TKA include preoperative ROM1-6), implant design1,2,5,7), posterior femoral condylar offset (FCO)8-11), intraoperative soft tissue balancing2,4,12), and posterior tibial slope (PTS)11,13-15).
In particular, the influence of FCO and PTS on ROM after TKA with posterior cruciate ligament (PCL)-retaining and -substituting prostheses has been amply demonstrated in a variety of studies8,9,11,14-18), whereas it has been rarely addressed in studies involving PCL-sacrificing TKAs characterized by the use of deep-dish polyethylene components for stability10,13).
The purpose of this study was to evaluate the influence of FCO and PTS on ROM after PCL-sacrificing TKA using a medial pivot prosthesis.
Materials and Methods
1. Materials
Of the patients who underwent PCL-sacrificing TKA using a
Effect of Posterior Femoral Condylar Offset and
Posterior Tibial Slope on Maximal Flexion Angle of the Knee in Posterior Cruciate Ligament Sacrificing Total Knee Arthroplasty
Jong-Heon Kim, MD
Department of Orthopedic Surgery, Hanyang University College of Medicine, Guri, Korea pISSN 2234-0726 · eISSN 2234-2451
Knee Surgery & Related Research
Purpose: To evaluate the effect of femoral condylar offset and posterior tibial slope on maximal flexion angle of the knee in posterior cruciate ligament (PCL)-sacrificing total knee arthroplasty (TKA, Medial-Pivot Knee System).
Materials and Methods: Forty-five knees in 35 patients who could be followed up more than 1 year after PCL-sacrificing TKA were evaluated retrospectively. We measured and analyzed the preoperative and postoperative maximal flexion angle, posterior femoral condylar offset difference, posterior femoral condylar offset ratio difference, and tibial slope.
Results: The mean maximal flexion angle after TKA was 118.44o±9.8o and significantly related to postoperative tibial slope (11.78o±6.2o) in correlation analysis (R=0.451, p=0.002). There was no statistical relationship between the postoperative maximal flexion angle and the posterior femoral condylar offset difference (3.24±3.862 mm, R=0.105, p=0.493) and posterior femoral condylar offset ratio difference (0.039±0.029 mm, R=
-0.163, p=0.284).
Conclusions: The maximal flexion angle of the knee after PCL-sacrificing TKA was significantly related to the postoperative tibial slope. Therefore, posterior tibial slope can be considered as a factor that affects maximal flexion angle after PCL-sacrificing TKA.
Keywords: Maximal flexion angle, Posterior femoral offset, Posterior femoral offset ratio, Posterior tibial slope, Cruciate-sacrificing total knee arthroplasty
Received September 20, 2012; Revised (1st) November 5, 2012;
(2nd) March 13, 2013; Accepted April 10, 2013 Correspondence to: Jong-Heon Kim, MD
Department of Orthopedic Surgery, Hanyang University Guri Hospital, 153 Gyeongchun-ro, Guri 471-701, Korea
Tel: +82-31-560-2313, Fax: +82-31-557-8781 E-mail: [email protected]
Introduction
The primary goal of total knee arthroplasty (TKA) is to reduce joint pain in standing and walking and maintain range of motion (ROM) to facilitate the ability to perform daily living activities.
Factors that have been associated with the change in ROM after
54
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2013 KOREAN KNEE SOCIETY www.jksrr.org
medial pivot prosthesis (Advance Medial-Pivot Knee System, Wright Medical Group Inc., Memphis, TN, USA) performed by the same surgeon at our institution between September 2005 and June 2009, 35 patients (45 knees) who were available for more than 1-year follow-up were included in this study. The mean age of the patients at the time of surgery was 68.6±7.2 years, ranging from 54 to 84 years. There were 32 females (40 knees) and 3 males (5 knees). The diagnosis was osteoarthritis in 42 knees and rheumatoid arthritis in 3 knees. The mean follow-up period was 20.8 months.
2. Methods
1) Surgical technique
All the operations were performed using the medial parapa- tellar approach. The PCL was resected in all knees. The extent of femoral resection was determined as the thickness of the distal femoral prosthesis and anteroposterior resection was performed for insertion of a prosthesis that best approximates the anteroposterior diameter of the femur measured intraoperatively.
The rotational alignment of the femoral component was obtained with reference to the Whiteside’s line, transepicondylar axis, and posterior condylar axis. Tibial resection was performed to produce 7o to 10o of postoperative PTS irrespective of the previous value. Flexion-extension gap imbalance, varus/valgus or anterior/posterior instability, or malalignment was not observed in any of the patients at the last follow-up. Postoperative rehabilitation protocol included passive motion exercises using a continuous passive motion machine from the first postoperative day and progressive weight bearing in a walker.
2) Radiographic assessment
On the ROM assessment, the patient was asked to flex the knee in the supine position and the maximal flexion angle was measured using a one-degree increment goniometer preoperatively and at the last follow-up. Lateral views of the
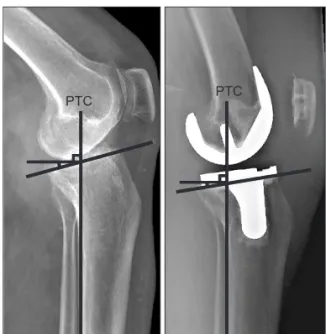
knee with superimposition of the femoral condyles were obtained by plain radiography preoperatively and fluoroscopic radiography postoperatively. Pre- and postoperative PTS measurements were performed using the posterior tibial cortex as a reference according to one of the six methods suggested by Braizier et al.19). The inclination angle between the line drawn perpendicular to the tangent of the posterior tibial cortex and the tangent to the tibial plateau was recorded as the preoperative PTS and the angle created with the tangent to the tibial cut surface as the postoperative PTS (Fig. 1). The FCO was measured as the distance from the tangent of the femoral diaphysis posterior cortex to the apex of the posterior femoral condyle preoperatively and to the apex of the posterior femoral component postoperatively (Fig. 2). The pre- and postoperative FCO difference was defined as the postoperative value minus preoperative value. All measurements were performed twice and the mean values were used for data analysis (Cronbach’s α; pre-
Fig. 1. Preoperative and postoperative radiographs showing the methods of determining posterior tibial slope. PTC: posterior tibial cortex.
PTC PTC
Fig. 2. Preoperative and postoperative radiographs showing measurements of femoral condylar offset. PFC: posterior femoral cortex.
PFC
PFC
and postoperative PTS: 0.987/0.989, pre- and postoperative FCO:
0.980/0.973).
To adjust the source-to-image distance difference of the pre- and postoperative radiographs and obtain relative FCO ratio (FCOR), pre- and postoperative FCOR was calculated according to the method of Soda et al.20) by dividing the FCO value by the distance from the femoral diaphysis anterior cortex to the posterior femoral condyle (Fig. 3). The difference between the pre- and postoperative FCORs was defined as the value obtained by subtracting the preoperative FCOR from the postoperative FCOR.
3) Statistical analysis
To determine the relationship between the preoperative and postoperative values, linear/multiple logistic regression analyses were performed using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was set at p<0.05.
Fig. 3. Preoperative and postoperative radiographs showing measurement of femoral condylar offset ratio (FCOR=PFC/
AFC). AFC: anterior femoral cortex, PFC:
posterior femoral cortex.
PFC
PFC AFC AFC
Fig. 4. The graph shows the correlation between posterior tibial slope and postoperative maximal flexion angle (R=0.451, p=0.002). MFA:
maximal flexion angle of the knee.
Fig. 5. The graph shows the correlation between posterior condylar offset and postoperative maximal flexion angle (R=0.105, p=0.493).
MFA: maximal flexion angle of the knee, dPCO: difference of posterior condylar offset.
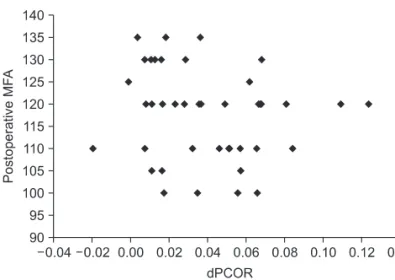
Fig. 6. The graph shows the correlation between posterior condylar offset ratio and postoperative maximal flexion angle (R=-0.163, p=0.284). MFA: maximal flexion angle of the knee, dPCOR: difference of posterior condylar offset ratio.
Results
The mean postoperative maximal flexion angle was 118.44o
±9.8o, which showed a significant correlation with the postoper- ative PTS (11.78o±3.9o; R=0.451, p=0.002) (Fig. 4). The mean preoperative and postoperative FCO was 24.78±2.243 mm and 28.11±4.50 mm, respectively. The mean preoperative and postoperative FCOR was 0.387±0.036 and 0.415±0.032, respectively. Thus, the mean difference in the pre- and postoperative FCO was 3.2±3.862 mm (R=0.105, p=0.493) and the mean difference in the pre- and postoperative FCOR was 0.039±0.029 (R=-0.163, p=0.284), which showed no significant relationship with the postoperative maximal flexion angle (Figs. 5 and 6).
Discussion
In this study, we investigated the influence of PTS and FCO on ROM after TKA using a PCL-sacrificing medial pivot knee implant. The study results showed a correlation between PTS and ROM as in the case of PCL-retaining TKA, whereas no relationship was found between FCO and ROM as in the case of PCL-substituting TKA.
ROM after TKA using a medial pivot knee system designed based on the concept of medial-pivoting of the knee during flexion21,22) has been documented in a variety of domestic and international research23-29). The mean maximal flexion angle of 118.44o that was obtained in our patients is comparable to the values reported in those studies.
The impact of PTS11,14,15,17) and FCO8-11) on ROM, such as maximal flexion angle, after TKA has been the subject of controversy. Bellemans et al.17) reported that 1o of extra PTS resulted in an average of 1.7o increase in maximal knee flexion after PCL-retaining TKA based on the assessment of knees with 0o, 4o, and 7o PTS. In a study by Malviya et al.18), 1o of additional PTS increased the maximal flexion angle by an average of 2.3o in 101 knees after PCL-retaining TKA. On the other hand, Kansara and Markel14) and Piazza et al.15) showed that there was no difference in the postoperative ROM between the knees with 0o and 5o of PTS after PCL-sacrificing TKA. Bauer et al.13) reported that the correlation between PTS and maximal knee flexion that can be observed after PCL-retaining TKA was not noted after PCL-sacrificing TKA. In this study, a statistically significant positive correlation was found between PTS and maximal flexion angle after PCL-sacrificing TKA using a medial pivot implant.
The study by Bellemans et al.8) suggested a significant
correlation between FCO and maximal knee flection in 150 arthroplasties of the knee; every 1 mm decrease in FCO led to a 6.1o reduction in postoperative maximal flexion. Goldstein et al.9) reported that reduced FCO due to downsizing of the femoral component resulted in a loss of flexion from 135o to 120o after PCL-retaining TKA. In contrast, according to the analysis of 69 cases of PCL-sacrificing TKA by Hanratty et al.10) and 410 cases by Bauer et al.13), FCO was not significantly related to maximal knee flexion. In a study by Arabori et al.16), bilateral TKA (PCL- retaining on one side and PCL-sacrificing on the other side) results showed that FCO was correlated with flexion angle in PCL-retaining knees but not in PCL-sacrificing knees. In the current study, we used the method of Soda et al.20) designed to obtain relative FCOR in order to minimize error in the pre- and postoperative FCO and FCOR comparison; however, we could not find any correlation between the postoperative maximal flexion angle and FCO and FCOR (R=0.105, p=0.493, R=-0.163, p=0.284).
In conclusion, a correlation between the postoperative PTS and maximal flexion angle can be found after PCL-sacrificing TKA using a medial pivot implant as well as PCL-retaining TKA, whereas no relationship can be observed between the FCO and FCOR difference and knee flexion after PCL-sacrificing TKA as well as PCL-substituting TKA. It is our understanding that the design characteristics of the PCL-sacrificing medial pivot Knee system that has a larger contact area in the medial compartment compared to the PCL-substituting knee implants could contribute to the correlation between PTS and flexion range.
The limitations of this study include the retrospective study design, lack of comparison with other implants with a deep- dish polyethylene component, the possibility of inaccurate measurement of the maximal flexion angle, and intraoperative balancing of soft tissue structures. In addition, we believe other potential factors that may affect the maximal flexion angle, such as implant design, should be addressed in future studies.
Conclusions
Maximal flexion angle of the knee after PCL-sacrificing TKA was correlated with PTS. However, the pre- and postoperative differences in the FCO and FCOR were not related to the flexion angle. Therefore, we believe PTS is a factor that influences maximal flexion angle after PCL-sacrificing TKA.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
References
1. Ranawat CS. Design may be counterproductive for optimizing flexion after TKR. Clin Orthop Relat Res. 2003;
(416):174-6.
2. Dennis DA, Komistek RD, Scuderi GR, Zingde S. Factors affecting flexion after total knee arthroplasty. Clin Orthop Relat Res. 2007;464:53-60.
3. Higuchi H, Hatayama K, Shimizu M, Kobayashi A, Koba- yashi T, Takagishi K. Relationship between joint gap differ- ence and range of motion in total knee arthroplasty: a prospective randomised study between different platforms.
Int Orthop. 2009;33:997-1000.
4. Kotani A, Yonekura A, Bourne RB. Factors influencing range of motion after contemporary total knee arthroplasty.
J Arthroplasty. 2005;20:850-6.
5. Kurosaka M, Yoshiya S, Mizuno K, Yamamoto T. Maximiz- ing flexion after total knee arthroplasty: the need and the pitfalls. J Arthroplasty. 2002;17(4 Suppl 1):59-62.
6. Ritter MA, Berend ME, Harty LD, Davis KE, Meding JB, Keating EM. Predicting range of motion after revision total knee arthroplasty: clustering and log-linear regression analyses. J Arthroplasty. 2004;19:338-43.
7. Bin SI, Nam TS. Early results of high-flex total knee arthroplasty: comparison study at 1 year after surgery. Knee Surg Sports Traumatol Arthrosc. 2007;15:350-5.
8. Bellemans J, Banks S, Victor J, Vandenneucker H, Moemans A. Fluoroscopic analysis of the kinematics of deep flexion in total knee arthroplasty. Influence of posterior condylar offset. J Bone Joint Surg Br. 2002;84:50-3.
9. Goldstein WM, Raab DJ, Gleason TF, Branson JJ, Berland K.
Why posterior cruciate-retaining and substituting total knee replacements have similar ranges of motion: the importance of posterior condylar offset and cleanout of posterior condylar space. J Bone Joint Surg Am. 2006;88 Suppl 4:182-8.
10. Hanratty BM, Thompson NW, Wilson RK, Beverland DE.
The influence of posterior condylar offset on knee flexion after total knee replacement using a cruciate-sacrificing mobile-bearing implant. J Bone Joint Surg Br. 2007;89:915-8.
11. Massin P, Gournay A. Optimization of the posterior condy- lar offset, tibial slope, and condylar roll-back in total knee
arthroplasty. J Arthroplasty. 2006;21:889-96.
12. Wyss T, Schuster AJ, Christen B, Wehrli U. Tension con- trolled ligament balanced total knee arthroplasty: 5-year results of a soft tissue orientated surgical technique. Arch Orthop Trauma Surg. 2008;128:129-35.
13. Bauer T, Biau D, Colmar M, Poux X, Hardy P, Lortat-Jacob A.
Influence of posterior condylar offset on knee flexion after cruciate-sacrificing mobile-bearing total knee replacement:
a prospective analysis of 410 consecutive cases. Knee.
2010;17:375-80.
14. Kansara D, Markel DC. The effect of posterior tibial slope on range of motion after total knee arthroplasty. J Arthroplasty.
2006;21:809-13.
15. Piazza SJ, Delp SL, Stulberg SD, Stern SH. Posterior tilting of the tibial component decreases femoral rollback in posterior- substituting knee replacement: a computer simulation study.
J Orthop Res. 1998;16:264-70.
16. Arabori M, Matsui N, Kuroda R, Mizuno K, Doita M, Kuro- saka M, Yoshiya S. Posterior condylar offset and flexion in posterior cruciate-retaining and posterior stabilized TKA. J Orthop Sci. 2008;13:46-50.
17. Bellemans J, Robijns F, Duerinckx J, Banks S, Vandenneucker H. The influence of tibial slope on maximal flexion after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2005;13:193-6.
18. Malviya A, Lingard EA, Weir DJ, Deehan DJ. Predicting range of movement after knee replacement: the importance of posterior condylar offset and tibial slope. Knee Surg Sports Traumatol Arthrosc. 2009;17:491-8.
19. Brazier J, Migaud H, Gougeon F, Cotten A, Fontaine C, Duquennoy A. Evaluation of methods for radiographic measurement of the tibial slope: a study of 83 healthy knees.
Rev Chir Orthop Reparatrice Appar Mot. 1996;82:195-200.
20. Soda Y, Oishi J, Nakasa T, Nishikawa K, Ochi M. New parameter of flexion after posterior stabilized total knee arthroplasty: posterior condylar offset ratio on X-ray photographs. Arch Orthop Trauma Surg. 2007;127:167-70.
21. Iwaki H, Pinskerova V, Freeman MA. Tibiofemoral move- ment 1: the shapes and relative movements of the femur and tibia in the unloaded cadaver knee. J Bone Joint Surg Br.
2000;82:1189-95.
22. Moonot P, Mu S, Railton GT, Field RE, Banks SA. Tibio- femoral kinematic analysis of knee flexion for a medial pivot knee. Knee Surg Sports Traumatol Arthrosc. 2009;17:927-34.
23. Bae DK, Yoon KH, Kim SG, Park KJ. Cruciate retaining medial pivot knee. J Korean Orthop Assoc. 2007;42:71-6.
24. Cho SD, Youm YS, Jeong JY, Park KB. Total knee arthro- plasty with PCL substituting medial pivot knee: short-term follow-up results. J Korean Knee Soc. 2009;21:45-50.
25. Lee S, Ko DO, Kim JH, Jeon YW, Kim KS, Kim TW. Total knee arthroplasty using a medial pivot knee: minimum 2-year follow-up results. J Korean Knee Soc. 2008;20:77-82.
26. Mont MA, Booth RE Jr, Laskin RS, Stiehl JB, Ritter MA, Stuchin SA, Rajadhyaksha AD. The spectrum of prosthesis design for primary total knee arthroplasty. Instr Course Lect.
2003;52:397-407.
27. Schmidt R, Komistek RD, Blaha JD, Penenberg BL, Maloney
WJ. Fluoroscopic analyses of cruciate-retaining and medial pivot knee implants. Clin Orthop Relat Res. 2003;(410):139- 47.
28. Shakespeare D, Kinzel V, Ledger M. Achieving ligament stability and correct rotational alignment of the femur in knee arthroplasty: a study using the Medial Pivot knee.
Knee. 2005;12:419-23.
29. Shakespeare D, Ledger M, Kinzel V. Flexion after total knee replacement: a comparison between the Medial Pivot knee and a posterior stabilised implant. Knee. 2006;13:371-3.