Athough conventional angiography is still considered the gold standard for the detection and diagnosis of coro- nary artery disease (CAD), it is a highly invasive proce-
dure. Multi-detector computed tomography (MDCT) for imaging the heart is a promising noninvasive technique in terms of its ability to visualize the coronary arteries (1-6). However, it is well known that the image quality is highly dependent on the heart rate, and the cardiac motion artifacts caused by higher heart rates (HRs) re- main a major cause of image degradation in MDCT coronary angiography (7-9). Some recent papers have reported that motion-free coronary angiograms can be consistently obtained when the HR is less than 80 bpm (10) and 64-slice MDCT provides diagnostic-quality im- ages of the coronary arteries within a wide range of
The Influence of Heart Rate and its Variations on Image Quality: A Comparative Study of 16- and 64-Slice
Multidetector Row Computed Tomography
1Dong Hun Kim, M.D., Sang Il Choi, M.D.2, Eun Ju Chun, M.D.2, Jae Hyung Park, M.D.3
1Department of Radiology, Soonchunhyang University Bucheon Hospital, Bucheon, Korea
2Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea
3Department of Radiology, Seoul National University Hospital, Seoul, Korea
Received December 9, 2008 ; Accepted January 21, 2009
Address reprint requests to : Sang Il Choi, M.D., Department of Radiology, Seoul National University Bundang Hospital, 300, Gumi- dong, Bundang-gu, Seongnam-si, Gyeonggi-do, 463-707, Korea
Tel. 82-31-787-7611 Fax. 82-31-787-4011 E-mail: [email protected]
Purpose: We wanted to investigate the influence of heart rate (HR) and its variations on the CT angiography (CTA) image quality with using 16- and 64-slice multidetector CT (MDCT).
Materials and Methods: Of the 200 recruited patients, 100 underwent 16-slice MDCT (M:F=74:26, median age: 55.2 ± 12.8 years) and 100 underwent 64-slice MDCT (M:F=68:32, median age: 58.4 ± 11.6 years). We evaluated the image quality with re- spect to the HR and the variations in the HR. The images were graded in terms of the quality of vessel depiction with using a four-point scoring system from 1 to 4, where 4 represented the best image quality. In addition, we analyzed the 16- and 64-slice MD- CT images in terms of the presence and frequency of stair-step artifacts.
Results: The mean HR variation was significantly lower on 64-slice MDCT than that on 16-slice MDCT (5.48 ± 4.20 bpm vs. 10.31 ± 5.90 bpm, respectively, p < 0.05).
The mean image quality score of 64-slice MDCT was significantly greater than that of 16-slice MDCT (3.40 ± 0.36 vs. 2.75 ± 0.43, respectively, p < 0.05). The frequency of stair-step artifacts was markedly greater for 16-slice MDCT (2.4 ± 3.2 vs. 0.5 ± 1.04, respectively, p < 0.05).
Conclusion: 64-slice MDCT provides better image quality because it reduces the scan times and minimizes the HR variations.
Index words :Tomography, X-ray Heart rate
Coronary artery disease
heart rates (38-102 bpm) (11), yet higher HRs and varia- tions in the HR significantly degrade the image quality of the whole coronary tree. Because the HR increases or it is highly variable in most patients during CT scanning, and even within short breath-hold durations (9-13) HR responsive scanning or premedications such as β-block- ers that lower and stabilize HR may increase the image quality by minimizing the influence of HR variations (9, 14).
To the best of our knowledge, the effect of HR and its variations on the image quality of 16- and 64-slice MDCTs, which are commonly used in current practice, have not yet been investigated and reported on in Korea. Therefore, we investigated the influence of HR and its variations on the image quality of the coronary CT angiograms obtained with using 16- and 64-slice MDCTs.
Materials and Methods
Patients
This retrospective study was conducted on 200 pa- tients who had undergone coronary CT angiography.
One hundred of them had undergone cardiac CT using a 16-slice MDCT from January 2006 to July 2006 (men:women=74:26, mean age: 55.2 ± 12.8 years), and the other 100 had undergone cardiac CT using a 64-slice MDCT from May 2007 to June 2007 (men:women=
68:32, mean age: 58.4 ± 11.6 years). The HRs were checked before and during the CT scans for all the pa- tients. To analyze the effects of HR on image quality, the patients were classified according to HR as follows: (1)
< 60 bpm, (2) 61-70 bpm, (3) 71-80 bpm, (4) 81-90 bpm, (5) 91-100 bpm and (6) >100 bpm. Variations in HR were defined as the difference between the highest
and lowest HR, and these variations were classified as:
(1) 0-5 bpm, (2) 6-10 bpm, (3) 11-15 bpm, (4) 16-20 bpm and (5) > 20 bpm. No β-blocker was administered to any patient prior to coronary CTA. The patients with a severe calcification in a coronary artery, a stent or who had undergone coronary bypass grafting were also ex- cluded.
MDCT Exam
Coronary CT angiography was performed with the use of a 16- slice MDCT scanner with a 0.42-s rotation time (Mx8000 IDT; Philips Medical Systems, Best, The Netherlands) and a 64-slice MDCT scanner with a 0.42-s rotation time (Brilliance 64, Philips Medical Systems, Best, The Netherlands) with retrospective ECG gating.
A standard scanning protocol was applied, with 16×
0.75-mm and 64×0.625-mm section collimation, a gantry rotation time of 420-msec, a tube energy of 120 kV and an effective tube current of 500/800 mAs. A bo- lus of 100-120 mL (16-slice MDCT) or 75-85 ml (64-slice MDCT) contrast media (Ioprovid, Ultravist 370;
Schering, Berlin, Germany) was intravenously injected (4 mL/sec). By using a Bolus Pro Ultra (BPU), a region of interest was placed in the ascending aorta (16-slice MD- CT)/descending thoracic aorta (64-slice MDCT) and the scan was automatically initiated once a selected thresh- old (150 HU) was reached. The ECG of the patient was saved concurrently with the acquisitions. The mean scan duration was 18 ± 3 seconds (range: 15 to 24 sec) for the 16-slice MDCT and 11 ± 3 seconds (range: 8 to 14 sec) for the 64-slice MDCT. The various scan parame- ters are shown in Table 1.
Image Reconstruction and Analysis
After acquisition of the raw helical CT data, retrospec-
Table 1. A Four-point Grade Scale of Image Quality
16-Slice MDCT 64-Slice MDCT
Collimation 16 × 0.75 mm 64 × 0.625 mm
Thickness/Increment 0.8 / 0.4 mm 0.67 / 0.33 mm
Pitch 0.2 0.2
Rotation time 420 msec 420 msec
Temporal resolution 53 msec 53 msec
kVp/mAs 120 / 500 120 / 800
Scan time 15-24 sec 8-14 sec
Threshold /delay time 200 HU / 5sec 150 HU / 6.5 sec
ROI ascending aorta descending aorta
Contrast media 100-120 ml (4 ml/sec) 75-85 ml (4 ml/sec)
+30 ml (3 ml/sec)saline +60 ml (3.5 ml/sec) CM & saline (3:7) Note. Use with retrospective ECG gating algorithm & adaptive multi-cycle reconstruction. HU, Hounsfield Unit; ROI, region of interest;
CM, contrast media
tively ECG-synchronized sections were reconstructed using adaptive multi-cyclic reconstruction and a heart rate responsive gating algorithm. The projection data was collected to provide image data sets at the desired physiological phases during the cardiac cycle. All the da- ta was processed using a dedicated workstation (Extended Brilliance Workspace; Philips Medical Systems, Best, The Netherlands) and the were displayed
using visualization techniques such as source tomo- grams, thin-slab maximum intensity projections (MIPs), multi-planar reformation (MPR) and volume rendering.
Subsequently, the curved MPR images were assessed for motion-free imaging (i.e., no tattered or ragged delin- eations) of the coronary branches. All three image post- processing modalities (source tomograms, thin-slab MIPs and curved MPRs) were used for the subjective
A B
C D
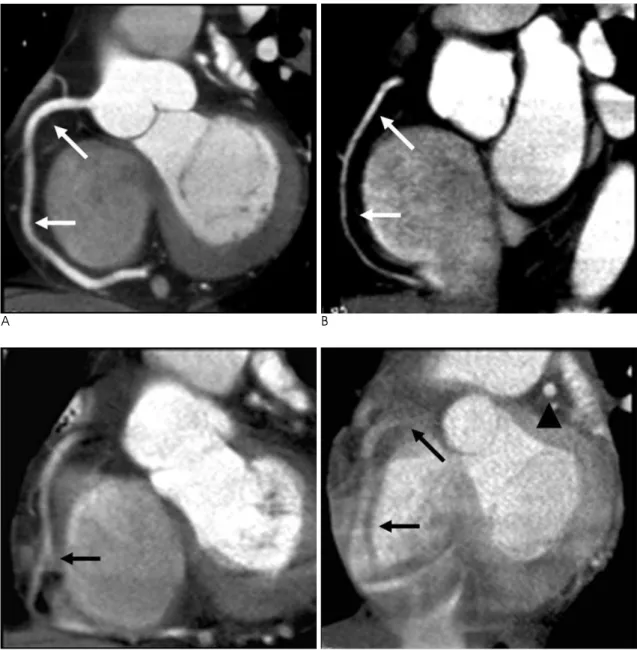
Fig. 1. Multiplanar reformations with a short axis view of the RCA in four patients, along with the semiquantitative four-point im- age quality scores.
A. An image with a quality score of 4 shows no motion artifacts (arrows) in all the proximal to mid segments of the three coronary arteries.
B. An image with a quality score of 3 shows no/minimal motion artifacts and it is assessable in the proximal to mid segments of two coronary arteries (arrows).
C. An image with a quality score of 2 is assessable in all the proximal segments of three coronary arteries. There is an obscure mid- dle segment of the RCA (arrow).
D. An image with a quality score of 1 is assessable in the proximal segments of one or two coronary arteries. Although the RCA cannot be assessed (arrows), the proximal segment of the LAD is seen clearly (arrowhead).
evaluations. Three investigators (DHK, EJC and SIC, with 4, 2 and 5 years of coronary CT angiography expe- rience, respectively) assessed the coronary artery seg- ments according to the guidelines of the American College of Cardiology and the American Heart Association (15). The image quality was evaluated by in- vestigators who were kept “blind” to the HRs and the variations in the HRs. Decisions concerning image qual- ity were achieved by consensus. The images were grad- ed with respect to vessel depiction with using a four- point scoring system (1 to 4), where 4 represented best image quality (Fig. 1). Image scores between 3 and 4 were considered adequate for coronary assessments, and those with scores of 1 or 2 were considered inade- quate. The scores were defined as shown in Table 2. In addition, high quality images were chosen by selecting an optimized HR window. Banding artifacts, including stair-step and acceleration artifacts caused by changes in HR, were evaluated on the 16-slice and 64-slice MDCT scans (Fig. 2). The artifacts were registered as present or not.
Statistical Analysis
Descriptive statistics were stratified according to the image quality scores into four image quality groups.
Continuous variables are expressed as means ± stan- dard deviations. P values < 0.05 indicated statistical sig- nificance. The Kruskal-Wallis test was used to evaluate the quantitative parameters (HR and its variations), which were stratified by the four image quality scores.
The two-sample t-test was used to compare the means of the image quality scores of the MDCTs. All the statisti- cal analyses were performed with SPSS, version 12.0.
Results
The numbers of the patients in each HR range (16- slice MDCT: 64-slice MDCT) before the scans were as follows: (1) < 60 bpm (n= 25:22), (2) 61-70 bpm (n=
32:30), (3) 71-80 bpm (n= 23:29), (4) 81-90 bpm (n=
13:15), (5) 91-100 bpm (n= 5:3) and (6) >100 bpm (n=
2:1) (Table 3). The mean HRs were 68.45 beats per minute ± 15.42 in the patients before undergoing 16- slice MDCT scanning and 68.90 beats per minute ±
A B
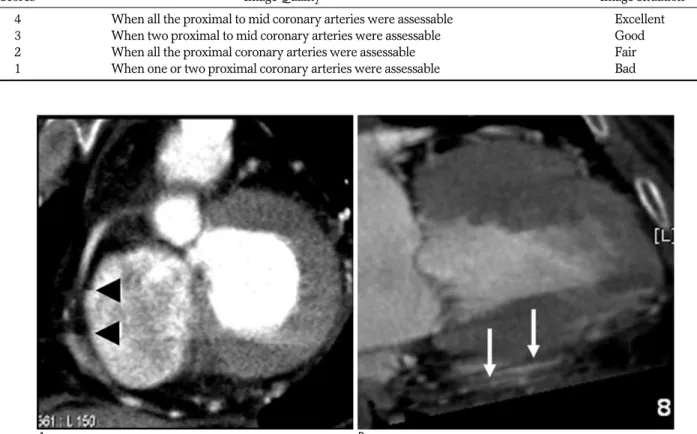
Fig. 2. Stair-step and acceleration artifacts.
A. Stair-step like motion artifacts are seen on the right coronary artery (arrowheads).
B. Prominent acceleration artifacts (arrows) are seen below the inferior wall of the LV.
Table 2. A Four-point Grade Scale of Image Quality
Scores Image Quality Image Situation
4 When all the proximal to mid coronary arteries were assessable Excellent
3 When two proximal to mid coronary arteries were assessable Good
2 When all the proximal coronary arteries were assessable Fair
1 When one or two proximal coronary arteries were assessable Bad
14.25 in the patients before undergoing 64-slice MDCT scanning. The mean HRs of the patients who under- went cardiac CT with a 16-slice or 64-slice MDCT were 71.04 beats per minute ± 13.52 and 69.31 beats per minute ± 14.71, respectively. A high HR variation was found to be associated with poor image quality (the mean score for 16-slice MDCT vs. that for 64-slice MD- CT: 3.17 vs. 3.63 at 0-5 bpm, 2.06 vs. 2.25 in 16-20 bpm, p < 0.05) (Table 4). 64-slice MDCT was found to have a higher mean image quality score (3.41 ± 0.97 vs.
2.84 ± 0.53, respectively, p < 0.05) and less occurrence of artifact (0.5 ± 1.04 vs. 2.4 ± 3.2, respectively, p <
0.05) (Table 5). In particular, the acceleration artifacts occurred more often in the 16-slice MDCT scans (n=11
vs. n =1).
Discussion
The overall diagnostic quality of noninvasive CT coro- nary angiography is largely dependent on the spatial res- olution, the HR during the examination, an appropriate reconstruction time point within the cardiac cycle and the contrast enhancement (2). The present study shows that greater HR variations and higher HRs deteriorate the image quality. Furthermore, our study shows that HR variations importantly affect the 16- and 64-slice MDCT image quality, which concurs with the findings of Lee et al. (16). In that previous report, the coronary CT angiography image quality was found to be more af- fected by variations in the HR than by a high HR, and the selection of an optimized reconstruction window for good image quality was found to be most affected by the HR when 4-detector row CT without multicyclic recon- struction and a HR responsive gating algorithm were used. Our study also showed the same result that HR variation affected the image quality rather than the HR.
Hoffmann et al. (10) suggested that any strategy to opti- mize the temporal resolution based on a single fixed HR would fail because of the highly variable nature of HRs even for a short breath-hold duration. In addition, they suggested that the initial HR be reduced to less than 75 Table 4. Image Quality, According to Variations of Heart Rate, between 16-slice MDCT and 64-slice MDCT
Variations of HR (Number of Patients) Image Quality Score for 16-slice MDCT Image Quality Score for 64-slice MDCT
0-5 bpm (n=30/47) 3.17 3.63
6-10 bpm (n=33/37) 2.97 3.46
11-15 bpm (n=19/12) 2.37 2.75
16-20 bpm (n=16/4)0 2.06 2.25
> 20 bpm (n=2/0)00 2.00 -
Average 2.75 ± 0.43 3.40 ± 0.36
Note. The average of image quality score for 64-slice MDCT is higher than that of 16-slice MDCT and the difference is statistically signifi- cant (p < 0.05) (two sample t-test).
Table 5. Comparison of artifact (stair-step) between 16-slice MD- CT and 64-slice MDCT
Variations of HR 16-slice MDCT 64-slice MDCT
0-5 bpm 0.4 0.2
6-10 bpm 1.3 0.3
11-15 bpm 3.3 1.6
16-20 bpm 6.9 2.3
> 20 bpm 7.0 -
Total 2. 4 ± 3.2� 0.5 ± 1.04�
Note. “�” means the number of occurred artifact/total patients for each variation of HR ± standard deviation. 64-slice MDCT was found to have fewer occurrences of artifacts (p < 0.05) than that of 16-slice MDCT.
Table 3. Image Quality between 16-slice MDCT and 64-slice MDCT for Different HR Values
HR Value (Number of Patients) Image Quality Score for 16-slice MDCT Image Quality Score for 64-slice MDCT
< 60 bpm (n=25/22) 3.60 3.80
61-70 bpm (n=32/30) 2.97 3.33
71-80 bpm (n=23/29) 2.22 3.20
81-90 bpm (n=13/15) 2.50 2.80
91-100 bpm (n=5/3)00 2.40 30.0
> 100 bpm (n=2/1)00 30.0 30.0
Average 2.86 ± 0.52 3.30 ± 0.32
Note. The average image quality score for 64-slice MDCT is higher than that of 16-slice MDCT and the difference (p < 0.05) is statistically significant (two sample t-test).
bpm to include a safety margin and to optimize the im- age quality because the HR in most patients increases slightly during scanning.
So then, how do we overcome this problem?
Fortunately, there have been several recent develop- ments that minimize image degradations due to higher HRs and HR variations. First, adaptive multi-cycle re- construction algorithms are available over a wider range of HRs up to 80-100 bpm for 16-slice or 64-slice scan- ners. These algorithms automatically adjust the system as the HR varies during spiral acquisition. Second, spe- cific cardiac phases or intervals can be determined based on the R waves of the ECG signals. This approach uses either a fixed offset or a fixed percentage delay dur- ing the R-R interval to determine a particular phase of the cardiac cycle (17). However, this method requires that the operator directly select the ideal phase for imag- ing, and it does not account for the variable diastolic phase of the heart (18, 19). Third, a delay algorithm can be used to automatically compensate for the non-lineari- ties during the systolic and diastolic portions of the car- diac cycle that are caused by HR variations to ensure that a desired physiological phase is captured and recon- structed. However, the images produced with using this algorithm are often poor. Finally, premedication, such as with a beta-blocker, can be used to reduce the heart rate and arrhythmia.
In addition to examining the effect of HR and its varia- tions on image quality, we also found that the image quality score was higher and the frequency of artifacts was lower for 64-slice MDCT (3.41 ± 0.97, 0.5 ± 1.04) than for 16-slice MDCT (2.84 ± 0.53, 2. 4 ± 3.2). In par- ticular, motion artifacts such as acceleration or stair-step artifacts occurred more frequently on the 16-slice MD- CT scans than on the 64-slice MDCT scans (n=11 vs. n
=1). These results were probably due to the narrower coverage (16 × 0.75 mm) and the slower scan time (18
± 3 seconds) of 16-slice MDCT than those for 64-slice MDCT (64 × 0.625 mm, 11 ± 3 seconds).
In conclusion, we suggest that 64-slice MDCT pro- duces better image quality than that of 16-slice MDCT by minimizing the HR variations, reducing the scan times and improving the spatial and temporal resolu- tions.
References
1. Schoenhagen P, Halliburton S, Stillman A, Kuzmiak SA, Nissen SE, Tuzcu EM, et al. Noninvasive imaging of coronary arteries:
current and future role of multi-detector computed tomography.
Radiology 2004;232:7-17
2. Schoepf UJ, Becker CR, Ohnesorge BM, Yucel EK. CT of coronary artery disease. Radiology 2004;232:18-37
3. Kuettner A, Beck T, Drosch T, Kettering K, Heuschmid M, Burgstahler C, et al. Diagnostic accuracy of noninvasive coronary imaging using 16-detector slice spiral computed tomography with 188 ms temporal resolution. J Am Coll Cardiol 2005;45:123-127 4. Schlosser T, Konorza T, Hunold P, Kuhl H, Schmermund A,
Barkhausen J. Noninvasive visualization of coronary artery bypass grafts using 16-detector row computed tomography. J Am Coll Cardiol 2004;44:1224-1229
5. Yamamuro M, Tadamura E, Kubo S, Nishina T, Ohba M, Hosokawa R, et al. Cardiac functional analysis with multi-detector row CT and segmental reconstruction algorithm: comparison with echocardiography, SPECT, and MR imaging. Radiology 2005;234:
381-390
6. Schuijf JD, Bax JJ, Jukema JW, Lamb HJ, Vliegen HW, van der Wall EE, et al. Noninvasive evaluation of the coronary arteries with multislice computed tomography in hypertensive patients.
Hypertension 2005;45:227-232
7. Nieman K, Rensing BJ, van Geuns RJ, Vos J, Pattynama PM, Krestin GP, et al. Non-invasive coronary angiography with multi- slice spiral computed tomography: impact of heart rate. Heart 2002;88:470-474
8. Hong C, Becker CR, Huber A, Schoepf UJ, Ohnesorge B, Knez A, et al. ECG-gated reconstructed multi-detector row CT coronary an- giography: effect of varying trigger delay on image quality.
Radiology 2001;220:712-717
9. Schroeder S, Kopp AF, Kuettner A, Burgstahler C, Herdeg C, Heuschmid M, et al. Influence of heart rate on vessel visibility in noninvasive coronary angiography using new multislice computed tomography: experience in 94 patients. Clin Imaging 2002;26:106- 111
10. Hoffmann MH, Shi H, Manzke R, Schmid FT, De Vries L, Grass M, et al. Noninvasive coronary angiography with 16-detector row CT: effect of heart rate. Radiology 2005;234:86-97
11. Leschka S, Wildermuth S, Boehm T, Desbiolles L, Husmann L, Plass A, et al. Noninvasive coronary angiography with 64-section CT: effect of average heart rate and heart rate variability on image quality. Radiology 2006;241:378-385
12. Wintersperger BJ, Nikolaou K, von Ziegler F, Johnson T, Rist C, Leber A, et al. Image quality, motion artifacts, and reconstruction timing of 64-slice coronary computed tomography angiography with 0.33-second rotation speed. Invest Radiol 2006;41:436-442 13. Herzog C, Arning-Erb M, Zangos S, Eichler K, Hammerstingl R,
Dogan S, et al. Multi-detector row CT coronary angiography: influ- ence of reconstruction technique and heart rate on image quality.
Radiology 2006;238:75-86
14. Vembar M, Garcia MJ, Heuscher DJ, Haberl R, Matthews D, Bohme GE, et al. A dynamic approach to identifying desired physi- ological phases for cardiac imaging using multislice spiral CT.
Meds Phys 2003;30:1683-1693
15. Bashore TM, Bates ER, Berger PB, Clark DA, Cusma JT, Dehmer GJ, et al. American College of Cardiology/Society for Cardiac Angiography and Interventions clinical expert consensus docu- ment on cardiac catheterization laboratory standards: a report of the american college of cardiology task force on clinical expert consensus documents. J Am Coll Cardiol 2001;37:2170-2214 16. Lee SH, Choi BW, Kim HJ, Jung H, Son HK, Kang WS, et al.
Analysis of the heart rate and its variation affecting image quality and optimized reconstruction window in retrospective ECG-gated coronary angiography using multidetector row CT. IEEE Trans
Nucl Sci 2004; 51: 225-231
17. Ohnesorge B, Flohr T, Becker C, Kopp AF, Schoepf UJ, Baum U, et al. Cardiac imaging by means of electrocardiographically gated multisection spiral CT: initial experience. Radiology 2000;217:564- 571
18. Lewis RP, Rittogers SE, Froester WF, Boudoulas H. A critical re- view of the systolic time intervals. Circulation 1977;56:146-158 19. Boudoulas H, Rittgers SE, Lewis RP, Leier CV, Weissler AM.
Changes in diastolic time with various pharmacologic agents: im- plication for myocardial perfusion. Circulation 1979;60:164-169
대한영상의학회지 2009;60:233-239
16열-과 64열-다절편 전산화단층촬영의 비교 연구1
1순천향대학교 부천병원 영상의학과
2분당서울대학교병원 영상의학과
3서울대학교병원 영상의학과 김동훈∙최상일2∙전은주2∙박재형3
목적: 16열 과 64열 다절편 전산화단층촬영(이하MDCT라 함)을 이용하여 CT관상동맥 영상 질에 미치는 심박수와 심박수 변화에 대하여 연구하고자 하였다.
대상과 방법: 200명을 대상으로 하였으며, 100명(남: 여=74명: 26명, 55.2 ± 12.8 세)은 16열 MDCT를, 또 다 른 100명(남: 여=68명: 32명, 58.4 ± 11.6 세)은 64열 MDCT를 촬영하였다. 저자들은 심박수와 심박수변화에 따른 영상질을 검사하였다. 영상은 1점에서 4점까지 혈관 분석으로 하였으며 4점이 가장 좋은 영상을 의미한다. 덧 붙여, 16열 및 64열 MDCT에서 계단상 허상(stair-step artifacts)을 분석하였다.
결과: 평균 심박수 변화는 64열 MDCT에서 16열 MDCT보다 의미 있게 낮았다(5.48 ± 4.20 회/분 과 10.31 ± 5.90 회/분, p < 0.05). 평균 영상 질 수치는 64열 MDCT에서 16열 MDCT보다 의미 있게 높았다 (3.40 ± 0.36 점 과 2.75 ± 0.43점, p < 0.05). 계단상의 허상은 16열 MDCT에서 64열 MDCT보다 더 많이 발생하였다 (2.4
± 3.2회/검사와 0.5 ± 1.04회/검사, p < 0.05).
결론: 64-열 MDCT는 스캔시간을 줄이고 심박수 변화가 최소화되기 때문에 더 나은 영상을 제공한다.