235
Copyrights © 2014 The Korean Society of Radiology
INTRODUCTION
Surgical pericardiotomy is an effective method to treat malig- nant pericardial effusion. Although pericardiotomy is generally considered safe, it has its risk of complications, including hemo- thorax, arrhythmia, hypotension, or heart failure (1). Metastatic tumor seeding along a transient indwelling drainage tube is an extremely rare complication of pericardiotomy. To our knowl- edge, no such case has ever been reported. We present a case of tumor implantation along the pericardiomtomy tube tract in a patient with lung cancer.
CASE REPORT
A 48-year-old man was admitted to hospital due to dyspnea that had started a few days before. The patient was diagnosed with non-small cell lung cancer (adenocarcinoma) in the left lower lobe with brain and bone metastases in May 2012, which subsequently progressed despite 3 courses of chemotherapy
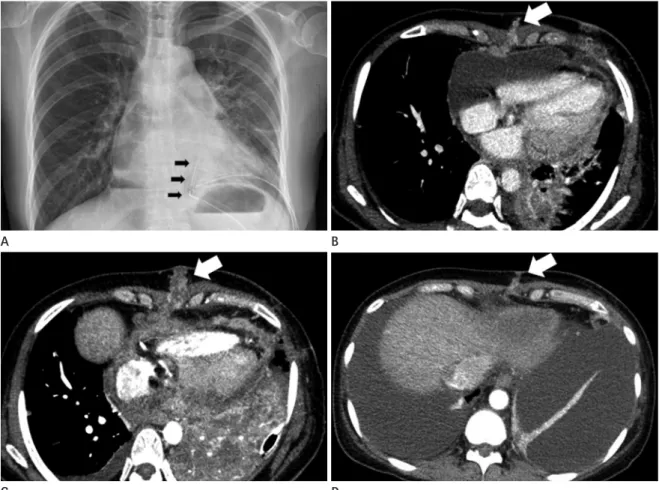
with various chemotherapeutic regiments [Gefitinib (Iress®), May 2012 through November 2012; Pemetrexed (Alimta®)-cisplatin, December 2012 through January 2013; Erlotinib (Tarceva®), May 2013 through July 2013]. Chest radiograph taken at the time of admission showed cardiomegaly with a moderate amount of left-sided pleural effusion. Electrocardiography showed low voltage sinus tachycardia (mean, 115/min). Transthoracic echo- cardiography revealed a large amount of pericardial effusion causing hemodynamic compromise compatible with cardiac tamponade. The patient underwent a pericardial window opera- tion on the day of admission. About 2500 mL of bloody pericar- dial effusion was drained. Two chest tubes (one via the subxi- phoid region and the other via the lateral chest wall) introduced though separate stab incisions were connected to a suction ma- chine (Fig. 1A). Both chest tubes were left in place for 5 days.
The pericardial specimen was submitted for histological analysis which revealed fibrosis with chronic inflammation and vascular proliferation. The pericardial fluid was submitted for cytological analysis which revealed metastatic adenocarcinoma. The pa-
Case Report
pISSN 1738-2637 / eISSN 2288-2928 J Korean Soc Radiol 2014;71(5):235-238 http://dx.doi.org/10.3348/jksr.2014.71.5.235
Received April 3, 2014; Accepted August 26, 2014 Corresponding author: Dae Hee Han, MD Department of Radiology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 137-701, Korea.
Tel. 82-2-2258-1436 Fax. 82-2-599-6771 E-mail: [email protected]
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distri- bution, and reproduction in any medium, provided the original work is properly cited.
Tube tract implantation metastasis of non-small cell lung cancer is an extremely rare complication of surgical pericardiotomy. We report a case of tube tract seeding along the previous chest tube tract in the subxiphoid region. The subxiphoid tube tract seeding was created during pericardial window operation of a 48-year-old male patient with lung cancer for the drainage of malignant pericardial effusion.
Index terms Pericardiotomy Tube Tract Implantation Lung Cancer
Malignant Pericardial Effusion
Implantation of Lung Cancer along the Tube Tract after
Pericardiotomy for Malignant Pericardial Effusion: A Case Report
악성 심낭삼출액 제거를 위해 시행한 심막절개술 후 튜브경로를 따라 발생한 폐암의 이식성 전이: 증례 보고Joo Yeon Kim, MD, Dae Hee Han, MD
Department of Radiology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
Implantation of Lung Cancer along the Tube Tract after Pericardiotomy for Malignant Pericardial Effusion
236
J Korean Soc Radiol 2014;71(5):235-238 jksronline.orgfestation in malignancies. Accessible treatment options include simple drainage and surgical approach, with the primary goal to relieve symptoms and improve quality of life. In emergency cas- es, with cardiac tamponade or significant effusion, initial relief could be obtained with percutaneous pericardiocentesis, occa- sionally followed by drainage with indwelling catheter or thorac- ic surgery (pericardiotomy or pericardial window operation) (1).
The most serious complication of pericardiocetesis is injury to the myocardium or coronary vessels. In addition, pneumotho- rax, hemothorax, serious arrhythmia, and puncture of the peri- toneal cavity or abdominal organ can also occur. Chylopericar- dium and intrapericardial thrombosis have rarely been reported (2). A large echocardiography-based study reported that the in- cidence of major complications after pericardiocentesis was be- tween 1.3% and 1.6% (3). Tract metastasis is an extremely rare complication of pericardiocentesis or pericardiotomy (4), where- tient’s condition improved considerably after the procedure with
no further complications.
Chest CT performed 12 days after the surgery revealed new soft tissue density nodules along the previous chest tube tract in the subxiphoid region (Fig. 1B). Although the nodules were not biopsied, repeated chest CT performed 1 month later showed a significant increase in nodule size with progression of nodular thickening of pericardium (Fig. 1C). The patient received che- motherapy with a new regimen. Chest CT performed at 3-month after the pericardial window operation revealed marked regres- sion of both the subxiphoid nodules and the pericardial thick- enings (Fig. 1D).
DISCUSSION
Malignant pericardial effusion is a common and serious mani-
Fig. 1. Chest PA taken immediately after pericardial window operation. Two indwelling chest tubes are inserted via subxiphoid (arrows) and intercostal routes, respectively (A). Chest CT obtained 12 days after surgery reveals linear arrayed soft tissue densi- ty nodules along the tract of the subxiphoid chest tube (removed) (B). CT obtained 1 month after surgery reveals remarkable in- terval growth of the seeded nodules and progression of pericardial nodular thickening (C). Post-chemotherapy CT (3 months af- ter surgery) shows marked regression of the seeded nodules and the pericardial thickenings (D).
A
C
B
D
Joo Yeon Kim, et al
237
jksronline.org J Korean Soc Radiol 2014;71(5):235-238
regions. Therefore, it was very likely that the soft tissue repre- sented tumor implantation.
In conclusion, we report a case of lung cancer implantation along the previous pericardiotomy tube tract as an extremely rare complication of malignant pericardial effusion treatment.
REFERENCES
1. Burazor I, Imazio M, Markel G, Adler Y. Malignant pericar- dial effusion. Cardiology 2013;124:224-232
2. Ceron L, Manzato M, Mazzaro F, Bellavere F. A new diag- nostic and therapeutic approach to pericardial effusion:
transbronchial needle aspiration. Chest 2003;123:1753- 1758
3. Tsang TS, Enriquez-Sarano M, Freeman WK, Barnes ME, Sinak LJ, Gersh BJ, et al. Consecutive 1127 therapeutic echocardiographically guided pericardiocenteses: clinical profile, practice patterns, and outcomes spanning 21 years. Mayo Clin Proc 2002;77:429-436
4. Quecedo E, Febrer I, Martínez-Escribano JA, Navarro- Iváñez R, Aliaga A. Tumoral seeding after pericardiocente- sis in a patient with a pulmonary adenocarcinoma. J Am Acad Dermatol 1994;31(3 Pt 1):496-497
5. Janes SM, Rahman NM, Davies RJ, Lee YC. Catheter-tract metastases associated with chronic indwelling pleural catheters. Chest 2007;131:1232-1234
6. Al-Saif OH, Sengupta B, Meshikhes AW. Port site metastases after a laparoscopic abdominoperineal resection of rectal cancer: report of a case. Surg Today 2011;41:412-414 7. Loew R, Dueber C, Schwarting A, Thelen M. Subcutaneous
implantation metastasis of a cholangiocarcinoma of the bile duct after percutaneous transhepatic biliary drainage (PTBD). Eur Radiol 1997;7:259-261
8. Kim JH, Kim YT, Lim HK, Kim YH, Sung SW. Management for chest wall implantation of non-small cell lung cancer after fine-needle aspiration biopsy. Eur J Cardiothorac Surg 2003;23:828-832
9. Uramoto H, Hanagiri T. Video-assisted thoracoscopic peri- cardiectomy for malignant pericardial effusion. Anticancer Res 2010;30:4691-4694
as catheter-tract metastasis is relatively common (0.5% in three large series of a combined 374 cases) complication of malignant pleural effusion (5). The occurrence of implantation metastasis has been reported in other interventional or surgical proce- dures, such as fine needle lung biopsy, percutaneous transhepat- ic biliary drainage, percutaneous ethanol injection for the treat- ment of hepatocellular carcinoma or liver metastasis, and gastrostomy tube insertion and laparoscopy (6, 7).
The mechanism of implantation metastasis is uncertain. Pos- sible mechanisms of tumor cell seeding include tumor cell dis- semination into soft tissue during a procedure and tumor cell growth along a tract as in perineural tumor growth (7). Possible risk factors of tumor dissemination have been postulated by many authors. Tumor dissemination may depend on the caliber and the type of the device used, the number of procedures per- formed, the absence of normal parenchyma overlying the lesion, and the skill of operator. Of those risk factors, the type of the de- vice used seems to be most important. The larger the caliber of the device is used, the greater the opportunity for tumor cells to seed along the tract (4). The duration between a percutaneous procedure and the appearance of an implantation lesion is highly variable, from 2 to 26 months (8). In most cases, time to tumor development is shorter in procedures using more aggressive techniques (4). In our patient, only 12 days elapsed after the chest tube insertion before the seeding nodules appeared on CT. Such a rapid tumor growth may have been related to the large caliber of the indwelling chest tube or the aggressive nature of the tumor as evidenced by rapid interval enlargement of pericardial nodule (Fig. 1B, C), lung nodules, and mediastinal lymph nodes.
The limitation of the current report is the lack of pathologic confirmation. In principle, various conditions such as infection could be considered as differentials. However, although place- ment of a pericardial indwelling catheter was known to carry a risk of infection (9), there were no infection signs either at that time of the imaging or during the cytotoxic chemotherapy. In addition, the soft tissue at the previous tube tract progressed and regressed simultaneously with the metastatic pericardial nod- ules, pulmonary nodules, and mediastinal lymphadenopathies before and after the chemotherapy, respectively. Although there was no histological proof on nodules or pericardial thickenings, cytological metastasis revealed that fluid flowed through both
Implantation of Lung Cancer along the Tube Tract after Pericardiotomy for Malignant Pericardial Effusion
238
J Korean Soc Radiol 2014;71(5):235-238 jksronline.org악성 심낭삼출액 제거를 위해 시행한 심막절개술 후 튜브경로를 따라 발생한 폐암의 이식성 전이: 증례 보고
김주연 · 한대희
배액관 자리를 따라 발생한 이식성 전이는 심막절개술 이후 발생할 수 있는 매우 드문 합병증이다. 우리는 48세 폐암 환 자에서 악성 심낭삼출액에 대한 치료로 심막창형성술을 시행한 이후에 일시적으로 거치한 심낭 배액관 자리를 따라 발생 한 이식성 전이를 보고하고자 한다.
가톨릭대학교 의과대학 서울성모병원 영상의학과