea
Tel: 82-31-820-3022, Fax: 82-31-847-3418 E-mail: [email protected]
Received: 2016. 9. 6.
Revised: 2016. 9. 19 Accepted: 2016. 9. 19
102
JOURNAL OF RETINA
http://dx.doi.org/10.21561/jor.2016.1.2.101 tient who was initially misdiagnosed with arteritic ischemic
optic neuropathy (AION). We belatedly reviewed the initial fundus photo provided by a clinic that the patient had pre- vious visited and corrected the diagnosis to acute syphilitic posterior placoid chorioretinitis (ASPPC).
Case Report
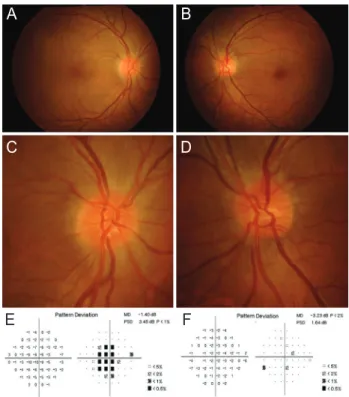
A 50-year-old male presented with a 7-day history of sig- nificant visual loss in the right eye. Examination revealed a best-corrected visual acuity of 20/100 in the right eye and 20/20 in the left eye. The patient had diabetes and was taking diabetes medication. A right relative afferent pupillary defect (RAPD) was elicited. The Ishihara test showed decreased col- or vision. Funduscopy revealed optic disc swelling with blur- ring of the disc margin in both eyes, which was prominent in the right eye and otherwise unremarkable (Fig. 1A-D). There were no signs of inflammation in the anterior segments or the vitreous. Humphrey perimetry (24-2 Swedish Interactive Threshold Algorithm Standard) testing revealed an extensive central scotoma in the right eye, leading to a lack of reli- ability in the left eye (Fig. 1E, F). Initial laboratory findings revealed an elevated erythrocyte sedimentation ratio (ESR) and C-reactive protein (CRP).
The patient had visited another clinic 4 days previously.
His visual symptoms had partially improved without any treatment. However, the vision in the right eye worsened, prompting the visit to our clinic. Due to the elevated ESR and CRP in our initial blood test, AION was the provision- al diagnosis. For the AION work-up, we consulted with a rheumatologist about this case and further blood screening including platelets was performed. We considered system- ic steroids and temporal artery biopsy and the patient was asked to return the following day with the data from the pre- vious clinic visit.
The following day, we reviewed the fundus photo from the previous clinic, which revealed a large, yellow-white, placoid lesion of the right macula (Fig. 2A, B). A fundus flu- orescein angiogram conducted at the previous clinic demon- strated early and late phase staining of the optic disc, but no clear sign of leakage. We also observed early central hypo- fluorescence and progressive late hyperfluorescence in the area of the placoid lesion (Fig. 2C, D). There were no signs of any retinal edema or serous detachment on macular opti-
cal coherence tomography (Fig. 2E, F). Thus, we had a high level of clinical suspicion regarding ASPPC, and conducted a rapid plasma regain test as a screening for acute syphilis infection. After a positive rapid plasma regain test (RPR;
1:128), we performed a T. pallidum particle agglutination as- say and a serum fluorescent treponemal antibody absorption test to confirm the diagnosis and discontinued the work-up for AION. Finally, these confirmative tests revealed positive results.
A cerebrospinal fluid (CSF) tap revealed CSF protein and glucose within the normal range. The CSF white cell count was slightly elevated and the CSF RPR was negative. The patient did not have any systemic symptoms of syphilis, such as malaise, headache, nausea, or constipation. There were no other systemic manifestations including chancres, con- dyloma lata, macular papular rash, or lymphadenopathy. His personal, family and social histories were unremarkable and A
C
Figure 1. Clinical features of patient at the time of presentation.
Best-corrected visual acuity was 20/100 in the right eye and 20/20 in the left eye. There were no abnormal findings, except for the optic disc, in fundus photographs (A, B). Optic disc stereophotography revealed optic disc swelling with blurring of the disc margin in both eyes which was prominent in the right eye (C, D). Visual field testing revealed depression of the central field in the right eye (E), leading to a lack of reliability in the left eye due to too many fixation losses (F).
MD = mean deviation; PSD = pattern standard deviation.
B
D
F A
C
E
103
Yi R, et al. Syphilitic optic neuritis
http://dx.doi.org/10.21561/jor.2016.1.2.101 his HIV titers were negative.
A diagnosis of syphilitic optic neuritis accompanied by syphilitic posterior placoid chorioretinitis in the acute phase was made. As optic neuritis and retinitis are generally con- sidered neurosyphilis and should be managed accordingly, he was admitted for a 2-week course of 1.2 g intravenous benzylpenicillin every 4 hours. Visual acuity, color vision, and optic disc swelling fully recovered after 2 weeks of pen- icillin treatment (Fig. 3). Three months after treatment, the RPR titer was reduced from 1:128 to 1:32.
Discussion
In patients with optic neuropathy and elevated ESR and CRP, a high degree of suspicion should be present for AION.
Systemic steroids should be given immediately once AION is suspected. However, our case showed that infectious dis-
ease, especially ocular syphilis, should always be on the list of differential diagnoses in optic neuritis with elevated ESR and CRP. Misdiagnosis of ocular syphilis as AION would lead to unnecessary temporal artery biopsy and steroid ther- apy without adjunctive antibiotics, which would worsen the prognosis by increasing the treponemal load.
Ocular syphilis has diverse possible clinical signs and symptoms. It should be ruled out in all patients with ocu- lar inflammation including optic neuritis. The sooner the treatment is initiated, the better the outcome, partly because secondary irreversible injuries like optic nerve atrophy or ganglion cell degeneration can be prevented. However, due to the lack of distinguishing characteristics of syphilitic op- tic neuritis and nonsyphilitic involvement, prompt diagnosis is often challenging, especially when there are no systemic manifestations, as in the present case.
There is often cellular activity in the posterior vitreous in anterior syphilitic optic neuritis. However, there were no such vitreous signs in our patient. Therefore, the ASPPC macular lesion identified in the present case was invaluable for diagnosis. ASPPC is a distinctive manifestation of ocular syphilis characterized by the development of a placoid mac- ular deposit in the outer retina.
However, problematically, ASPPC can be evident only transiently. In our patient, the ASPPC had resolved sponta- A
C
E
B
D
F
Figure 2. Prior clinical data. Best-corrected visual acuity was 20/200 OD and 20/20 OS. Fundus examination of the right eye demonstrat- ed features of acute syphilitic placoid posterior uveitis, with retinal opacification in a round or oval area of the posterior pole (A). Fundus examination of the left eye was similar to that of the presentation in our clinic (B). Fluorescein angiography findings showed an early hy- pofluorescent macular lesion (C) followed by late-staining hyperfluo- rescence (D). Optical computed tomography of the right eye showed nodular hyperreflectivity of the RPE without subretinal fluid (E). There were no signs of any retinal edema or serous detachment on macular optical computed tomography of the left eye (F). S = superior; N = nasal; I = inferior; T = temporal.
A
C
B
D
Figure 3. Clinical features of patient after treatment. Fundus photo- graphs (A, B) and optic disc stereophotography (C, D) of both eyes after treatment. After treated with a 2-week course of penicillin G in- fusions, optic disc swelling was resolved in both eyes. Best-corrected visual acuity was improved to 20/25 in the right eye and 20/20 in the left eye.
104
JOURNAL OF RETINA
http://dx.doi.org/10.21561/jor.2016.1.2.101 neously without systemic penicillin treatment. By the time of
the visit to our clinic, this clinical clue was no longer appar- ent on a fundus exam. Therefore, even though there may be no abnormal funduscopic finding other than optic disc swell- ing, a high degree of clinical suspicion about syphilitic optic neuritis should be retained. As in the present case, review of the initial fundus photo or charts from previous clinics that a patient visited can detect this important but transient clue.
If a clinic is equipped with spectral domain-optical computed tomography (SD–OCT), detection of an already resolved ASPPC lesion is possible. SD-OCT imaging can re- veal prominent nodular elevation of the RPE that can persist for up to 1 month after treatment [3].
In patients with ASPPC, circulating T. pallidum enters the choroidal circulation and gains access to the outer retina where the choroidal vascular supply is greatest, especially in the macula [4]. This can explain the presently observed simultaneous development of ASPPC and optic neuritis, be- cause the posterior ciliary artery derived from the choroidal circulation is not only the main source of blood supply to the macular lesion but also the optic head, except for the nerve fiber layer.
Even though the outer retina of the macula and optic nerve were involved simultaneously in our case, ASPPC resolves quickly without treatment, while optic neuritis does not. The retinal pigment epithelium (RPE) may contribute to this difference. The RPE shares several functions with macrophages, including expression of Toll-like receptors, complement, and bacterial phagocytosis [5]. Since spiro- chetes are effectively eradicated by the engulfing activity of macrophages, we can deduce that phagocytosis of the RPE is also effective in eliminating this microorganism. SD-OCT imaging of ASPPC reveals irregular hyperreflectivity of the RPE with prominent nodular elevation [3]. This also sug- gests the possibility that RPE layers are crucially involved in the mechanism of ASPPC.
Even though capillaries of the optic nerve head have tight
junctions and nonfenestrated endothelium, which represent a nerve-blood barrier against microorganisms, they are just passive physical barriers and do not have an active function like the RPE. Clinicopathologic examination combined with molecular analysis is required to confirm this hypothesis.
In conclusion, even though optic neuropathy with elevated ESR and CRP is an important feature of AION, a high de- gree of clinical suspicion regarding syphilitic optic neuritis is also vital in these patients. Misdiagnosis of syphilitic optic neuritis as AION can lead to steroid therapy without adjunc- tive antibiotics, which will worsen the prognosis. Even when there is no abnormal funduscopic finding other than optic disc swelling, previous fundus photographs or chart data should be reviewed. These efforts can hasten diagnosis and result in prompt treatment with benzylpenicillin in cases of transient ASPPC, as in our patient.
Conflicts of interest There are no conflicts of interest.
References
1. Tamesis RR, Foster CS. Ocular syphilis. Ophthalmology 1990;97:1281-7.
2. Smith GT, Goldmeier D, Migdal C. Neurosyphilis with optic neu- ritis: an update. Postgrad Med J 2006;82:36-9.
3. Pichi F, Ciardella AP, Cunningham ET Jr, et al. Spectral domain optical coherence tomography findings in patients with acute syphilitic posterior placoid chorioretinopathy. Retina 2014;34:373-84.
4. Gass JD, Braunstein RA, Chenoweth RG. Acute syphilitic posteri- or placoid chorioretinitis. Ophthalmology 1990;97:1288-97.
5. Namperumalsamy P, Rathinam SR. Mycobacterial Infections. In:
Ryan SJ, ed. Retina, 5th ed. London: Saunders/Elsevier, 2013; 1473-8.