Abstract : Colorectal cancer is the third most frequently diagnosed cancer in Korea (2007). It is the third leading cause of cancer death in men and the forth leading cause of cancer death in women. The mortality from colorectal cancer has increased slightly over the past 10 years for the westernization of Korean diet. But the survival rate is increasing with endoscopic surgery and chemotherapy regimens including a VEGF(Vascular Endotherial Growth Factor) inhibitor or an EGFR(Epidermal Growth Factor Receptor) inhibitor. The objective of the study is to review and evaluate the adjuvant chemotherapy after surgery and the chemotherapy of advanced or metastatic disease by NCCN(National Comprehensive Cancer Network) guideline in oncology (for colon cancer) V.2.2010. We reviewed retrospectively the EMR of 29 patients who had received adjuvant chemotherapy after surgery from January 2007 to December 2009. The use of adjuvant chemotherapy for patients with stage II colon cancer is controversal. The adjuvant therapy with FOLFOX, 5-FU/LV or capecitabine is recommended for patients with stage III disease, and as an option for patients with high-risk stage II disease by NCCN guideline. And irinotecan-containing regimens should not be used as adjuvant therapy in colon cancer. All of the patients with stage II lesions were received LF regimen regardless of risk-based stage in NPH(National Police Hospital). The use of irinotecan-containing regimens(IFL or FOLFIRI) as adjuvant therapy in 3 cases of 21 cases is not appropriated(14.3%). Recommended initial therapy options for advanced or metastatic disease depend on whether or not the patient is appropriate for intensive therapy. And chemotherapy options for patients with progressive disease are dependent on the choice of initial therapy. The use of IFL regimen for advanced disease is no longer recommended for its toxicity and is removed from the guideline. However we found that 5 cases of 9 patients in advanced or
대장암에 대한 항암화학요법 사용평가
경찰병원 약제과
The Review of Chemotheraphy in Colorectal Cancer
Eun Mi Bang, Yun Hee Park, Won Kyu Kim, and Keum Sook Lim
Department of pharmacy, National Police Hospital, 58 karak-dong, songpa-gu, Seoul, 138-708, Korea
회원학술보고
보건복지부의 주요 암통계에 의하면 2007년 암발 생자수는 161,920명으로 전년도에 비해 1.06% 증가 하였으며, 남자는 위암, 폐암, 대장암, 간암, 전립선 암 순, 여자는 갑상선샘암, 유방암, 위암, 대장암, 폐 암 순으로 많이 발생하였다. 이 중 대장암은 전체의 12.7%를 차지하고 있으며 위암, 갑상선샘암에 이어 3위를 차지하며, 1999년의 9.6%에 비교시 매년 0.4% 내외로 증가함을 알 수 있다. 연령대별로는 60 대가 30.5%로 가장 많고, 70대가 24.6%, 50대가 22.3%의 순으로 많이 발생된다. 암에 의한 전체 사 망률은 폐암, 간암, 위암, 대장암 순이며, 이중 대장 암은 남자는 세번째로, 여자는 네번째로 사망률이 높 았다. 2006년 대비 사망률이 가장 많이 증가된 암은 대장암으로 서구식 식습관으로 인한 대장암 발생률 이 급격히 증가됨이 그 원인이라 하겠다. 전체 암환 자의 5년 상대 생존율은‘03~07년’57.1%로
‘01~05년’53.1% 대비 4% 증가하여 꾸준한 향상을 보이고 있으며, 대장암의 경우는‘03~07년’68.7%
로 비교적 높은 편이다.
대장암의 위험인자로는 고지방, 고칼로리, 저섬유 소 식이습관, 50대 이상의 고령, 염증성 장질환, 용 종, 가족력, 유전자적인 소인 등이 있다. 미국의 경 우는 대장암 환자의 1/3정도가 가족력과 관련이 있 고, 질환의 위험도를 증가시켜 가족력이 있는 환자의 경우 세심한 주의를 기울일 것을 권장하고 있다.
Hereditary NonPolyposis colorectal Cancer(HNPCC)와 Familial Adenomatous Polyposis(FAP)의 경 우 는 MLH1(MutL homolog1), MSH2(MutS homolog2) gene mutation과 APC(Adenomatosis polyposis coli)
gene mutation에 각각 관련이 있고 특히 HNPCC 는 대장암으로 발병할 가능성이 높다. 또한 대장암 환자의 80% 이상은 선종성 용종으로부터 암성변화 를 일으켜 발병되어진다.
대장암의 치료는 내시경 및 수술을 통한 절제술, 방 사선치료, 항암화학요법 등이 있으며 여러 가지 치료 가 병합하여 이용되기도 한다. 최근 분자 및 세포 생 물학의 발달로 암세포에 대한 표적 치료제가 개발되 어 기존 항암화학요법과 조합 혹은 단독 사용으로 진 행성 대장암의 생존기간을 향상시키고 있다. 이에 본 연구에서는 최근 대장암에 대한 본원의 항암화학요 법을 조사하고 2010년 National Comprehensive Cancer Network(NCCN) guideline in Colon Cancer를 기준으로 평가하여 개선점을 제시하여 환자에게 양질의 의료서비스를 위한 병원약사의 중 재역할 부분을 제시하고자 한다.
Ⅰ. 연구방법
1. 연구 대상
2007년 1월 1일부터 2009년 12월 31일까지 본원 에 대장암 절제술 후 항암치료목적으로 혈액종양내 과에 입원한 환자 중 무균 주사조제실로 항암제 조제 를 의뢰한 29명을 대상으로 하였고, 전자의무기록을 조회하여 후향적으로 조사하였다.
2. 조사내용
1) 환자특성 : 성별, 연령분포, 기저질환, 가족력 metastatic disease were received IFL regimen. Therefore, it is recommended that the use of IFL regimen for advanced disease should be limited.
[Key words] colorectal cancer, adjuvant chemotherapy, chemotherapy of advanced or metastatic disease
투고일자 2010. 5. 4; 심사완료일자 2010. 5. 17; 게재확정일자 2010. 5. 29
2) Adjuvant chemotherapy: Stage Ⅱ, Stage
Ⅲ별 대장암 절제술 후 시행한 regimen 분석 3) Chemotherapy for advanced or metastatic colorectal cancer : 진행 및 전이된 대장암 환자를 집중치료가 필요한 군과 필요하지 않는 군으로 분류 하여 사용한 regimen 분석
4) Chemotherapy induced nausea and vom- iting(CINV) 예방 및 치료 : regimen별 CINV 예방 및 치료 분석
5) 항암화학요법 실시 중 용량 감량 및 투여 중단 사유
6) 항암치료 후 감시 및 관리
3. 조사기준
대장암의 adjuvant chemotherapy와 진행 및 전 이성 대장암의 항암화학요법 조사기준은 NCCN Clinical Practice Guideline in colon can- cer(2010)을 기초로 범주화하여 조사하였다. CINV 예방 및 치료는 regimen별로 치료일정에 따라 단독 항암제의 Hesketh level을 기준하거나 또는 동시 투여되는 항암제의 각각의 Hesketh level을 고려한 emetogenic potential을 기준하여 본원의 CINV 예방 및 치료 전략을 조사하였다.
Ⅱ. 결과
1. 환자특성
환자의 남녀 구성은 남자 24명(82.8%), 여자 5명 (17.2%)이었으며, 환자의 연령대별 분포는 60대가 10명으로 전체 중 34.5%를 차지하였고, 50대가 8명 (27.6%), 70대가 6명(20.7%), 40대가 4명(13.8%), 30대가 1명(3.4%) 순이었다. 기저질환으로는 고혈 압, 당뇨병, 간염, 골다공증, 결핵 순으로 많았고, 대 장암 가족력이 있는 환자는 1명이었다.
2. Adjuvant chemotherapy
대장암 환자 29명 중 결장암은 20명, 직장암은 9명
으로 대부분 adenocarcinoma였으며, right hemicolectomy한 환자는 11명(37.9%), left hemicolectomy한 환자는 5명(17.2%), sig- moidectomy한 환자는 3명(10.3%), low anterior resectomy한 환자는 9명(31.0%)이었고 1명은 타병 원에서 수술하여 정확한 기록이 없었다.
본원에서는 대장암의 진행단계를 American Joint Committee on Cancer(AJCC)에서 제시 한 AJCC Cancer staging Manual에 기준으로 한 TNM 병기를 사용하여 분류하고 있었다.
(Table 1) 수술 후 항암화학요법은 대장암 절제 후 isolated metastasis 절제술을 받은 2명의 환자 를 제외하고 산출한 결과 평균 30일 이후에 실시하 였다. 수술 후 실시한 adjuvant chemotherapy 대상환자는 Stage Ⅱ, StageⅢ환자로 이루어져 있었고 Stage Ⅰ환자는 없었다. 진단 당시 TNM 병기를 기준으로 하여 최초 사용한 adjuvant chemotherapy는 StageⅡ(ⅡA,ⅡB)환자에서는 LF regimen만 사용하여 100%였고, StageⅢ(Ⅲ A, ⅢB, ⅢC)환자의 경우는 LF(61.5%), FOL- FOX4(15.4%), FOLFIRI(15.4%), IFL(7.7%) regimen 순으로 사용하였다.(Table 2, Table 3)
3. Chem ot her apy f or advanced or metastatic colorectal cancer
Adjuvant chemotherapy 후 전이된 환자는 결장 암환자는 20명 중 4명, 직장암은 9명 중 5명으로 직 장암의 전이률이 높았으며 조사기간 3년동안의 EMR 조회를 기준으로 산출한 결과 평균 2년 3개월 후에 재발하였고, 조사 대상 대장암 환자 중 31.0%
가 전이 및 재발로 진행되었다. 전이된 장기는 폐,
간, 복막 순으로 호발되었고, 기타 신장, 췌장, 식도
로도 전이가 되었으며, 폐 및 간으로의 전이가 전체
중 66.7%를 차지하였다. 진행성 및 전이성 대장암에
사 용 된 chemotherapy regimen은 LF,
Capecitabine, FOLFOX4, FOLFIRI, IFL과
anti-VEGF(Vascular Endothelial Growth
Factor)제인 bevacizumab과 FOLFIRI, beva-
cizumab과 IFL가 있었으며, 환자의 상태에 따라
NCCN guideline에 기준하여 2그룹으로 나누어 조 사하였다. (Table 4) 집중적인 치료가 적절하지 않 은 환자는 1st line으로 LF(1st~6th), Capecitabine regimen을 사용하였고 2nd line으로 동일한 LF(7th~12th), IFL regimen을 사용하였으며, 집 중적인 치료가 적절한 환자는 1st line으로 FOLFIRI, FOLFOX4, IFL을 사용하였고 2nd line 으로는 bevacizumab+FOLFIRI, bevacizumab+IFL,
FOLFIRI, FOLFOX4, Capecitabine regimen을 사용하였다.
4. Chemot herapy induced nausea and vomiting(CINV) 예방 및 치료
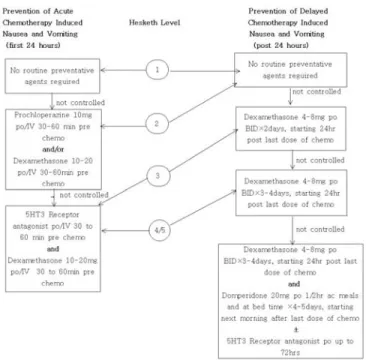
환자가 항암화학요법시 가장 많이 접하게 되는 부 작용이 CINV이며 각각의 regimen에 따라 CINV가 유발되는 정도가 상이하며, 환자에 따라서도 차이가 있으며, chemotherapy가 거듭되면서 발생빈도가 증가하는 양상을 보였다. 본원에서 대장암에 대한 항 암화학요법의 regimen별로 급성 CINV, 지연성 CINV 예방 및 치료전략을 조사한 결과 가장 많이 사 용한 LF regimen에 대한 CINV 예방 및 치료는 Hesketh level 2로 ondasetron 8mg inj.(day1- day5)으로 관리가 잘 되고 있었다. 반면, FOL- FOX4와 FOLFIRI regimen에 대한 예방 및 치료 는 chemotherapy 첫째날이 level 4임에도 불구하 고 ondasetron 8mg inj.(day1-day2)으로 관리하 고 있어 CINV가 유발되는 경우에는 둘째날에 ondasetron 8mg inj.외에 lorazepam 2mg inj.
혹은 dexamethasone 5mg inj. 을 증세에 따라 추 가하여 진정시켰다. IFL regimen (level 4)을 사용 하는 경우는 1, 8, 15, 22일째 날에 ondasetron 8mg inj.으로 CINV를 예방하였고, 지연성 구토 발 생 은 적 어 추 가 적 인 조 치 사 항 은 없 었 다 . Capecitabine regimen(level 2)은 CINV 예방조치 가 없음에도 불구하고 발현되지 않았다.(Table 5) 지연성 구토가 진정되지 않고 계속 진행되는 경우는 항도파민제로 metoclopramide 5mg 경구제, metoclopramide 10mg 주사제 혹은 domperi- done 10mg 경구제를 사용하고 그 외 항세로토닌제 인 ondansetron 8mg 경구제를 보조요법으로 사용하 고 있었다. Bevacizumab을 병용한 regimen의 경우 는 bevacizumab이 Hesketh level 1로 CINV유발 에 크게 영향을 미치지 않았다.
Table 1. TNM stages for carcinoma of the colon and rectum
Tis T1 T2 T3
T4
Cacinoma in situ and intramucosal (within lamina propria) Invades through muscularis mucosa into submucosa Invades muscularis propria
Invades through muscularis propria into subserosa or nonperitonealized pericolic or perirectal tissues Invades adjacent organs or structures or perforates visceral peritoneum
Modified from American Joint Committee on Cancer. AJCC staging menual, 6th ed. New York: Springer-Verlag,2002.
Primary tumor
0
Ⅰ
ⅡA
ⅡB
ⅢA
ⅢB
ⅢC
Ⅳ
Tis, N0, M0 T1 OR T2, N0, M0 T3, N0, M0 T4, N0, M0 T1-2, N1, M0 T3-4, N1, M0 Any T, N2, M0 Any T, any N, M1
Stage grouping
N0N1 N2
No nodal metastasis
Metastasis in 1-3 regional nodes Metastasis in 4 or more regional nodes
Regional lymph nodes
M0 M1
None Present
Distant metastasis
Drug
5-Fluorouracil Leucovorin Oxaliplatin Leucovorin 5-Fluorouracil 5-Fluorouracil Irinotecan Leucovorin 5-Fluorouracil 5-FluorouracilBevacizumab
Irinotecan Leucovorin 5-Fluorouraci
Bevacizumab
Capecitabine
Dose
400-425mg/㎡20mg/㎡
85mg/㎡
200mg/㎡
400mg/㎡
600mg/㎡
180mg/㎡
400mg/㎡
400mg/㎡
2400mg/㎡
5mg/kg
100-125mg/㎡
20mg/㎡
400-500mg/㎡
5mg/kg
1250mg/m2 po twice daily
Schedule
day 1-5 day 1-5 day 1 day 1, 2 day 1, 2 day 1, 2 day 1 day 1, 2 day 1, 2 day 1-2day 1
day 1,8,15,22 day 1,8,15,22 day 1,8,15,22
day 1,15,29
day 1-14
Infusion time
bolusbefore 5-FU 2hrs 2hrs
bolus after leucovorin CIV 22hrs 90 min.
2hrs bolus 46-48hrs
90min. for initial dose: if tolerated next infusion 60min. and then 30min.
90 min.
bolus bolus
90min. for initial dose: if tolerated next infusion 60min. and then 30min.
-
Cycle frequency
28days14days
14days
42days
21days
Table 3. Chemotherapy regimens for colorectal cancer
Regimen LF
FOLFOX4
FOLFIRI
+bevacizumab
IFL
+bevacizumab
Capecitabine
Table 4. Chemotherapy for advanced or metastatic colorectal cancer
Patient not appropriate for intensive therapy
Patient appropriate for intensive therapy
LF IFL (2cases) FOLFIRI+bevacizumab FOLFIRI Capecitabine IFL+bevacizumab+
Capecitabine FOLFOX4
Second-line therapy
LFCapecitabine FOLFIRI
FOLFOX4
IFL
First-line therapy Table 2. Adjuvant chemotherapy regimens
for TNM stages of colorectal cancer
ⅡA(T3,N0,M0)
ⅡB(T4,N0,M0)
ⅢA(T1-2,N1,M0)
ⅢB(T3-4,N1,M0)
ⅢC(anyT,N2,M0)
Ⅱ
Ⅲ
Stage
6 2 1 1 3 1 1 4 1 1
No. of use
LFLF LF FOLFOX4
LF FOLFIRI
IFL LF FOLFOX4
FOLFIRI
Regimen
5. 항암화학요법 실시 중 용량 감량 및 투여 중단 사유
LF, Capecitabine regimen은 hand-foot syn- drome으로 투여를 중단하였고, FOLFOX4, FOLFIRI, IFL은 neutropenia, leukemia, diar- rhea, LFT 수치 상승으로 투여를 중지하거나 감량 하였다. 이 중 IFL이 neutropenia, leukemia, diarrhea가 다른 regimen보다 심하게 나타났으며, Capecitabine regimen의 경우는 neutropenia로 투여를 중단하거나 감량한 예는 없었다.
6. 항암치료 후 감시 및 관리
항암치료 후 전이암이나 진행암으로 재발을 감시하 기 위해 주로 carcinoembryonic antigen(CEA), computed tomography of abdomen and pelvis(AP-CT), colonoscopy를 주기적으로 실시 함으로 관리하고 있었고, 또한 positron emission tomography (PET)/CT로 전이여부를 판단하는 기 준으로 주기적(평균 9.7개월)으로 시행하고 있었다.
NCCN guideline에 따르면 CEA는 치료 후 2년동
안 3-6개월마다, 그 후 총 5년내에 6개월마다 측정 하 고 , AP-CT는 3년 동 안 매 년 검 사 하 며 , colonoscopy는 치료 1년 후에 실시하고, advanced adenoma 유무에 따라 존재하면 1년 후에 한번 더 실시하고, 그렇지 않은 경우는 3년 후에 실시하며 그 후에는 5년마다 실시하는 것으로 되어 있다. 반면 일 반적으로 시행하는 PET/CT scan은 권장하고 있지 않다. 본원에서 항암치료 후 follow-up을 기록이 미비한 환자 1명과 치료기간이 짧은 1명을 제외하고 NCCN guideline으로 적합성 여부를 평가한 결과 27명 중 CEA는 23명(85.2%)이, AP-CT와 colonoscopy는 각각 22명(81.5%)이 기준에 적합하 였다.(Table 6)
Ⅲ. 평가기준
대장암 수술 후 adjuvant chemotherapy와 진행 암 및 전이암 chemotherapy 평가 기준은 2010년 NCCN Clinical Practice Guideline in colon cancer를 기준하였고, 진행 및 전이된 대장암의 항 암화학요법은 초회 치료와 치료 후 1차 진행한 경우 Regimen
LF
FOLFOX4
FOLFIRI±
bevacizumab
I F L ± bevacizumab
Capecitabine
Emetogenic potential
Days 1-5: level* 2Day 1: level 4 Day 2: level 2
Day 1: level 4 Day 2: level 2
Day 1,8,15,22: level 4
Day 1-14: level 2
Prevention of acute CINV
ondansetron 8mg inj.ondansetron 8mg inj.
ondansetron 8mg inj.
ondansetron 8mg inj.
-
Prevention of delayed CINV
ondansetron 8mg inj.ondansetron 8mg inj.±
lorazepam 2mg inj. ± dex- amethasone 5mg inj.
ondansetron 8mg inj.±
lorazepam 2mg inj. ± dexam- ethasone 5mg inj.
-
-
Table 5. Prevention of Chemotherapy induced nausea and vomiting
* Hesketh level: level of emetogenicity according to the Hesketh classification (J ClinOncol 15:103-109,1997)
만 고려하여 평가하였다.(Table 7, Table 8) CINV예방 및 치료계획에 관한 평가기준은 reg- imen별로 각 항암제의 Hesketh Level로 산출한 Hesketh Level of emeogenic potential을 기 준으로 하여(Table 9, Fig. 1) 권고안으로 평가하 였다.(Fig. 2)
Ⅳ. 고찰
대장암은 상대적으로 항암화학요법에 내성을 나타 내는 암으로 알려져 왔으나, 최근 새로운 항암제의 도입과 분자생물학의 발전에 따른 생물학적 표적치 료의 개발로 생존기간이 연장되고 삶의 질 향상을 가
Surveillance
∙CEA every 3-6mo for 2y, then every 6mo for a total of 5y for T2 or greater lesions
∙Chest/abdominal/pelvic CT annually×3y for patients at high risk for recurrence
∙Colonoscopy in 1y except if no preoperative colonoscopy due to obstructing lesion, colonoscopy in 3-6mo
∙If advanced adenoma, repeat in 1y
∙If no advanced adenoma, repeat in 3y, then every 5y
∙PET/CT scan is not routinely recommended
Pathologic stage
Stage Ⅰ T1-2,N0,M0
Stage ⅡA T3,N0,M0
no high risk features
Stage ⅡA, ⅡB T3-4,N0,M0
T3 with high risk features*
Stage Ⅲ T1-4,N1-2,M0
Adjuvant Therapy
NoneConsider Capecitabine or 5-FU/leucovorin or Clinical trial or Observation 5-FU/leucovorin/oxaliplatin or Capecitabine or 5-FU/leucovorin or Clinical trial or Observation 5-FU/leucovorin/oxaliplatin or Capecitabine or 5-FU/leucovorin
Table 7. Pathologic Stage, Adjuvant Therapy and Surveillance (NCCN guideline 2010 in colon cancer)
* High risk for systemic recurrence: grade 3-4, lymphatic/vascular invasion, bowel obstruction, <12LN examined
Accepted n (%)
23(85.2%)22(81.5%)
22(81.5%)
Unaccepted n (%)
4(14.8%)5(18.5%)
5(18.5%)
Colorectal Cancer Surveillance
CEA every 3-6 months for 2 years, then every 6 months for a total of 5 years
CT scan of abdomen and pelvis annually for 3 years Colonoscopy in 1 year
- If advanced adenoma, repeat in 1 year
- If no advanced adenoma, in 3 years, then every 5 years
Table 6. Appropriateness for colorectal long-term follow-up care
져오게 되었다. 항암화학요법은 근치적 수술 후 재발 을 줄이는 목적으로, 수술이 불가능한 진행성 대장암 의 경우에는 생존기간 연장 및 삶의 질 향상을 목적 으로 시행되어 지고 있다.
대장암 병기는 과거에는 Dukes' staging system 및 Astler-Coller modifications를 사용했으나 최 근에는 TNM 병기가 생존률의 차이를 정확하게 반 영하여 권장되고 있다. 예를 들면 low grade tumor 인 ⅡA(T3N0M0)는 수술 후 5년 disease-free survival (DFS)이 약 74%이며, ⅡB(T4N0M0)는 약 63%로 감소되는 반면 ⅢA(T1-2N1M0)는 5년 DFS가 약 71%로 ⅡB에 비해 생존율이 높다.
본원에서 대장암 절제술 후 시행되는 adjuvant chemotherapy regimen을 분석한 결과 stage Ⅱ 의 경우는 LF regimen을, stage Ⅲ에서는 LF, FOLFOX4, FOLFIRI, IFL regimen을 사용하였 다. NCCN의 자료에 의하면 Europian MOSAIC trial에서 adjuvant chemotherapy로 FOLFOX4 와 5-Fluorouracil(5-FU)/leucovorin(LV)의 효 능을 비교한 결과 stage Ⅱ 환자의 경우는 5-year disease-free survival(DFS)에 있어서는 두 군에 서 통계학적으로 유의적인 차이가 없었으나, stage
Ⅲ환자의 경우는 5-year DFS이 5-FU/LV는 58.9%, FOLFOX4는 66.4%로 통계학적으로 유의
Patient appropriate forPatient not appropriate for Intensive therapy
Initial therapy
FOLFOX ± bevacizumab or CapeOX* ± bevacizumab or FOLFOX ± cetuximab or
panitumumab
(KRAS wild-type gene only)
FOLFIRI +bevacizumab or FOLFIRI ± cetuximab or
panitumumab
(KRAS wild-type gene only)
5-FU/leucovorin +bevacizumab
Therapy after First Progression
FOLFIRIor Irinotecan
or FOLFIRI ± cetuximab or panitumumab (KRAS wild-type gene only) FOLFOX
or CapeOX
or Cetuximab(KRAS wild-type gene only)+irinotecan, patients not able to tolerate combination, consider single agent cetuximab or panitumumab (KRAS wild-type gene only)
FOLFOX or CapeOX or Irinotecan or FOLFIRI
Table 8. Chemotherapy for advanced or metastatic disease (NCCN guideline 2010 in colon cancer)
* CapeOX; oxaliplatin 130mg/㎡ day1, capecitabine 850-1000mg/m2 twice daily for 14days repeat every 3weeks
Capecitabine ± bevacizumab or
Infusional 5-FU +leucovorin ± bevacizumab
Fig. 2 Recommendations for the Prevention and Treatment of Nausea and Vomiting Related to Cancer Chemotherapy
Fig. 1 Determination of Hesketh Level of Emetogenic Potential of Chemotherapy Regimens
적인 차이(P=0.005)가 있음을 보고하였다. 따라서 이러한 근거에 의하면 본원에서 사용하는 LF regi- men이 5-FU/LV와 다소 차이는 있지만 stage Ⅱ 에서 LF regimen을 사용하는 것이 NCCN의 기준 에서 적합하다고 볼 수 있겠다. 또한 US inter- group trial CALGB C89803에서는 stage Ⅲ 환자 에 IFL regimen을 5-FU/LV regimen과 비교하여 시행한 결과 overall survival이나, DFS면에서 5- FU/LV regimen보다 향상된 점이 없었으며, 추가 적으로 adjuvant chemotherapy에서 FOLFIRI regimen과 5-FU/LV regimen을 비교시 우수한 점이 없고, 설사 및 혈관계 부작용이 동반되어 stage
Ⅱ나 stage Ⅲ 환자에게 irinotecan이 포함된 reg- imen 사용은 NCCN에서는 권장하고 있지 않다. 이 러한 근거로 평가시 adjuvant therapy에 사용된 21case 중에 irinotecan을 포함한 IFL, FOLFIRI 가 3case로 14.3%가 부적합하였다. 종합적인 NCCN의 adjuvant chemotherapy guideline은 stage Ⅱ 환자의 경우는 수술 후 항암화학요법 시행 여부에 상관없이 5-year overall survival 면에서 통계학적으로 유의적인 차이가 보이지 않아 항암화 학요법 시행을 신중히 고려해야 하며, MOSAIC trial에서는 stage Ⅱ 환자 중 high risk 군(T3- T4, N0, M0)에서 FOLFOX4가 5-FU/LV보다 DFS가 개선되었으며, low risk군에서는 차이가 없 어 stage Ⅱ 환자의 low risk군에는 FOLFOX4는 권장하지 않고 high risk군에는 FOLFOX4를 고려 할 만 하다고 제시하고 있다. Stage Ⅲ 환자의 경우
는 대장암 절제술 후 6개월간 standard regimen으 로 FOLFOX4를 사용하거나, oxaliplatin 사용이 부적합한 환자의 경우 capecitabine 단독요법이나, 5-FU/LV regimen 사용을 권장하고 있으며, irinotecan을 포함하는 regimen은 권장하지 않는 다. 이러한 근거를 본원에 적용해 볼 때 stageⅡ 환 자는 risk별로 구별하지 않고 LF regimen을 사용 하였는데, high-risk군에서는 LF보다는 FOL- FOX4를 고려하는 것이 바람직하다고 볼 수 있고, adjuvant chemotherapy에 irinotecan을 포함하 는 IFL, FOLFIRI regimen 사용은 제한해야 될 것 으로 보인다.
진행성 및 재발성 대장암에 대한 chemotherapy 에 대한 NCCN guideline은 최근 간전이, 폐전이, 간/폐 전이, 복부/복막 전이별로 치료 전략을 개별화 하였다. 우선 전체 대장암환자의 15%-25%가 전이 되는 간의 경우는 이 중 80%-90%가 절제가 불가하 여 수술을 하지 않은 경우 5년 생존률이 낮아 주요한 사인으로 간주되고 있으며, 반면 절제가 가능한 경우 는 치유가능성이 높아 최근 치료전략으로 절제가 불 가한 전이부위를 항암요법으로 절제가능하도록 실시 하는 neoadjuvant chemotherapy 전략을 제안하 고 있으며 최근 보고에 의하면 절제술 후 5년 생존률 을 50%를 상회한다고 보고하고 있다. 하지만 neoadjuvant chemotherapy 시행은 병소 크기를 감소하여 절제가능하게 하는 장점과 이로 인해 수술 시점을 지연하게 되는 단점 및 항암제 독성으로 인한 단점이 교차하여 절제가능하다면 수술을 실시하는 것이 우선되며, 절제 가능여부가 경계에 있는 경우에 는 전이부위 크기를 감소할 목적으로 neoadjuvant chemotherapy를 실시하는 것이 고려할 만하다고 권장하고 있다. 폐전이의 경우는 간전이에 준하여 수 술 및 neoadjuvant chemotherapy를 고려하며 간 과 폐에 동시에 전이된 경우의 절제술은 매우 특수한 경우에 한해 실시하며, 복부/복막에 전이된 경우는 치유보다는 고식적인 요법으로 관리하는 것을 치료 목적으로 제시하고 있다. NCCN guideline에서 제 시하는 neoadjuvant chemotherapy regimen은 FOLFIRI, FOLFOX 혹은 CapeOX[capecitabine, oxaliplatin]에 bevacizumab을 가감하거나 만일 Table 9. Hesketh level of individual
chemotherapeutic agent
Bevacizumab Capecitabine Fluorouracil Irinotecan Oxaliplatin
Agent
12
4
Level
<10%
10-30%
60-90%