Tuberc Respir Dis 2013;74:274-279
CopyrightⒸ2013. The Korean Academy of Tuberculosis and Respiratory Diseases. All rights reserved.
A Case of Pulmonary Sarcoidosis with Endobronchial Nodular Involvement
Kyung Hwa Cho, M.D.1, Jeong Hyun Shin, M.D.1, Seong Hoon Park, M.D.2, Heon Soo Kim, M.D.3, Sei Hoon
Yang, M.D.1
Departments of 1Internal Medicine, 2Radiology, and 3Pathology, Wonkwang University College of Medicine, Iksan, Korea
Sarcoidosis is a multisystemic disorder of unknown cause that is characterized pathologically by noncaseating granulomas. Diagnosis is based on the exclusion of other infectious, interstitial, and neoplastic diseases and on the typical pathology. Although the lungs and mediastinal lymph nodes are almost involved, endobronchial nodular lesions of sarcoidosis with lung involvements are rare. We report a case of sarcoidosis with lung involvements and endobronchial nodules as confirmed by bronchial biopsy.
Key Words: Sarcoidosis; Bronchi; Biopsy
Address for correspondence: Sei Hoon Yang, M.D.
Department of Internal Medicine, Wonkwang University
Hospital, Wonkwang University College of Medicine, 895
Muwang-ro, Iksan 570-749, Korea
Phone: 82-63-859-2582, Fax: 82-63-855-2025
E-mail: [email protected]
Received: Sep. 4, 2012
Revised: Sep. 24, 2012
Accepted: Oct. 23, 2012
CCIt is identical to the Creative Commons Attribution Non-Commercial
License (http://creativecommons.org/licenses/by-nc/3.0/).
Introduction
Sarcoidosis is a cryptogenic general granulomatosis that typically affects adults up to 50 years of age.
Sarcoidosis infiltrates all organs, particularly the bilateral hilar lymph nodes, lungs, peripheral lymph nodes, skin, eyes, liver, and spleen
1. Boek first used the term 'sar- coid' in 1899 in regard to a condition of multiple tumors and rashes. In Korea, sarcoidosis has occurred in ap- proximately 0.13 out of 100,000 individuals since the first case was reported here in 1984 (The 2nd Nation- wide Actual Condition Survey, 2000), but it has recently been on an increasing trend
2. The clinical symptoms of sarcoidosis are usually nonspecific and generalized, and include fever, fatigue, anorexia, weight loss, and mala- ise. The symptoms vary depending upon the organs that
are infiltrated. Given that sarcoidosis mostly infiltrates the lungs, respiratory symptoms such as exertional dyspnea, cough, and chest pain are observed in most cases
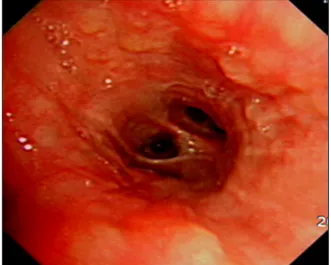
3. In our experience, it is rare that sarcoidosis nod- ularly infiltrates the bronchus. This is a report of a case of endobronchial nodular sarcoidosis diagnosed by bronchoscopy and a biopsy.
Case Report
A 42-year-old Indian male who was employed as an automotive engineer was referred to our hospital with complaints of a month-long fever and cough. The pa- tient had been diagnosed with pulmonary tuberculosis 5 years previously in India, and he had returned from Thailand a month before visiting our hospital complain- ing of fever, persistent cough, and general malaise.
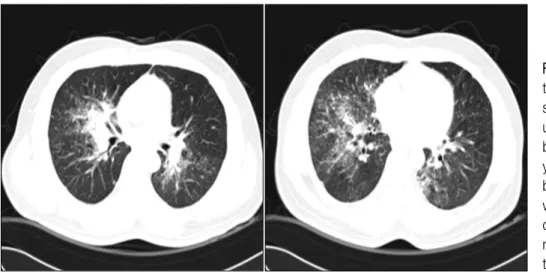
Before he was referred to our center, he had undergone
computed tomography (CT) at another hospital because
his symptoms had persisted even after medical treat-
ment, whereon abnormalities had been detected. As
noted, the patient had been previously diagnosed with
pulmonary tuberculosis by positive mycobacterium tu-
berculosis culture in April 2003, in India. He completed
a 7-month course of anti-tuberculosis medications was
completely recovered, and he had no history of dia-