DOI: 10.4174/jkss.2011.80.4.272
ORIGINAL ARTICLE
Journal of the Korean Surgical Society
JKSS
pISSN 2233-7903ㆍeISSN 2093-0488
Received August 12, 2010, Accepted November 1, 2010 Correspondence to: Selcuk Mevlut Hazinedaroglu
Department of Surgery, Ankara University Medical Faculty, 737. Sok. No:4, 4B-3, Ege Botanik Konutları, 06550, Cankaya, Ankara, Turkey Tel: +90-312-5082435, Fax: +90-312-3093989, E-mail: [email protected]
cc Journal of the Korean Surgical Society is an Open Access Journal. All articles are distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Multiple renal arteries challenge in laparoscopic donor nephrectomy: how far can we go?
Volkan Genc, Ahmet Serdar Karaca, Erkinbek Orozakunov, Atil Cakmak, Yusuf Sevim, Evren Ustuner
1, Derya Oztuna
2, Selcuk Mevlut Hazinedaroglu
Departments of Surgery, 1Radiology, and 2Biostatistics, Ankara University School of Medicine, Ankara, Turkey
Purpose: Living donor kidneys with multiple arteries are routinely procured laparoscopically. We aim to present our experi- ence with laparoscopic donor nephrectomy (LDN) and to compare the graft function and outcome between cases with single versus multiple arteries. Methods: We compared the demographic data, operation time, warm ischemia time, rejection rate, and graft function between LDN kidneys with single artery and those with multiple arteries. Results: Seventy-three cases with 1 renal artery (group LDN-1), 8 cases with 2 renal arteries (group LDN-2) and 5 cases with 3 or more renal arteries (group LDN-3) were included in the study. The mean operative time was significantly higher in groups LDN-2 (100.3 ± 9.5 minutes) and LDN-3 (120.6 ± 10.3 minutes) compared to group LDN-1 (75.7 ± 10 minutes, P < 0.001). Similar results were de- tected with respect to the warm ischemia time. There were no statistically significant differences related to graft function and outcome among these groups. Conclusion: Multiple renal arteries present a special challenge in both donor nephrectomy and renal transplantation. However, laparoscopic procurement of a kidney with multiple renal arteries, regardless of the number, is reliable and has no significant impact on the graft outcome.
Key Words: Laparoscopic, Nephrectomy, Graft rejection, Multiple, Renal artery
INTRODUCTION
Laparoscopic donor nephrectomy (LDN) has become the gold standard in many kidney transplant centers. The shortfall of available organs for patients awaiting kidney transplant grows continuously. LDN may increase the number of kidneys available for transplantation while minimizing the morbidity and expediting the recovery of potential donors.
Since the first report of laparoscopic live donor neph- rectomy in 1995 [1], graft outcome has been the primary
theme in research literature. On the other hand, to max- imize the available donor pool, organs with multiple ar- teries were included in the scenario with the expectation of similar graft outcome in comparison to single artery organs. In the present study, we aim to present our experi- ence with LDN and to compare the outcomes when pro- curing kidneys with single versus multiple renal arteries.
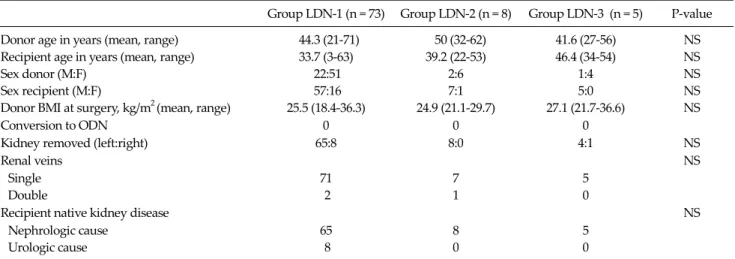
Table 1. Demographic data of the three groups
Group LDN-1 (n = 73) Group LDN-2 (n = 8) Group LDN-3 (n = 5) P-value
Donor age in years (mean, range) 44.3 (21-71) 50 (32-62) 41.6 (27-56) NS
Recipient age in years (mean, range) 33.7 (3-63) 39.2 (22-53) 46.4 (34-54) NS
Sex donor (M:F) 22:51 2:6 1:4 NS
Sex recipient (M:F) 57:16 7:1 5:0 NS
Donor BMI at surgery, kg/m2 (mean, range) 25.5 (18.4-36.3) 24.9 (21.1-29.7) 27.1 (21.7-36.6) NS
Conversion to ODN 0 0 0
Kidney removed (left:right) 65:8 8:0 4:1 NS
Renal veins NS
Single 71 7 5
Double 2 1 0
Recipient native kidney disease NS
Nephrologic cause 65 8 5
Urologic cause 8 0 0
LDN, laparoscopic donor nephrectomy; LDN-1, cases with single renal arteries; LDN-2, cases with two renal arteries; LDN-3, cases with three or more renalarteries; BMI, body mass index; ODN, open donor nephrectomy; NS, not significant.
METHODS
Eighty-six LDNs performed between December 2005 and June 2009 were included in this study. Exclusion cri- teria were hand assisted technique and defective follow up period. All LDN subjects who underwent procedures by the same senior transplant surgeon (SMH) at the Ankara University Hospital and conversion to open sur- gery did not occur in any LDN donors.
Surgical procedures
Before placing the patient in the lateral decubitus posi- tion, the Pfannenstiel incision site was marked. A 10-mm trocar for camera placement was inserted directly in the periumbilical region. Two 5-mm trocars were then placed in the subcostal area. On the right side, a third 5-mm trocar for liver retraction was placed in the subxiphoid region.
Dissection for kidney exposure was performed with har- monic scalpel (Ultracision ACE36P, Ethicon Endo-Surgery Inc., Cincinnati, OH, USA). The gonadal vein on the left side was dissected up to the renal vein together with the ureter. Adrenal and lumbar veins were divided with a har- monic scalpel. The renal artery and vein were skele- tonized. The ureter with surrounding tissue was dissected down to the iliac vessels and divided by using 10-mm tita- nium clips (Ethicon Endo-Surgery). After completing all
dissection procedures, the Pfannenstiel incision was per- formed and a 12-mm trocar was placed in this area for the stapler entrance. Renal artery and renal vein were divided with one angle laparoscopic stapling device (Endo GIA Roticulator; Tyco Healthcare, Hampshire, UK). Thereaf- ter, the peritoneum was transected and the kidney was ex- tracted quickly by hand.
Total operative time of donors was measured as from first incision to last skin suture. Warm ischemia time (WIT) was defined as the time from clamping of renal artery/ar- teries and renal vein/veins with stapler to commencement of cold flushing. If the graft had 2 or more renal arteries, the point of commencement of cold flushing was accepted after the cannulation and perfusion of all arteries.
Donors were divided into three subgroups according to: 1 renal artery (LDN-1), 2 renal arteries (LDN-2), and 3 or more renal arteries (LDN-3). Patient demographics, to- tal operative times, WITs, serum creatinine level at various time points, rejection rate, arterial and venous complica- tions, and graft and patient survival rates were compared among these three groups.
Statistical analysis
Statistical analyses were performed using SPSS ver. 11.5 (SPSS Inc., Chicago, IL, USA). Data were expressed as mean ± standard deviation for metric variables and as fre-
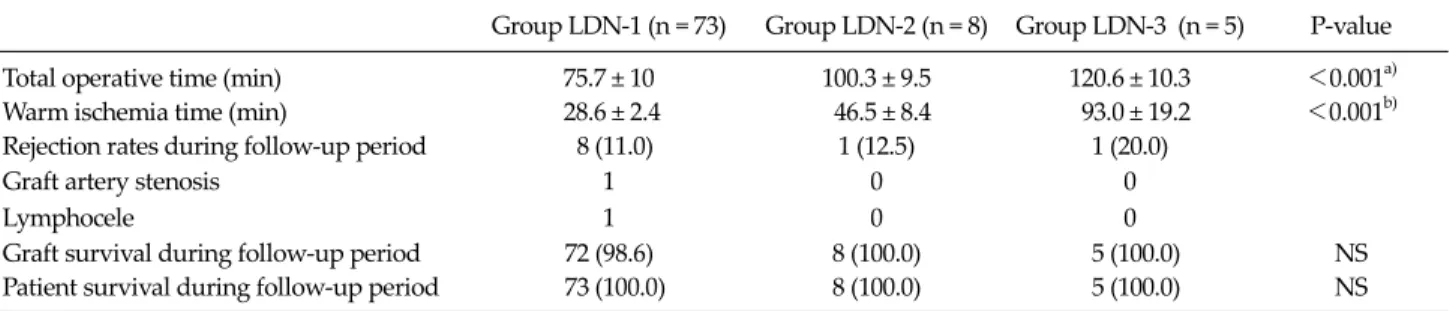
Table 2. Operative data and postoperative outcomes
Group LDN-1 (n = 73) Group LDN-2 (n = 8) Group LDN-3 (n = 5) P-value
Total operative time (min) 75.7 ± 10 100.3 ± 9.5 120.6 ± 10.3 <0.001a)
Warm ischemia time (min) 28.6 ± 2.4 46.5 ± 8.4 93.0 ± 19.2 <0.001b)
Rejection rates during follow-up period 8 (11.0) 1 (12.5) 1 (20.0)
Graft artery stenosis 1 0 0
Lymphocele 1 0 0
Graft survival during follow-up period 72 (98.6) 8 (100.0) 5 (100.0) NS
Patient survival during follow-up period 73 (100.0) 8 (100.0) 5 (100.0) NS
Values are presented as mean ± SD or number (%).
LDN, laparoscopic donor nephrectomy; LDN-1, cases with single renal arteries; LDN-2, cases with two renal arteries; LDN-3, cases with three or more renal arteries; NS, not significant.
a)Multiple comparison tests for all pairwise comparisons. b)Multiple comparison tests for pairwise comparisons except group LDN-2 vs.
group LDN-3.
quency (percentage) for categorical variables. In order to compare the three groups in terms of metric variables, Kruskal-Wallis variance analysis was used, and for catego- rical variables, chi-square test was used. If significant dif- ferences were found, the multiple comparison test was used to determine which groups were different. A value of P < 0.05 was accepted as statistically significant.
RESULTS
Seventy-three cases with 1 renal artery (group LDN-1), 8 cases with 2 renal arteries (group LDN-2) and 5 cases with 3 or more renal arteries (group LDN-3, four cases with 3 renal arteries and one case with 4 renal arteries) were included in this study. Demographic data with re- spect to the three groups are shown in Table 1. The mean ages of LDN-1, LDN-2, and LDN-3 donors were 44.3 years (range, 21 to 71 years), 50 years (range, 32 to 62 years), and 41.6 years (range, 27 to 56 years), respectively. The mean age of recipients was 33.7 years (range, 3 to 63 years) in LDN-1, 39.2 years (range, 22 to 53 years) in LDN-2, and 46.4 years (range, 34 to 54 years) in LDN-3. The gender dis- tribution was similar among groups. Body mass index was similar in LDN-1, LDN-2, and LDN-3 donor groups (P = 0.59). Conversion to open surgery was not necessary in any of the LDN subjects. Right-sided nephrectomy was performed in 8 donors in the LDN-1 group and in 1 donor in the LDN-3 group. Recipient native kidney diseases
were similar among groups.
The operative data, postoperative renal outcome and complications are given in Table 2. The mean total oper- ative time was shorter for the procurement of organs with single arteries (75.7 minutes; range, 60 to 90 minutes) than for organs with 2 arteries (100.2 minutes; range, 82 to 112 minutes) and organs with 3 or more arteries (120.6 mi- nutes; range, 112 to 138 minutes; P < 0.001). Furthermore, the mean WIT was significantly shorter for organs with single arteries (28.62 seconds; range, 22 to 34 seconds) than for organs with 2 arteries (46.5 seconds; range, 36 to 61 sec- onds) and organs with 3 or more arteries (93 seconds;
range, 78 to 126 seconds; P < 0.001). Eleven percent of the LDN-1 group, 12.5% of the LDN-2 group and 20% of the LDN-3 group had an episode of acute rejection within the follow-up period. Lymphocele was detected in one LDN-1 recipient and was treated with surgical intervention.
Renovascular hypertension and partial perfusion defect after transplantation was not seen in any patients. Graft ar- tery stenosis in one LDN-1 recipient was treated with per- cutaneous transluminal balloon angioplasty. The cause of the one graft loss in the LDN-1 group was due to graft ar- tery thrombosis, but there were no significant differences identified among these three groups with respect to graft and patient survivals.
Serum creatinine levels were not statistically significant among these three groups in the preoperative period (P = 0.81) or at postoperative day 1 (P = 0.82), day 2 (P = 0.42), day 5 (P = 0.51), 1 month (P = 0.74), 3 months (P = 0.29), 6
Table 3. Serum creatinine (mg/dL) levels (preoperative and postoperative at various time points)
Group LDN-1
Group LDN-2
Group
LDN-3 P-value Day PO 8.16 ± 3.25 7.65 ± 1.88 8.56 ± 4.88 0.81 Day 1 3.97 ± 1.91 3.48 ± 1.22 3.12 ± 1.41 0.82 Day 2 2.05 ± 1.08 1.73 ± 0.65 1.56 ± 0.31 0.42 Day 5 1.37 ± 0.53 1.35 ± 0.65 1.14 ± 0.29 0.51 1 month 1.21 ± 0.31 1.16 ± 0.36 1.16 ± 0.20 0.74 3 months 1.25 ± 0.36 1.07 ± 0.27 1.11 ± 0.27 0.29 6 months 1.25 ± 0.31 1.02 ± 0.13 1.61 ± 1.05 0.10 12 months 1.24 ± 0.35 0.97 ± 0.13 1.18 ± 0.22 0.09 Values are presented as mean ± SD.
LDN, Laparoscopic donor nephrectomy; LDN-1, cases with single renal arteries; LDN-2, cases with two renal arteries; LDN-3, cases with three or more renal arteries; PO, pre-operative.
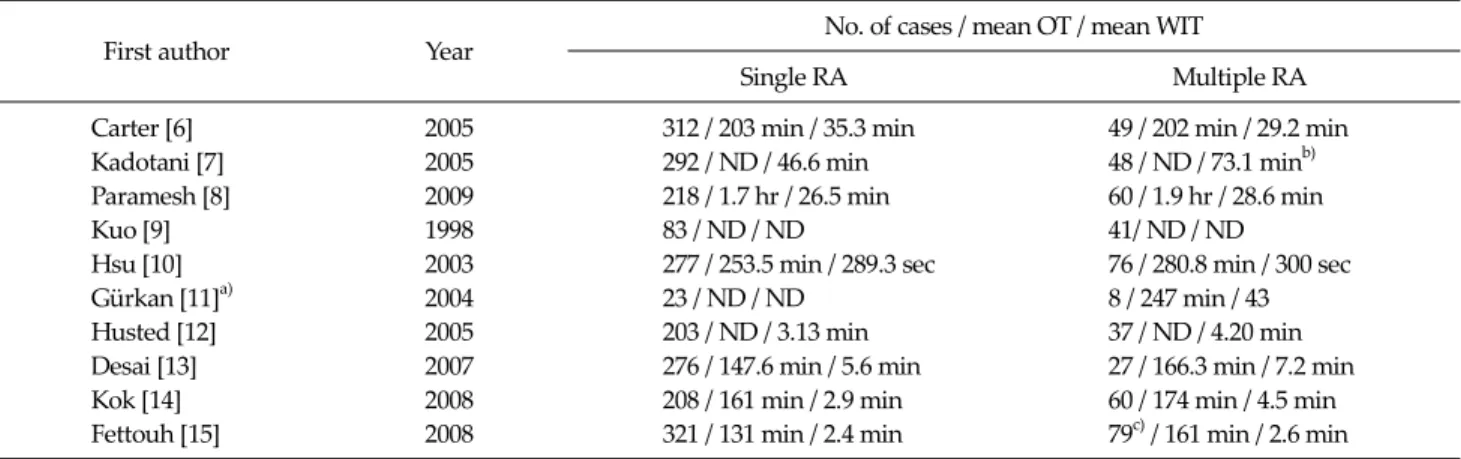
Table 4. Literature review regarding series of multiple renal arteries (RA) in laparoscopic donor nephrectomy
First author Year No. of cases / mean OT / mean WIT
Single RA Multiple RA
Carter [6] 2005 312 / 203 min / 35.3 min 49 / 202 min / 29.2 min
Kadotani [7] 2005 292 / ND / 46.6 min 48 / ND / 73.1 minb)
Paramesh [8] 2009 218 / 1.7 hr / 26.5 min 60 / 1.9 hr / 28.6 min
Kuo [9] 1998 83 / ND / ND 41/ ND / ND
Hsu [10] 2003 277 / 253.5 min / 289.3 sec 76 / 280.8 min / 300 sec
Gürkan [11]a) 2004 23 / ND / ND 8 / 247 min / 43
Husted [12] 2005 203 / ND / 3.13 min 37 / ND / 4.20 min
Desai [13] 2007 276 / 147.6 min / 5.6 min 27 / 166.3 min / 7.2 min
Kok [14] 2008 208 / 161 min / 2.9 min 60 / 174 min / 4.5 min
Fettouh [15] 2008 321 / 131 min / 2.4 min 79c) / 161 min / 2.6 min
OT, operation time; WIT, warm ischemia time; ND, no data.
a)In this study, cases with multiple arteries in laparoscopic donor nephrectomy were only compared with cases with multiple arteries in open donor nephrectomy and were not compared to cases with single arteries. b)Results in the article were defined as total ischemia time. c)Sum of the cases with multiple renal arteries (n = 59) and cases with venous anomalies and/or multiple veins (n = 20).
months (P = 0.10), and 12 months (P = 0.09) (Table 3).
DISCUSSION
LDN was associated with a significant improvement in postoperative pain control, better postoperative respira- tory function, a reduction in hospital stay, earlier return to normal activities, and improved wound cosmesis.
Furthermore, this operation technique resulted in similar graft survival and donor safety compared with open do-
nor nephrectomy [2]. This technique is technically chal- lenging related to various vascular abnormalities. Hence, an exact knowledge of the vascular anatomy and collect- ing system are mandatory before operation. We used mul- tidetector renal computed tomography angiography (MDCTA) for evaluation of the renal arteries preopera- tively. MDCTA has sensitivity ranging between 86-88%, specificity between 98-100% and accuracy between 93-98% for arterial anatomy [3-5]. In our study, 15.1% of the donor organs had multiple arteries, and CT evaluation of renal artery anatomy in these donors was sufficiently accurate for correctly identifying renal arteries and veins.
No false-positive accessory artery was detected but in one patient, a 2-mm accessory artery was missed on pre- operative CT angiography. We identified this accessory ar- tery during surgical dissection and it was undamaged.
Living donor kidneys with multiple arteries are also routinely procured laparoscopically. While there have been many studies related with the effects of laparoscopic versus open technique on graft function, there are only a limited number of studies in the literature including the effect of multiple renal arteries on graft function (Table 4).
While some studies reported a higher rate of surgical and medical complications after transplant with multiple arteries grafts [6-8], other reports suggested no difference related to rejection rate and patient and graft survival be-
tween cases with multiple and single arteries [9-15]. In this study, we aim to present our experience with LDN and to compare the graft function and outcome between cases with single versus multiple arteries.
Multiple renal arteries in LDN present potential disadvantages. Prolonged pneumoperitoneum related to increased operation time and increased WIT generally occurs. The pneumoperitoneum that is created during lap- aroscopy is known to be associated with adverse renal he- modynamic effects and acutely decreased urine output of native kidneys [16,17]. However, multiple studies includ- ing comparison of laparoscopic versus open donor neph- rectomy showed that this situation did not affect the long-term graft outcome [18-20]. Delayed graft function (DGF) is defined as hemodialysis requirement within one week of transplantation. The effect of WIT on DGF is con- troversial according to the literature. Jacobs et al. [21] com- pared WIT ≤ 3 minutes vs. ≥ 3 minutes and WIT ≤ 5 mi- nutes, 5-10 minutes, and ≥ 10 minutes, and showed that prolonged WIT did not affect graft function. Similarly, an- other study by Simforoosh et al. [22] compared three groups with WIT in the ranges of 4-6 minutes, 6-10 mi- nutes, and > 10 minutes, and no significant difference in graft function was detected among these groups. In con- trast, in a series reported by Sasaki et al. [23], a WIT of > 10 minutes was associated with acute tubular necrosis and an elevated serum creatinine concentration at 7 days post- transplantation. The WITs in this study are shorter than in other reports [6-15], because we used only one angle sta- pler and, thus, the kidney could be quickly extracted by hand. No time was lost with single-division of artery and vein and extraction bag. Nevertheless, we prepared the cold perfusion table equipment in concordance with the number of renal arteries for the duration of surgery.
Although we detected significantly longer WIT in the LDN-2 and LDN-3 groups than LDN-1 group, no sig- nificant difference was identified among these three groups with respect to graft outcome, including creatinine level, rejection rate and graft survival.
In conclusion, multiple renal arteries present a special challenge in both donor nephrectomy and renal trans- plantation. However, laparoscopic procurement of a kid- ney with multiple arteries, regardless of the number, is re-
liable and has no significant impact on the graft outcome.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
1. Ratner LE, Ciseck LJ, Moore RG, Cigarroa FG, Kaufman HS, Kavoussi LR. Laparoscopic live donor nephrectomy.
Transplantation 1995;60:1047-9.
2. Nicholson ML, Kaushik M, Lewis GR, Brook NR, Bagul A, Kay MD, et al. Randomized clinical trial of laparoscopic versus open donor nephrectomy. Br J Surg 2010;97:21-8.
3. Kim JK, Park SY, Kim HJ, Kim CS, Ahn HJ, Ahn TY, et al.
Living donor kidneys: usefulness of multi-detector row CT for comprehensive evaluation. Radiology 2003;229:869-76.
4. Namasivayam S, Small WC, Kalra MK, Torres WE, Newell KA, Mittal PK. Multidetector-row CT angiography for pre- operative evaluation of potential laparoscopic renal do- nors: how accurate are we? Clin Imaging 2006;30:120-6.
5. Chai JW, Lee W, Yin YH, Jae HJ, Chung JW, Kim HH, et al.
CT angiography for living kidney donors: accuracy, cause of misinterpretation and prevalence of variation. Korean J Radiol 2008;9:333-9.
6. Carter JT, Freise CE, McTaggart RA, Mahanty HD, Kang SM, Chan SH, et al. Laparoscopic procurement of kidneys with multiple renal arteries is associated with increased ureteral complications in the recipient. Am J Transplant 2005;5:1312-8.
7. Kadotani Y, Okamoto M, Akioka K, Ushigome H, Ogino S, Nobori S, et al. Management and outcome of living kidney grafts with multiple arteries. Surg Today 2005;35:459-66.
8. Paramesh A, Zhang R, Florman S, Yau CL, McGee J, Al-Abbas H, et al. Laparoscopic procurement of single ver- sus multiple artery kidney allografts: is long-term graft survival affected? Transplantation 2009;88:1203-7.
9. Kuo PC, Cho ES, Flowers JL, Jacobs S, Bartlett ST, Johnson LB. Laparoscopic living donor nephrectomy and multiple renal arteries. Am J Surg 1998;176:559-63.
10. Hsu TH, Su LM, Ratner LE, Trock BJ, Kavoussi LR. Impact of renal artery multiplicity on outcomes of renal donors and recipients in laparoscopic donor nephrectomy.
Urology 2003;61:323-7.
11. Gürkan A, Kaçar S, Başak K, Varilsüha C, Karaca C. Do multiple renal arteries restrict laparoscopic donor neph- rectomy? Transplant Proc 2004;36:105-7.
12. Husted TL, Hanaway MJ, Thomas MJ, Woodle ES, Buell JF.
Laparoscopic living donor nephrectomy for kidneys with multiple arteries. Transplant Proc 2005;37:629-30.
13. Desai MR, Ganpule AP, Gupta R, Thimmegowda M.
Outcome of renal transplantation with multiple versus sin- gle renal arteries after laparoscopic live donor neph- rectomy: a comparative study. Urology 2007;69:824-7.
14. Kok NF, Dols LF, Hunink MG, Alwayn IP, Tran KT, Weimar W, et al. Complex vascular anatomy in live kidney dona- tion: imaging and consequences for clinical outcome.
Transplantation 2008;85:1760-5.
15. Fettouh HA. Laparoscopic donor nephrectomy in the pres- ence of vascular anomalies: evaluation of outcome. J Endourol 2008;22:77-82.
16. Chiu AW, Chang LS, Birkett DH, Babayan RK. The impact of pneumoperitoneum, pneumoretroperitoneum, and gas- less laparoscopy on the systemic and renal hemodynamics.
J Am Coll Surg 1995;181:397-406.
17. London ET, Ho HS, Neuhaus AM, Wolfe BM, Rudich SM, Perez RV. Effect of intravascular volume expansion on re- nal function during prolonged CO2 pneumoperitoneum.
Ann Surg 2000;231:195-201.
18. Dave S, Farhat W, Pace K, Navarro O, Hebert D, Khoury AE. Effect of donor pneumoperitoneum on early allograft perfusion following renal transplantation in pediatric pa-
tients: an intraoperative Doppler ultrasound study. Pediatr Transplant 2008;12:522-6.
19. Percegona LS, Bignelli AT, Adamy A Jr, Machado C, Pilz F, Meyer F, et al. Early graft function in kidney trans- plantation: comparison between laparoscopic donor neph- rectomy and open donor nephrectomy. Transplant Proc 2008;40:685-6.
20. Bolte SL, Chin LT, Moon TD, D'Alessandro AM, Nakada SY, Becker YT, et al. Maintaining urine production and ear- ly allograft function during laparoscopic donor nephrec- tomy. Urology 2006;68:747-50.
21. Jacobs SC, Cho E, Foster C, Liao P, Bartlett ST. Laparoscopic donor nephrectomy: the University of Maryland 6-year experience. J Urol 2004;171:47-51.
22. Simforoosh N, Basiri A, Shakhssalim N, Ziaee SA, Tabibi A, Moghaddam SM. Effect of warm ischemia on graft out- come in laparoscopic donor nephrectomy. J Endourol 2006;20:895-8.
23. Sasaki TM, Finelli F, Bugarin E, Fowlkes D, Trollinger J, Barhyte DY, et al. Is laparoscopic donor nephrectomy the new criterion standard? Arch Surg 2000;135:943-7.