5
Malaria Imported by Travelers: Epidemiological Aspects in Korea and Japan
Sang-Hee Park, Ph.D.
1, Myeong-Jin Lee, Ph.D.
2, Kook-Hwan Rhim, Ph.D.
3, Hyeong-Ae Bang, Ph.D.
3, Won-Chang Lee, Ph.D.
41
Division of Zoonoses, Center for Immunology & Pathology, Korea Center for Disease Control & Prevention, Seoul, Korea
2
Public Health in Department of Nutritional Sciences, Otemae College of Nutrition, Osaka, Japan,
3
College of Health Science, Korea University,
4College of Veterinary Medicine, Konkuk University, Seoul, Korea
Background: Malaria imported by travelers has been an increasing problem in Korea and Japan recent two decades, representing one of risk for travelers visiting tropical and sub-tropical countries where malaria is endemic. The present study analyzes all of the malaria cases reported in Korea and Japan during 2002∼2009 in order to assess the trend of incidence over time and review the risk factors for travelers visiting malaria endemic countries. Methods: All malaria cases that occurred during 2002∼2009 in Korea and Japan were analyzed. The incidences of exotic malaria in Korea and Japan were calculated by continent and by countries most visited, using data provided by annual reports of exotic malaria in the Web Statistics System, Korea Center for Disease, and Report of Infectious Disease Surveillance Center, Japan. Results: A total of 11,573 domestic cases of malaria occurred between 2002 and 2009 in Korea, and the average incidence rate was 2.99, and that of malaria imported by travelers in the exotic was 0.08 per 100,000 populations. During the same period in Japan, the incidence rate of exotic malaria was 0.05, and its incidence rate in Korea was much higher than Japan’s. All 2002∼2009 case report of imported malaria in Korea was analyzed. A total 40.9% (124 cases) of 277 cases were infected with Plasmodium falciparum , while 36.0% (109 cases) were diagnosed with P. vivax , 3.3% (10 cases) with P. falciparum and P. vivax mixed, 1.3% (4 cases) with P. ovale , 2.3% (7 cases) with P. malariae and 16.2% (49 cases) with unknown causes. In Japan, the percentages of the 529 cases with P. falciparum, P. vivax, P. ovale, P. malariae and unknown cases were 49.9% (264 cases), 40.1% (212 cases), 4.9% (26 cases), 1.9% (10 cases) and 3.2% (17 cases), respectively. The infection rates of P. falciparum and P. ovale in Japan were noted to be higher than those in Korea ( P <0.05 and P <0.01). A total of 303 cases malaria which was regarded from endemic areas outside Korea was recorded during that time. P. falciparum was predominant in the cases from Africa it forms 80.8% (97 cases) of 120 cases, while P. vivax was the leading protozoa in Asia 73.4% (80 cases) of 109 cases. Moreover, most cases were from Africa, 47.9% (145 cases), followed by Asia, 46.2% (140 cases), Oceania, 4.6% (14 cases), Central and South America, 1.0% (3 cases) and unknown areas, 0.3% (I case), respectively. From 2006 to 2009, a total of 215 cases of exotic malaria were reported in Japan. Among them, P.falciparum and P. vivax were by far the most common infecting malaria, being responsible for 90.2% (194 cases) of the cases. Most cases were from Africa, 56.7% (122 cases), followed by Asia, 26.5% (57 cases), Oceania, 10.2% (22 cases), Central and South America, 3.3% (7 cases) and unknown areas, 3.3% (7 cases), respectively.
Key words: Exotic malaria, Epidemic aspects, Korea and Japan
Received: February 12, 2011, Accepted: March 27, 2011
Correspondence: Won-Chang Lee, College of Veterinary Medicine, Konkuk University, 1 Hwayang-dong, Gwangjin-gu, Seoul 143-476, Korea
Tel: 02-456-1185
E-mail: [email protected]
I. INTRODUCTION
Malaria is one of the most lethal protozoan disease and a
dominant public health concern in more than 100 nations, and
is caused by one or more of four species of Plasmodium (i.e.,
P. vivax, P. falciparum, P. ovale, and P. malariae) that can infect
humans, while other Plasmodium species infect animals. The
infection is transmitted by the bite of an infected female
Year Korea Japan Domestic cases (IR) Exotic cases (IR) Total cases (IR) Exotic cases (IR) 2002
2003 2004 2005 2006 2007 2008 2009 Average IR
1,763 (3.70) 1.107 (2.31) 826 (1.71) 1,324 (2.74) 2,021 (4.17) 1,799 (4.52) 1,017 (2.09) 1,317 (2.71)
(2.99)
36 (0.08) 64 (0.13) 38 (0.08) 45 (0.09) 30 (0.06) 35 (0.07) 29 (0.06) 26 (0.05) (0.08)
1,799 (3.78) 1.171 (2.44) 864 (1.79) 1,369 (2.83) 2,051 (4.23) 2,227 (4.60) 1,046 (2.15) 1,343 (2.75)
(3.12)
83 (0.07) 78 (0.06) 75 (0.06) 67 (0.05) 62 (0.05) 52 (0.04) 56 (0.04) 59 (0.05) (0.05) Abbreviation: IR, Incidence rate per 100,000 populations.
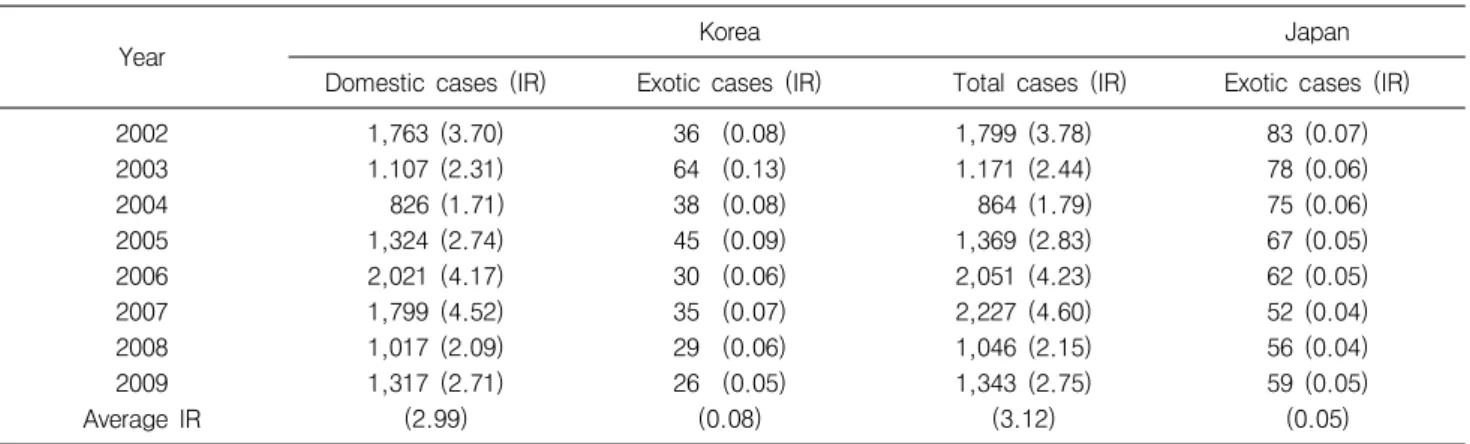
Table 1. Comparison of incidence rate of malaria between Korea and Japan, 2002∼2009
Anopheles species mosquito [1]. Malaria remains a devastating global problem, with an estimated 350∼500 million cases occurring annually [2].
Indigenous malaria has been successfully eradicated in North America, Europe, and a few other previously endemic locations.
Extensive antimalarial programs, improvement of health care service, and advances in socioeconomic development have all contributed to the significant achievements in eradicating the disease in this century [3].
In Korea, no domestic case of malaria has been reported from 1980 to 1992. However, since 1993, the infection of a military personnel in the demilitarization (DMZ) area in Gyeonggi and Gangwon province which lies in the north part of Seoul city in the Korean peninsula, a number of malaria cases has begun to emerge by far, P. vivax has been the most common type of malaria, prevailing in 97.5% of domestic cases [4].
On the other hand, in Japan, indigenous malaria was declared to be eradicated in 1961 and now only imported malaria cases are encountered [5,6]. Nevertheless, a new malaria transmission pattern is increasingly seen in Korea and Japan. Increasing travel to tropical areas where malaria is still in active existence is responsible for emergence of imported malaria in developed countries where malaria has been no more concern. In fact, imported malaria has been an increasing problem in Korea and Japan in the last two decades, now representing the main risk for travelers visiting tropical and sub-tropical countries where malaria is endemic [7].
The present study analyzes all of the malaria cases reported in Korea and Japan during 2002∼2009 in order to assess the trend of prevalence rates over the time and to review risk factors for travelers visiting malaria endemic areas.
II. MATERIALS AND METHODS
1. Surveillance data of malaria in Korea and Japan
The raw data on confirmed domestic and exotic malaria cases in Korea were obtained from the Annual Reports of Malaria in the Disease Web Statistics System 2002∼2009 and the Korea Center for Disease Control and Prevention (KCDCP) [8]. Data pertaining to Japan were obtained from the Surveillance Data of Malaria, 2002∼2009, The Infectious Disease Surveillance Center (IDSC), and the National Institute of Infectious Disease in Japan [9].
2. Statistical analysis
To better quantify the impact of malaria on health in Korea and Japan, we compiled and analyzed information regarding the incidence rate, and the frequency rate in percentage of related risk factors including the distribution of the species of malaria imported by travelers, and related visiting areas. The statistical calculated of incidence rate of malaria per 100,000 populations between Korea and Japan and estimating 95%
confidence intervals (95% CI). The Chi-square test (χ
2-test) was also used to compare the frequency distribution data.
Results were considered to be statistically significant at P<0.05
or P<0.01.
Species Korea Japan
Cases (%) 95% CI Cases (%) 95% CI
P. falciparum 124 (40.9) 35.4∼46.3 264 (49.9)* 45.6∼54.2
P. vivax 109 (36.0) 30.6∼41.4 212 (40.1) 35.9∼44.3
P.f. + P.v. 10 (3.3) 1.3∼5.3 - -
P. ovale 4 (1.3) - 26 (4.9)† 3.1∼6.7
P. malariae 7 (2.3) 1.0∼3.0 10 (1.9) 0.8∼2.7
Unknown 49 (16.2)† 12.0∼20.3 17 (3.2) 1.7∼4.7
Total 303 - 529 -
Abbreviation: 95% CI, confidence intervals 95%.
Chi-square analysis a significant difference from the total value.
*
P
<0.05, †P
<0.01.Table 2. Comparison of exotic malaria cases between Korea and Japan, 2002∼2009
Species of malaria Africa Asia Oceania America Unknown Total (%)
P. falciparum 97 24 3 0 0 124 (40.9)
P. vivax 19 80 7 2 1 109 (36.0)
P.f. + P.v. 3 5 1 1 0 10 (3.3)
P. ovale 2 2 0 0 0 4 (1.3)
P. malariae 5 2 0 0 0 7 (2.3)
Unknown 19 27 3 0 0 49 (16.2)
Total (%) 145 (47.9) 140 (46.2) 14 (4.6) 3 (1.0) 1 (0.3) 303
Raw data modified from KCDCP in Korea, 2002∼2009.
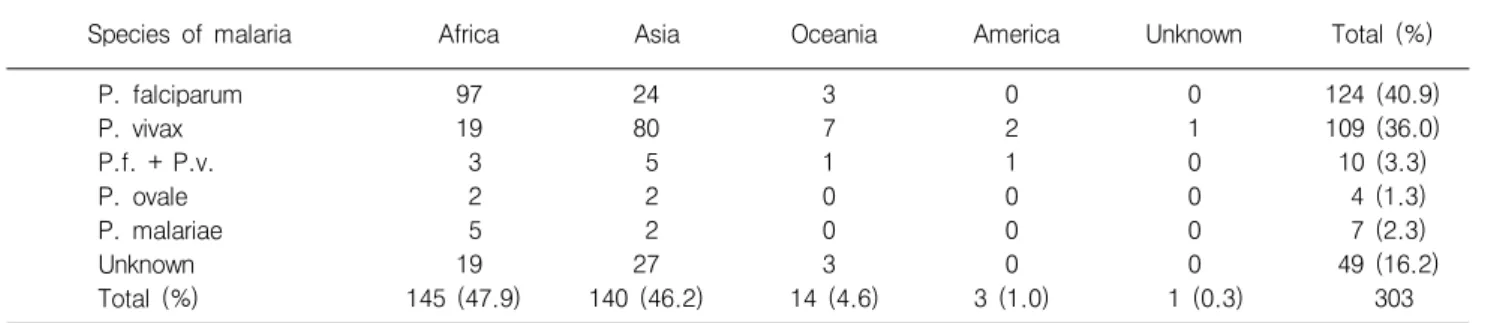
Table 3. Reported cases of malarias in Korea imported by travelers from the suspected endemic area
III. RESULTS AND DISCUSSION
Malaria that affected Koreans belongs to one of two main groups. The first group is Plasmodium vivax malaria, which emerged in Korea in 1993. The second is imported malaria by travelers, and has been increasing in Korea in the last two decades, representing the main risk for travelers visiting malarious countries.
Table 1 shows the incidence rate of malaria, including exotic cases in Korea and Japan from 2002 to 2009. The domestic cases of Plasmodium vivax malaria in Korea involved 11,573 cases during 2002 and 2009. The average incidence rate was 2.99 per 100,000 populations and that of malaria imported by travelers in the exotic case was 0.08 with a variation of 0.05 to 0.13. By region, incidence of domestic malaria was highest in vicinities such as Gyeonggi, Gangwon, Incheon and Seoul, respectively. Percentage of the victims of domestic malaria cases who were civilians including farmers, soldiers or veterans were 55.3%, 21.0% and 23.7%, respectively [8]. During the same
period in Japan, the incidence rate of exotic malaria cases showed an average of 0.05 with a variation of 0.05 to 0.07.
The incidence rate in Korea was slightly higher than that in Japan.
These significant differences between the two countries can be explained on the basis of the differences in their epidemics pattern of domestic and exotic malaria cases imported by travelers [4,8], while the majority of malaria infections in Japan occur among persons who have traveled to and from areas with ongoing malaria transmission. In fact, the total number of patients with acute malaria in Japan has been around 100∼
150 annually for the past two decades. Of those, about 75%
are Japanese and 25% are foreigners [6]. Table 2 shows comparative observation of the distribution of the Plasmodium species of exotic malaria cases between Korea and Japan. From 2002 to 2009 a total of 303 persons were diagnosed with exotic malaria in Korea. One hundred twenty four (40.9%) of the 303 cases were infected with P. falciparum, while 36.0%
(109 cases) were diagnosed with P. vivax, 36.0% (109 cases)
with P. vivax and P. falciparum mixed, 3.3% (10 cases), with
P. ovale, 1.3% (4 cases), with P. malariae, 2.3% (7 cases) or
Species of malaria Africa Asia Oceania America unknown Total (%)
P. falciparum 100 13 5 0 2 120 (55.8)
P. vivax 7 40 16 7 4 74 (34.4)
P. ovale 7 0 0 0 1 8 (3.7)
P. malariae 3 0 0 0 0 3 (1.4)
Unknown 5 4 1 0 0 10 (4.7)
Total (%) 122 (56.7) 57 (26.5) 22 (10.2) 7 (3.3) 7 (3.3) 215
Raw data modified from IASR in Japan, 2006∼2009.
Table 4. Reported cases of malarias in Japan imported by travelers from the suspected endemic areas
16.2% (49 cases) with unknown cases. During the same period in Japan, the percentages of the 529 persons infected with P.
falciparum, P. vivax, P. ovale, P. malariae and unknown cases were 49.9% (264 cases), 40.1% (212 cases), 4.9% (26 cases), 1.9% (10 cases) and 3.2% (17 cases), respectively. Notably, the risk rates of P. falciparum and P. ovale in Japan were much higher than in Korea (P<0.05 and P<0.01). These data strongly indicate that the exotic malaria incidence is influenced by their travel areas [7,10].
A total of 303 cases were reported with exotic malaria imported by travelers in Korea during 2002 to 2009 (Table 3). P. falciparum and P. vivax were by far the most common infectious protozoa, forming 76.9% (233 cases) of the 303 cases. P. falciparum was the predominant pathogen from Africa (97 versus 19 cases of P. vivax), while P. vivax was the leading parasite in cases from Asia (80 versus 24 cases of P. falciparum).
In case of exotic malaria were contracted in Africa zone, 47.9%
(145 cases) of 303 cases, followed by Asia’s 46.2% (140 cases), Oceania’s 4.6% (14 cases), Central and South America’s 1.0%
(3 cases) and unknown 0.3% (1 case), respectively. Of these, falciparum malaria and vivax malaria occur frequently than others do. Falciparum malaria tends to develop complications such as encephalopathy, acute renal failure, pulmonary edema/acute respiratory distress syndrome (ARDS), dissemi- nated intravascular coagulation syndrome (DICS)-like bleeding tendency, and sometimes death. Also, its drug resistance is an encountering problem [11]. On the other hand, from 2006 to 2009, a total of 215 cases were reported with exotic malaria imported by travelers in Japan from the suspected areas listed in Table 4. P. falciparum and P. vivax were by far the most common infecting malaria, forming 90.2% (194 cases) of the 215 cases. P. falciparum was the predominant pathogen in those coming from Africa (100 versus 7 cases of P. vivax), while P.
vivax was the leading protozoan in cases in Asia (40 versus 13 cases of P. falciparum). Notable, most cases were from Africa, 56.7% (122 cases), followed by Asia, 26.5% (57 cases),
Oceania, 10.2% (22 cases), Central and South America, 3.3%
(7 cases) and unknown areas, 3.3% (7 cases), respectively. On the other hand, the suspected areas of infection were analyzed by causative Plasmodium species. As for falciparum malaria, Africa accounted for 83.3% (100 cases), followed by Asia 10.8% (13 cases), Oceania’s 4.2% (5 cases) and unknown areas 1.7% (2 cases). As for vivax malaria, Asia accounted for 54.1%, (40 cases), followed by Oceania’s 21.6% (16 cases), Africa’s 9.5% (7 cases), Central and South America’s 9.5% (7 cases) and unknown 5.4% (4 cases), respectively. Ovale and malariae malaria cases were very few in numbers; only 7 cases of ovale and 3 cases of malariae were recorded to be originated from Africa among exotic cases.
While many Korean and Japanese people travel to Asian countries where malaria risk is limited, the number of those visiting highly malaria-endemic areas like sub-Saharan Africa or Oceania is steadily increasing. Consequently, counter- measures against a possible increase in the number of malaria cases, especially that falciparum malaria case in the future, should become a priority [4,12-14].
In conclusion, many Korean and Japanese travelers are unaware of diseases in the countries they visit, and do not adequately protect themselves. Careful attention to avoid contact with mosquitoes is very important to avoid malaria infection, but not easy to do. No practical method of immunization is available yet. Various types of chemo- prophylaxis agents for malaria have been used for a long time with respectable success [13-15]. To implement effective education measure against imported malaria, evaluation of infection risks based on the incidence rates of malaria per given number of travelers to each area/country is warranted.
REFERENCES
1. Thwing J, Skarbinski J, Newman RD, Baeber AM, Mali S,
Robert JM, et al. Malaria Surveillance-United States, 2005.
Morbidity and Mortality Weekly Report (MMWR) 2007;56:23-40.
2. Guinovart C, Navia MM, Tanner M and Alonso PL. Malaria:
burden of disease. Curr Mor Med 2006;6:137-140.
3. Dan M, Costin C and Slater E. Malaria imported by traveler: The Israeli Experience. J Travel Med 1996;3:182-185.
4. KCDCP. Epidemiology of Malaria in Korea 2005. Communicable Disease Monthly Report. Korea Center for Disease Control and Prevention (KCDCP) 2006;17:1-11.
5. Miura T, Kimura M, Koibuchi T, Endo T, Nakamura H, Odawara T, et al. Clinical Characteristics of imported malaria in Japan: Analysis at a referral hospital. Am J Trop Med Hyg 2005;73:
599-603.
6. Kano S and Kimura M. Trends in malaria cases in Japan. Acta Trop 2004;89:271-278.
7. KCDCP. The Control Index of Malaria in Korea. Korea Center for Disease Control and Prevention (KCDCP) 2010;47-52.
8. KCDCP. Disease web statistics system, 2002-2009. Korea Center for Disease Control and Prevention (KCDCP). http://www.cdc.go.kr/
kcdchome.
9. Infectious Disease Surveillance Center (IDSC), National Institute of
Infectious Disease in Japan (2002-2009) Surveillance Data (web system): Online at IDSC <http://idsc.nih.go.jp/idwr/ydata/report- Ea.html>.
10. Mizuno Y and Kudo K. Travel-related health problems in Japanese travelers. Travel Med Infect Dis 2000;7:296-300.
11. NIIDIDCD. National Institute of Infectious Disease and Infectious Diseases Control Division (NIIDIDCD), Ministry of Health and Welfare. Malaria, Japan, April 1999-2006. Infect Agents Surveillance Rep 2007;28:1-2.
12. Kimura M, Yasuharu A, Matsumoto Y, Naksjima K, Wataya Y and Ohtomo H. Epidemiological and Clinical Aspects of Malaria in Japan. J Treavel Med 2003;10:122-127.
13. Infectious Disease Surveillance Center (IDSC), Malaria, Japan, April 1999-2005. Infectious Agents Surveillance Report 2007;28:1-2.
14. Cheong HS, Kwon KT, Rhee JY, Ryu SY, Heo SY, Chung KR, et al. Imported Malaria in Korea: a 13-Year Experience a Single Center. Korean J Parasitol 2009;47:299-302.
15. Center for Disease Control and Prevention (CDC). MALARIA; Chapter 2 the Pre-Travel Consultation Malaria. CDC, July 2, 2010.
http://www.cdc.gov/travel/yellobook/2010/chapter-2/malaria.aspx.
=국문초록=