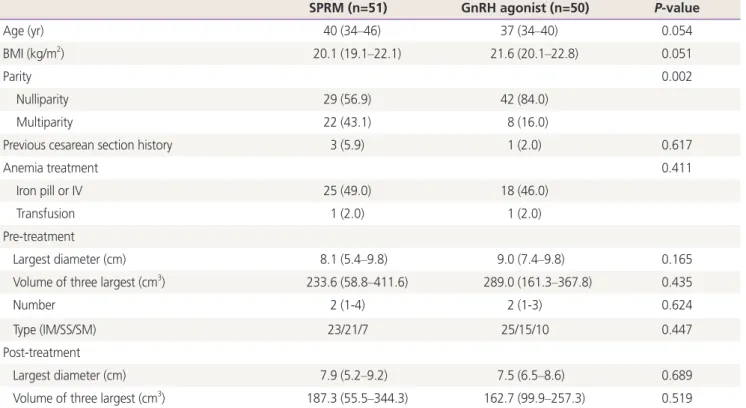
Uterine fibroid shrinkage after short-term use of selective progesterone receptor modulator or gonadotropin-releasing hormone agonist
5
0
0
전체 글
(2)
(3)
(4)
(5)
수치
관련 문서
In this study, a new immunocontraceptive vaccine composed of six tandem copies of gonadotropin-releasing hormone (GnRH) fused to rat granulocyte-macrophage
In this study as a first study to report the combination treatment of a GnRH agonist for 6 months plus 4 week du- ration of 10 romatise inhibitor in near menopause cases the result
The aim of the study was to evaluate the impact of body mass index (BMI) on luteinizing hormone (LH) secretion to gonadotro- pin-releasing hormone (GnRH) stimulation test in
Peng C, Fan NC, Ligier M, Vaananen J, Leung PCK Expression and regulation of gonadotropin-releasing hormone (GnRH) and GnRH receptor messenger ribonucleic acids in
This study was aimed to evaluate the efficacy of a single administration of long-act- ing gonadotrophin-releasing hormone agonist (GnRHa) as compared with daily administrations
Because prostate cancer shows androgen dependency in the early stages 1 , andro- gen-deprivation therapy with gonadotropin-releasing hor- mone (GnRH) agonists is the most
