73
Case Report
ISSN 2465-8243(Print) / ISSN: 2465-8510(Online) http://dx.doi.org/10.14777/uti.2016.11.2.73 Urogenit Tract Infect 2016;11(2):73-75
Renal Actinomycosis Initially Misdiagnosed as Renal Cell Carcinoma with Renal Vein Thrombosis
Jong Wook Kim, Hyoung Kook Jeong, Jong Jin Park, Ji Yun Chae, Hong Seok Park, Du Geon Moon, Mi Mi Oh Department of Urology, Korea University Guro Hospital, Seoul, Korea
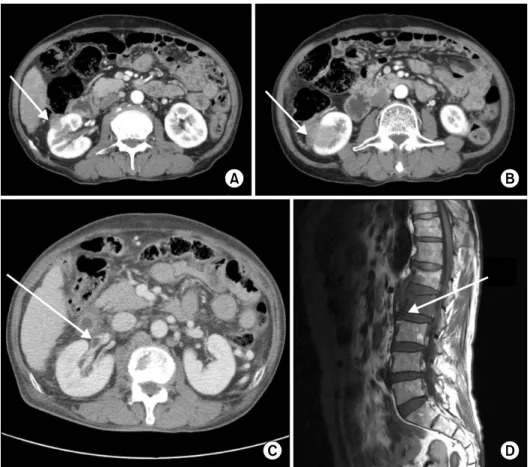
This case report describes an uncommon case of renal actinomycosis in a 63-year-old man. The patient underwent radical nephrectomy for suspicious renal cell carcinoma with renal vein thrombosis and spinal metastasis. The postoperative diagnosis of renal and spinal actinomycosis was established in accordance with the results from histological examination. Three years after surgery, the patient did not show any symptoms of recurrence.
Keywords: Actinomycosis; Carcinoma, renal cell; Renal vein thrombus
Copyright 2016, Korean Association of Urogenital Tract Infection and Inflammation. All rights reserved.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 March, 2016 Revised: 13 June, 2016 Accepted: 8 July, 2016
Correspondence to: Mi Mi Oh