149
Address for correspondence: In Jae Oh, M.D.
Department of Ineternal Medicine, Chonnam National University Medical School, 671, Jebong-ro, Dong-gu, Gwangju 501-757, Korea
Phone: 82-61-379-7617, Fax: 82-61-379-7619 E-mail: [email protected]
Received: Jan. 5, 2008 Accepted: Jan. 24, 2008
일측성 폐침윤을 보인 폐포양 유육종증 1예
전남대학교 의과대학 내과학교실
김희경, 반희정, 지수영, 채동렬, 조계중, 임정환, 주진영, 권용수, 오인재, 김규식, 김유일, 임성철, 김영철
A Case of Pseudoalveolar Sarcoidosis with Unilateral Pulmonary Infiltration
Hee Kyung Kim, M.D., Hee Jung Ban, M.D., Su Young Chi, M.D., Dong Ryeol Chae, M.D., Gye Jung Cho, M.D., Jung Hwan Lim, M.D., Jin Yung Ju, M.D., Yong Soo Kwon, M.D., In Jae Oh, M.D., Kyu Sik Kim, M.D., Yu Il Kim, M.D., Sung Chul Lim, M.D., Young Chul Kim, M.D.
Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea
A sarcoidosis is a multisystemic granulomatous disorder that has a predilection for pulmonary involvement, and the common radiological findings for the disease are bilateral nodular or reticulonodular patterns. Pseudoalveolar sarcoidosis is a rare presentation of sarcoidosis. The radiological finding is an alveolar pattern that involves or compresses the alveoli by clustered interstitial granuloma. A 58-year-old man was admitted due to incidental findings of a unilateral consolidative lesion as seen on chest radiography. A chest computed tomography (CT) examination showed multiple bronchoalveolar consolidations that were suspicious of a malignancy. However, a percutaneous needle biopsy revealed non-caseating granuloma with an asteroid body that was compatible with sarcoidosis. After one month, the consolidative lesions improved without any treatment. (Tuberc Respir Dis 2008;64:149-152)
Key Words: Pseudoalveolar, Sarcoidosis, Unilateral
서 론
유육종증은 원인 불명의 전신성 질환으로, 양측 폐문 림프절 비대를 동반한 폐 침윤 소견 및 안 침범, 피부 침범 을 특징적으로 보이는 질환으로 침범 부위의 조직검사에 서는 비건락성 육아종 소견이 관찰된다.
폐포양 유육종증은 간질의 육아종들이 융합하여 주변 폐포를 누르거나 폐포강을 침범하여 방사선학적으로 ‘폐 포’ 병변을 이루는 병변으로 유육종증의 매우 드문 형태이 다1-5. 특히 일측성 폐침윤을 보이는 폐포양 유육종증은 국 내에서 현재까지 1예만이 보고되었다6.
본 저자들은 일측성 폐침윤 소견으로 내원하여 시행한 조직검사 등에서 유육종증으로 진단된 폐포양 유육종증
1예를 경험하였기에 문헌 고찰과 함께 보고하는 바이다.
증 례
환 자: 박○○, 58세 남자
주 소: 우연히 발견된 일측성 폐침윤
과거력 및 가족력: 4년 전 당뇨병과 고혈압을 진단 받고 약물 치료 중이었으며, 7년 전 좌측 신세포암으로 좌측 신 제거술을 시행하였으며 현재까지 재발하지 않은 상태임 사회력: 15갑년의 흡연력이 있었으며 1년 전부터 금연 현병력: 평소 호흡 곤란이나 기침, 가래, 흉부 불쾌감 등의 호흡기 증상이나, 체중감소, 전신 쇠약감 등의 증상 은 없었던 환자로, 건강검진을 위해 시행한 단순 흉부 방 사선 촬영에서 비정상 폐침윤이 발견되어 이에 대한 검사 를 위하여 내원
이학적 소견: 내원 당시의 활력징후는 혈압 135/70 mmHg, 맥박 55회/분이었으며, 호흡수 13회/분, 체온은 36.4oC였다. 두경부 진찰상 특이 소견은 없었고 청진상 특이 소견은 없었다.
검사실 소견: 말초 혈액 검사상 혈색소 12.6 g/dl, 백혈
HK Kim et al: A case of pseudoalveolar sarcoidosis with unilateral pulmonary infiltration
150
Figure 2. (A, B) Initial chest HRCT scans shows a mass-like opacity in the superior and posterobasal segment of the right lower lobe. (C, D) Follow-up chest HRCT (4 months later) scans shows a resolution of previous lesions in the superior and posterobasal segment of the right lower lobe.
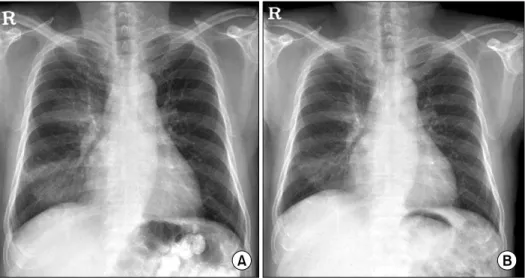
Figure 1. (A) Initial chest X-ray shows a consolidation of the right lower lung field. (B) A follow-up chest X-ray (1 month later) shows a partial resolution of consolidation of the right lower lung field.
구 9,900/mm3 (호중구 70%, 림프구 21.2%), 혈소판 357,000/
mm3이었고, 혈청 생화학 검사상 총단백 7.1 g/dl, 알부민 4.3 g/dl, AST/ALT 21/27 U/L, BUN/Cr 18.3/1.1 mg/dl, 총칼슘 4.6 mEq/L이었다. CEA 2.84 ng/mL, 혈청 안지오 텐신 전환효소(ACE)는 7.0 U/L로 정상 범위였으며, ANA, ANCA, RA factor, anti-HIV Ab 모두 음성이었다.
결핵 피부 반응 검사 및 객담 배양 검사는 음성이었다.
폐기능 검사 소견: FVC 3.14 L (예측치의 84%), FEV1
2.50 L (예측치의 91%), FEV1/FVC 79%, DLCO 17 ml/
mmHg/min (예측치의 85%)로 정상 소견을 보였다.
방사선 소견: 내원 시 단순 흉부 촬영(Figure 1A) 및 흉부 전산화 단층 촬영(Figure 2A, B)에서 우하엽 경결
Tuberculosis and Respiratory Diseases Vol. 64. No. 2, Feb. 2008
151 Figure 3. The pathologic findings of transthoracic needle biopsy reveals (A) chronic non-caseatng granulomatous in- flammation and giant cell (H&E stain, ×200). (B) In high power field, there is a asteroid body (white arrow) in giant cell (H&E stain, ×400).
소견이 관찰되었고, 이는 폐렴 또는 세기관지 세포암이나 전이암이 의심되었다.
기관지내시경 및 병리 소견: 세균학적 검사를 위한 검 체물 채취와 조직 검사를 위해서 기관지 내시경을 시행하 였다. 기관지 세척액 배양검사와 조직검사상 특이소견은 보이지 않아, 우하엽의 경결 부위에서 경흉부 세침 생검을 추가 시행하였다. 세침 생검 조직검사상 별모양 소체 (asteroid body)를 포함한 만성 비괴사성 육아종성 염증소 견(Figure 3)이 관찰되었고 이는 유육종증에 합당한 소견 으로 판단되었다.
임상경과: 방사선 소견 및 조직 검사 소견을 종합하여 환자는 유육종증의 드문 발현 형태인 폐포양 유육종증으 로 진단하였다.
환자는 호흡기 증상이나 신경계나 심장을 침범한 증상 이 없었고, 혈액 검사, 심전도 및 안과 검진상 이상 소견이 관찰되지 않아 진단 후 바로 스테로이드 투약 등의 치료를 시행하지 않았다. 정기적인 외래 방문을 통하여 증상의 발현 여부를 확인하면서 단순 흉부 방사선 촬영을 하였다.
외래 추적에서 증상의 발현은 없었으며, 1개월 후 시행한 단순 흉부 방사선 촬영(Figure 1B)과 4개월 후 시행한 흉 부 전산화 단층 촬영(Figure 2C, D)상 이전에 관찰되었던 우폐야의 폐침윤은 호전되는 양상을 보이고 있다.
고 찰
유육종증은 침범 장기에 따라 다양한 증상을 보일 수 있으나, 90% 이상 환자에서 폐침윤이 동반되므로 전형적
으로 건성 기침, 운동 시 호흡 곤란 등의 호흡기 증상을 보인다. 그러나 30∼60%의 환자에서는 증상 없이 흉부 방사선 촬영에서 이상 소견을 보이기도 한다7.
유육종증의 전형적인 흉부 방사선 소견은 양측 폐 상엽 의 결절과, 양측 흉곽 내 임파선 비대가 특징적인 소견이 나, 임파선 비대가 없거나 비전형적인 유육종증의 폐 침윤 소견을 보이는 경우 임상 증상 및 방사선 소견만으로는 다른 폐질환과 감별이 힘들다8.
폐포양 유육종증은 흉부 전산화 단층 촬영상 양측성 다 발성의 폐 주변부나 기관지-혈관 다발 주변에 위치한 불규 칙한 경계를 가진 진한 균질 음영 또는 불균질한 음영과 이에 동반된 병변의 주변부나 주위 폐의 미세결절 소견을 보이는 것으로6, 작은 결절들이 융합하여 불분명한 경계를 갖는 음영을 형성하여 폐포 경결과 감별하기 힘들어 방사 선학상으로 본 증례와 같이 폐렴이나 폐암과의 감별이 어
렵다2-5,9. 국내의 경우 폐포양 유육종증은 매우 드물게 발
견되고 있고 발견되는 경우도 대부분 양측성 폐침윤 소견 을 보이며, 일측성 폐침윤을 보이는 경우는 현재까지 1예 만이 보고되었다6.
유육종증의 임상 증상 및 방사선학적 소견은 비특이적 인 경우를 보일 수 있어 가장 명확한 진단 방법은 조직학 적 검사이다9. 조직 소견은 상피양 세포나 랑게르한스 세 포 또는 거대세포의 응집으로 이루어진 비괴사성 육아종 이 특징적이며, 약 60%에서 거대세포내 별모양소체(aste- roid body)를 관찰할 수 있다.
유육종증의 약 40%는 자연 치유되는 경과를 보이며, 약 40%에서는 치료가 지연되더라도 치료에 반응하는 경
HK Kim et al: A case of pseudoalveolar sarcoidosis with unilateral pulmonary infiltration
152
과를 보인다고 알려져 있다. 중증의 안구, 신경계 또는 심 장을 침범한 유육종증, 중증의 고칼슘 혈증, 진행성 2기의 폐질환, 증상이 있는 2기의 폐질환과 3기의 폐질환등에서 는 초기 스테로이드나 methotrexate 사용을 권장하며 이 러한 징후가 없는 경우 6개월 정도 치료 없이 관찰하는 것을 권장한다10,11.
본 증례는 내원 당시 증상이나 방사선 소견상 폐렴, 폐암 또는 과거 신세포암 병력으로 전이암이 의심되었던 환자이나 혈액 검사나 객담과 기관지 내시경을 통해서 얻은 검체의 도말, 배양검사 및 세포검사상 육아종성 염 증을 초래할 만한 원인 질환이 발견되지 않았고, 경흉부 세침 생검상 유육종증에 합당한 소견을 보였다. 방사선 학적으로 비전형적인 소견을 보이는 경우 유육종증의 진 단이 늦어져 중요 장기를 침범하여, 진행성 다발성 장기 부전이 초래되는 경우도 보고되고 있어 초기 적절한 진 단이 필요하다. 본 환자의 경우 타장기 침범 소견이 없었 고 증상 역시 없었기 때문에 치료 없이 추적관찰 하였고 1개월 이후에 초기 병변은 흉부 방사선 추적검사에서 호 전되었다.
요 약
유육종증은 원인 불명의 전신성 질환으로 폐 침윤은 양 측 폐 상엽의 결절과, 양측 흉곽내 임파선 비대가 특징적 이나 폐포 병변을 보여 폐렴이나 폐암으로 오인될 수 있는 일측성 폐포양 유육종증은 드문 것으로 알려져 있어 문헌 고찰과 함께 보고하는 바이다.
참 고 문 헌
1. Johkoh T, Ikezoe J, Takeuchi N, Kohno N, Tomiyama
N, Akira M, et al. CT findings in "pseudoalveolar"
sarcoidosis. J Comput Assist Tomogr 1992;16:904-7.
2. Muller NL, Mawson JB, Mathieson JR, Abboud R, Ostrow DN, Champion P. Sarcoidosis: correlation of extent of disease at CT with clinical, functional, and radiographic findings. Radiology 1989;171:613-8.
3. Sahn SA, Schwarz MI, Lakshminarayan S. Sarcoidosis:
the significance of an acinar pattern on chest roentgenogram. Chest 1974;65:684-7.
4. Grenier P, Valeyre D, Cluzel P, Brauner MW, Lenoir S, Chastang C. Chronic diffuse interstitial lung disease:
diagnostic value of chest radiography and high-reso- lution CT. Radiology 1991;179:123-32.
5. Battesti JP, Saumon G, Valeyre D, Amouroux J, Pechnick B, Sandron D, et al. Pulmonary sarcoidosis with an alveolar radiographic pattern. Thorax 1982;37:
448-52.
6. Nam JE, Ryu YH, Park JG, Choe KO, Im JG, Lee KS, et al. High resolution CT findings of pseudoalveolar sarcoidosis. J Korean Radiol Soc 2002;47:191-6.
7. Hamper UM, Fishman EK, Khouri NF, Johns CJ, Wang KP, Siegelman SS. Typical and atypical CT manifes- tation of pulmonary sarcoidosis. J Comput Assist Tomogr 1986;10:928-36.
8. Sharma OP. Sarcoidosis: a worldwide phenomenon.
Sarcoidosis 1984;1:11-5.
9. Brauner MW, Grenier P, Mompoint D, Lenoir S, de Cremoux H. Pulmonary sarcoidosis: evaluation with high resolution CT. Radiology 1989;172:467-71.
10. Gibson GJ, Prescott RJ, Muers MF, Middleton WG, Mitchell DN, Connolly CK, et al. British Thoracic Society Sarcoidosis study: effects of long term cortico- steroid treatment. Thorax 1996;51:238-47.
11. Newman LS, Rose CS, Maier LA. Sarcoidosis. N Engl J Med 1997;336:1224-34.