introduction
Mucoid degeneration of the anterior cruciate ligament (ACL) has been implicated as one of the factors responsible for knee pain1-8). Kumar et al.3) first documented a case of biopsy indicated ACL mucoid degeneration in 1999. Contrary to the previous reports of the rarity of the lesion, recent studies have revealed relatively high prevalence9-12). Etiological factors of mucoid de- generation of the ACL include repeated trauma to the ACL or degeneration of the ligament, chronic impingement of the ACL,
synovial changes, and influence of anatomical variables such as the intercondylar notch of the knee and posterior tibial slope (PTS)9,10,13-17). In general, conservative treatment is the initial treatment of choice; however, if symptoms do not improve, ar- throscopic partial resection of the ACL can be performed11,18-20).
PTS is anatomically associated with anterior tibial translation, and it is positively correlated with anterior tibial translation, re- sulting in increased load on the ACL21,22). Studies have suggested there is a relationship between PTS and mucoid degeneration of the ACL and increased posterior slope has been associated with increased risk of ACL injury16,17,23,24).
The purpose of the current study was to investigate the relation- ship between mucoid degeneration of the ACL identified during total knee arthroplasty (TKA) and PTS.
materials and methods
This study was conducted on a total of 424 patients (636 knees) who underwent TKA under the diagnosis of Kellgren-Lawrence
Relationship between Mucoid Degeneration of the
Anterior Cruciate Ligament and Posterior Tibial Slope in Patients with Total Knee Arthroplasty
Yoon-Seok Youm, MD, Sung-Do Cho, MD, Hye-Yong Cho, MD, and Seung-Hyun Jung, MD
Department of Orthopedic Surgery, Ulsan University Hospital, Ulsan, Korea
purpose: The purpose was to analyze the relationship between posterior tibial slope (PTS) and mucoid degeneration of the anterior cruciate ligament (ACL) in patients with total knee arthroplasty.
materials and methods: Four hundred and twenty-four patients (24 males and 400 females; 636 knees) who received total knee arthroplasty for osteoarthritis were included. Their mean age was 68.9 years (range, 48 to 88 years). The patients were classified into three groups according to the status of ACL; normal ACL group (group I), mucoid degeneration of ACL group (group II) and ruptured or absent ACL group (group III). Plain lateral radiographs were used to measure the PTS and the values were compared among groups.
results: There were no significant differences with regard to gender, age and left-to-right side ratio among groups (p>0.05). The mean PTS was 9.9o (range, 0.6o to 20.1o) in group I (161 knees), 10.8o (range, 0.2o to 21.8o) in group II (342 knees) and 12.3o (range, 2o to 22.2o) in group III (133 knees), which showed significant differences (p<0.001).
conclusions: The patients with mucoid degeneration of the ACL and those with ruptured or absent ACL had greater PTS than those with normal ACL. These findings suggest that an increased PTS may be one of the causative factors for mucoid degeneration of the ACL.
Keywords: Knee, arthroplasty, posterior tibial slope, anterior cruciate ligament, mucoid degeneration pISSN 2234-0726 · eISSN 2234-2451
Knee Surgery & Related Research
Received July 27, 2015; Accepted September 9, 2015 Correspondence to: Sung-Do Cho, MD
Department of Orthopedic Surgery, Ulsan University Hospital, 877 Bangeojinsunhwan-doro, Dong-gu, Ulsan 44033, Korea
Tel: +82-52-250-7129, Fax: +82-52-235-2823 E-mail: [email protected]
34
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2016 KOREAN KNEE SOCIETY www.jksrr.org
grade IV osteoarthritis of the knee between May 2007 and Febru- ary 2011. There were 24 males and 400 females with a mean age of 68.9 years (range, 48 to 88 years). The exclusion criteria were previous surgery on the ipsilateral knee, lower limb deformity, mediolateral ligament instability, revision TKA, and rheumatoid arthritis.
The surgery was performed by the same surgeon (Cho SD) in all patients with a standard midline skin incision and a medial parapatellar approach. Intraoperatively, the presence of ACL de- generation/tear was identified and recorded by the same surgeon (Cho SD). Specimens obtained during surgery were histopatho- logically reviewed. The ultimate diagnosis of ACL mucoid degen- eration was based on the gross observation and histopathological findings. According to the diagnostic results, the patients were divided into three groups: group I, patients with normal ACL;
group II, patients with mucoid degeneration of ACL; and group III, patients with ruptured or absent ACL (Fig. 1).
PTS was assessed on the lateral radiograph using the picture ar- chiving communication system (PiView STAR software; Infinitt, Seoul, Korea) by an orthopedist who was blinded to patient data.
For the measurement of PTS, the diaphyseal axis of the tibia was established as a line connecting the two points equidistant from the anterior and posterior borders of the tibia, one was immedi- ately inferior to the tibial tubercle and the other was 10 cm more distal to it. A reference line was drawn perpendicular to the di- aphyseal axis at the level of the femorotibial joint. Then, another line was drawn by connecting the highest points of the anterior and posterior edges of the medial plateau. The angle between this line and the reference line was defined as the PTS (Fig. 2).
Statistical analysis was performed to determine statistical sig- nificance of difference in PTS among groups. A chi-square test was used to compare demographic characteristics among groups, and PTS was compared using the one-way analysis of variance test. The relationship between age and PTS in each group was as-
sessed using the Pearson correlation test. For statistical analysis, SPSS ver. 21.0 (IBM Co., Armonk, NY, US) was used with the significance level set at p<0.05.
results
Of the total 636 knees, ACL degeneration or tear was not ob- served in 161 knees (25.3%, group I), mucoid degeneration was observed in 341 knees (53.6%, group II), and the ACL was either ruptured or absent in 133 knees (20.9%, group III). There was no statistically significant difference among the groups with regard to gender, age, and the left-to-right side ratio (p>0.05) (Table 1).
The mean PTS was 9.9o (range, 0.6o to 20.1o) in group I, 10.8o (range, 0.2o to 21.8o) in group II, and 12.3o (range, 2o to 22.2o) in group III, showing statistically significant difference among groups (p<0.001) (Table 2).
A B C
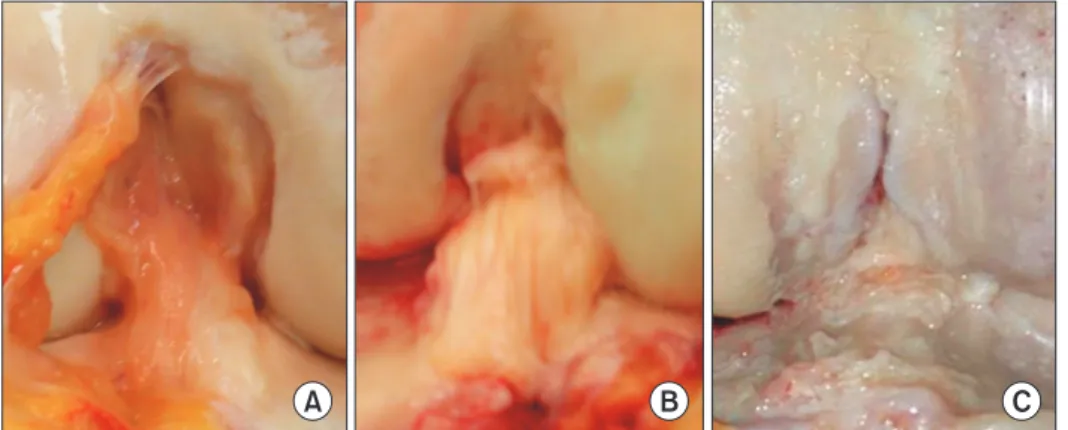
Fig. 1. Intraoperative gross appearance of the anterior cruciate ligament (ACL).
Normal (A), mucoid degeneration (B), and rupture or absence (C) of the ACL.
Fig. 2. Posterior tibial slope measurement.
Due to the comparatively low proportion of males in each group, statistical analysis of male-to-female comparison of PTS could not be carried out. Age was found to have no influence on PTS (p>0.05).
discussion
The results of the current study showed increased PTS in the knees with mucoid degeneration of the ACL or those with rup- ture or absence of the ligament compared to those with normal ACL.
Mucoid degeneration of the ACL can be diagnosed based on magnetic resonance imaging (MRI) findings, gross observations, and histopathological examinations. MRI characteristics of ACL mucoid degeneration include ill-defined and thickened ligament, increased signal intensity and celery stalk sign, and intraoperative
findings include ACL thickening, discharge of mucoid materials or loss of synovial lining, and impingement in full extension of the knee4,9,25,26). Histopatholoigcal indications are increased col- lagen production and alterations in mucoid materials17,25). In our study, intraoperative gross findings and histopathological exami- nations were used for the assessment of mucoid degeneration of the ACL, and MRI was not carried out.
PTS is measured as the angle between a line perpendicular to the mid-diaphysis of the tibia and a line parallel to posterior tibial inclination. A normal PTS ranges from 7o to 13o although some variations exist depending on the measurement site and meth- od27). Besides, the values on plain radiographs tend to be greater than those on MRI images28). PTS is positively correlated with an- terior tibial translation21,22). Based on a review of cadaveric studies and mathematical models, Feucht et al.27) concluded that PTS was positively correlated with anterior translation of the tibia;
however, the influence of anterior tibial shift on increased strain in the ACL could be confirmed only in mathematical models, not in cadaveric studies. In spite of this, they conjectured that a steep tibial posterior slope is a risk factor for ACL injuries. Some stud- ies have shown that PTS is greater in the ACL tear group than in the normal ACL group. Similarly, increased PTS was found to be associated with ACL injuries in a multitude of studies14,16,24,29). Table 1. Demographics
Variable Group I Group II Group III
Age (yr) 67.6±6.7 68.8±7.1 69.4±6.7
Gender
Male 5 20 7
Female 156 322 126
Side
Right 86 176 63
Left 75 166 70
Values are presented as mean±standard deviation or number.
Table 2. Posterior Tibial Slope (PTS)
Group I Group II Group III
PTS (o) 9.9±3.4 (0.6–20.1) 10.8±3.5 (0.2–21.8) 12.3±4.3 (2.0–22.2) Values are presented as mean±standard deviation (range).
A B
Fig. 3. (A) Relationship between poste- rior tibial slope (PTS) and anterior tibial translation. (B) Increased PTS may cause increased anterior tibial translation.
Based on the review of the abovementioned studies, we as- sumed a positive correlation between PTS and anterior transla- tion of the tibia, which predisposes the ACL to biomechanical alterations resulting in constant damage to the ACL and mucoid degeneration (Fig. 3). Jung et al.17) reported that PTS was signifi- cantly greater in the patient group with mucoid degeneration than in the control group. In our study, increased PTS was ob- served in the mucoid degeneration group (group II) and absent or torn ACL group (group III) compared to the normal ACL group (group I). In addition, the PTS was significantly greater in group III than in group II, suggesting that mucoid degeneration can eventually progress to a tear or loss of the ACL. Therefore, in the absence of clear understanding of the mechanism, we surmise there is a relatively close relationship between PTS and mucoid degeneration of the ACL. It is our understanding that the possibility of ACL injury or mucoid degeneration should be taken into consideration if a steep PTS is observed during clinical examination.
We acknowledge there are some limitations or our study. First, the influence of meniscus on the PTS was not addressed in the analysis because measurements were performed using plain radiographs. Second, other factors that could affect mucoid de- generation were not investigated. Third, we did not attempt to identify the exact mechanism of mucoid degeneration.
conclusions
The patients with mucoid degeneration of the ACL and those with ruptured or absent ACL had greater PTS than those with normal ACL. These findings suggest that an increased PTS may be one of the causative factors for mucoid degeneration of the ACL.
conflict of interest
No potential conflict of interest relevant to this article was re- ported.
references
1. Fealy S, Kenter K, Dines JS, Warren RF. Mucoid degenera- tion of the anterior cruciate ligament. Arthroscopy. 2001;17:
E37.
2. Hsu CJ, Wang SC, Fong YC, Huang CY, Chiang IP, Hsu HC.
Mucoid degeneration of the anterior cruciate ligament. J Chin Med Assoc. 2006;69:449-52.
3. Kumar A, Bickerstaff DR, Grimwood JS, Suvarna SK. Mu- coid cystic degeneration of the cruciate ligament. J Bone Joint Surg Br. 1999;81:304-5.
4. McIntyre J, Moelleken S, Tirman P. Mucoid degeneration of the anterior cruciate ligament mistaken for ligamentous tears. Skeletal Radiol. 2001;30:312-5.
5. Melloni P, Valls R, Yuguero M, Sáez A. Mucoid degeneration of the anterior cruciate ligament with erosion of the lateral femoral condyle. Skeletal Radiol. 2004;33:359-62.
6. Motmans R, Verheyden F. Mucoid degeneration of the anterior cruciate ligament. Knee Surg Sports Traumatol Ar- throsc. 2009;17:737-40.
7. Narvekar A, Gajjar S. Mucoid degeneration of the anterior cruciate ligament. Arthroscopy. 2004;20:141-6.
8. Nishimori M, Sumen Y, Sakaridani K. Mucoid degeneration of the anterior cruciate ligament: a report of two cases. Magn Reson Imaging. 2004;22:1325-8.
9. Kim TH, Lee DH, Lee SH, Kim JM, Kim CW, Bin SI. Ar- throscopic treatment of mucoid hypertrophy of the anterior cruciate ligament. Arthroscopy. 2008;24:642-9.
10. Kwee RM, Ahlawat S, Kompel AJ, Morelli JN, Fayad LM, Zi- kria BA, Demehri S. Association of mucoid degeneration of anterior cruciate ligament with knee meniscal and cartilage damage. Osteoarthritis Cartilage. 2015;23:1543-50.
11. Cha JR, Lee CC, Cho SD, Youm YS, Jung KH. Symptomatic mucoid degeneration of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2013;21:658-63.
12. Salvati F, Rossi F, Limbucci N, Pistoia ML, Barile A, Mas- ciocchi C. Mucoid metaplastic-degeneration of anterior cru- ciate ligament. J Sports Med Phys Fitness. 2008;48:483-7.
13. Cha JH, Lee SH, Shin MJ, Choi BK, Bin SI. Relationship be- tween mucoid hypertrophy of the anterior cruciate ligament (ACL) and morphologic change of the intercondylar notch:
MRI and arthroscopy correlation. Skeletal Radiol. 2008;37:
821-6.
14. Diard F, Chateil JF, Hauger O, Moinard M. Para-articular and intraosseous synovial cysts and articular mucoid cysts. J Radiol. 1999;80(6 Suppl):679-96.
15. Rolf C, Watson TP. Case report: intra-tendinous ganglion of the anterior cruciate ligament in a young footballer. J Orthop Surg Res. 2006;1:11.
16. Sonnery-Cottet B, Archbold P, Cucurulo T, Fayard JM, Bor- tolletto J, Thaunat M, Prost T, Chambat P. The influence of the tibial slope and the size of the intercondylar notch on rupture of the anterior cruciate ligament. J Bone Joint Surg Br. 2011;93:1475-8.
17. Jung KH, Cho SD, Park KB, Youm YS. Relation between mucoid degeneration of the anterior cruciate ligament and posterior tibial slope. Arthroscopy. 2012;28:502-6.
18. Morice A, Coupry A, Lintz F, Robert H. Reduction plasty for hypertrophic anterior cruciate ligament mucoid degenera- tion: clinical and knee laxity outcomes in 23 cases. Orthop Traumatol Surg Res. 2013;99:693-7.
19. Chudasama CH, Chudasama VC, Prabhakar MM. Ar- throscopic management of mucoid degeneration of anterior cruciate ligament. Indian J Orthop. 2012;46:561-5.
20. Lintz F, Pujol N, Dejour D, Boisrenoult P, Beaufils P. Anterior cruciate ligament mucoid degeneration: selecting the best treatment option. Orthop Traumatol Surg Res. 2010;96:400-6.
21. Dejour H, Bonnin M. Tibial translation after anterior cru- ciate ligament rupture: two radiological tests compared. J Bone Joint Surg Br. 1994;76:745-9.
22. Giffin JR, Vogrin TM, Zantop T, Woo SL, Harner CD. Ef- fects of increasing tibial slope on the biomechanics of the knee. Am J Sports Med. 2004;32:376-82.
23. Brandon ML, Haynes PT, Bonamo JR, Flynn MI, Barrett GR, Sherman MF. The association between posterior-infe- rior tibial slope and anterior cruciate ligament insufficiency.
Arthroscopy. 2006;22:894-9.
24. Zeng C, Cheng L, Wei J, Gao SG, Yang TB, Luo W, Li YS, Xu M, Lei GH. The influence of the tibial plateau slopes on in- jury of the anterior cruciate ligament: a meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2014;22:53-65.
25. Makino A, Pascual-Garrido C, Rolon A, Isola M, Muscolo DL. Mucoid degeneration of the anterior cruciate ligament:
MRI, clinical, intraoperative, and histological findings. Knee Surg Sports Traumatol Arthrosc. 2011;19:408-11.
26. Lintz F, Pujol N, Boisrenoult P, Bargoin K, Beaufils P, Dejour D. Anterior cruciate ligament mucoid degeneration: a review of the literature and management guidelines. Knee Surg Sports Traumatol Arthrosc. 2011;19:1326-33.
27. Feucht MJ, Mauro CS, Brucker PU, Imhoff AB, Hinterwim- mer S. The role of the tibial slope in sustaining and treating anterior cruciate ligament injuries. Knee Surg Sports Trau- matol Arthrosc. 2013;21:134-45.
28. Hudek R, Schmutz S, Regenfelder F, Fuchs B, Koch PP. Novel measurement technique of the tibial slope on conventional MRI. Clin Orthop Relat Res. 2009;467:2066-72.
29. Todd MS, Lalliss S, Garcia E, DeBerardino TM, Cameron KL.
The relationship between posterior tibial slope and anterior cruciate ligament injuries. Am J Sports Med. 2010;38:63-7.