Neurofibromatosis Type 2와 무관하게 발생된 척추 경막내 다발성 신경초종 *
- 증 례 보 고 -
단국대학교 의과대학 신경외과학교실
김정태·성정남·박봉진·조맹기·김영준
= Abstract =
Multiple Spinal Intradural Schwannomas in the Absence of Neurofibromatosis Type 2 Manifestations
- -
- - A Case Report - - - -
Jung Tae Kim, M.D., Jung Nam Sung, M.D., Bong Jin Park, M.D., Maeng Ki Cho, M.D., Young Joon Kim, M.D.
Department of Neurosurgery, College of Medicine, Dankook University, Cheonan, Korea
ost extracranial schwannomas are solitary, but neurofibromas are frequently associated with other manie- tations of neurofibromatosis. Schwannomas that occur within the context of neurofibromatosis tend to be multiple, but multiple schwannomas without manifestation of neurofibromatosis type 2 are very rare. The authors report a very rare case of multiple spinal intradural schwannomas in the absence of neurofibromatosis Type 2 mani- estations.
A 40-year-old man suffered from longstanding low back pain and left side sciatica which was treated with two stage operations. MRI showed multiple intradural mass lesions extending from L1 vertebral segment to S1 vertebral segment. There were no clinical and radiological manifestations of Type 2 neurofibromatosis.
Histologically confirmed diagnosis was schwannoma.
KEY WORDS:Spinal tumor・Multiple schwannomas・Neurofibromatosis type 2.
서 론
신경초종은 척추강내 종양중 가장 많은 발생빈도를 보이 며 주로 경막내수외(intradural-extramed ullary)에 발생 하는 종양이다. Schwann 세포에서 기원하며 척추에 발생하 는 경우 감각 신경근에서 기원하는 종양으로 주위조직과 경 계가 분명한 피막에 쌓여있다.
신경초종증(schwannomatosis or neurilemmomatosis) 은 양측성 청신경종양 및 신경섬유종증의 특징적인 다른 증 후들을 동반하지 않는 다발성 신경초종으로 정의된다
14).
신경초종은 주로 단일 병변으로 발생하며 드물게 다발성으 로 발생하는데 다발성으로 발생되는 경우 신경섬유종증 Type 2와 동반되는 경우가 대부분이며 신경섬유종증 Type 2를 동반하지 않는 다발성 신경초종은 매우 드물다
7).
저자들은 청신경종양 및 신경섬유종증을 동반하지 않은 요추와 천추부위에 발생한 각기 다른 신경근 기원의 다발성 신경초종을 수술적으로 치험 하고 문헌고찰과 함께 보고하 고자 한다.
증 례
38세 남자환자로 내원 9개월 전부터 하부요통과 좌측 하 지방사통이 발생하여 간헐적 대증적 치료를 받아왔으며 내
M M M M
*본 논문은 1997년 춘계학회 포스터 발표 논문임.
원 5개월 전부터 하부요통이 점점 심해졌고, 최근 배뇨후 잔뇨감을 느끼게 되어 외래를 방문하여 요천추부 자기공명 영상소견상 척추내 종양 진단하에 입원하였다.
과거력상 내과적 질환이나 종양성 병변, 수술 병력, 난청, 시력장애 및 가족력에서도 특이소견은 없었다.
이학적 검사상 피부의 색소침착이나 탈색, 피하 결절 등 은 관찰할 수 없었으며 안저검사에서도 정상소견을 보였다.
신경학적 검사상 하지 직거상 검사에서 좌측에서 70℃의 제한을 관찰할 수 있었으며, 좌측 제1족지와 족관절의 배굴 (dorsiflexion)의 약화를 보였고, 심부 건반사는 좌측 과반 사(ankle jerk)가 저하된 소견을 보였다. Barbinski 증후나 족간대(ankle clonus) 등의 병적 반사는 관찰되지 않았다.
배뇨후 잔뇨감을 호소하였으나 도관으로 검사한 결과 잔뇨 는 확인되지 않았다.
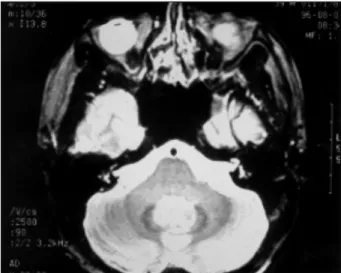
요추-천추 단순 X-선 촬영상 특이소견은 보이지 않았 고, 척수조영술 소견상 제5요추에서 제1천추부위에 걸쳐 비 교적 조영제 주(contrast column)와의 경계가 명확한 원형 충만 결손을 보이는 경막내수외 종괴를 보였다. 척추 자기 공명영상에서 제1요추부에서 제1천추부에 걸쳐 독립된 다 발성의 경막내 종양들의 소견을 보였고 제5요추부에서 제1
천추부에 발생된 종양은 크고 중앙에 괴사병변이 관찰되었 는데 종양은 T1 강조영상에서 저신호강도, T2 강조영상에 서 고신호강도를 보였으며 조영제 주입시 강한 조영증강을 보였다(Fig. 1). 뇌 자기공명영상에서 양측 청신경부위에 종 양의 소견은 없었다(Fig. 2).
Fig. 1. Left:Preoperative lumbosacral sagittal MRI image showing multiple intradural mass lesions extending from L1 ver- tebral segment to S1 vertebral segment. Multiple lesions are low signal intensity in precontrast T1-weighted image and postcontrast T1-weighted image showing strong enhancement. Right:Postoperative MRI image showing total removal of tumor masses with postoperative change.
Fig. 2. A T2-weighted axial brain MRI image showing no tu-
morous lesions at bilateral cerebellopontine angles.
수술은 5개월 간격으로 두차례 시행하였다. 1차수술은 제 5요추-제1천추에 걸쳐있는 종괴를 후궁절제와 정중 천추 능절제를 통하여 접근하였다. 수술 소견에서 여러 개의 각 기 다른 신경근 기원의 종괴를 발견하고 신경근과 함께 모 두 제거하였다. 종괴는 주위조직과 경계가 분명한 피막으로
쌓여 있었고 신경근과는 박리되지 않았다. 신경근의 전기적 자극에 하지 근육은 반응을 보이지 않았다. 2차수술은 5개 월 후에 제1요추에서 제4요추부위까지의 종괴를 부분 척추 궁 절제술을 통한 접근법으로 모두 제거하였다. 수술소견에 서 제1요추에서부터 제4요추에 걸쳐 황색조의 각기 다른 신경근 기원의 다발성 종괴가 주위조직의 침윤없이 경계가 잘 구분되는 피막으로 쌓여 있었다. 종양은 최대지름 2cm 부터 매우 작은 크기까지 다양하였다(Fig. 3).
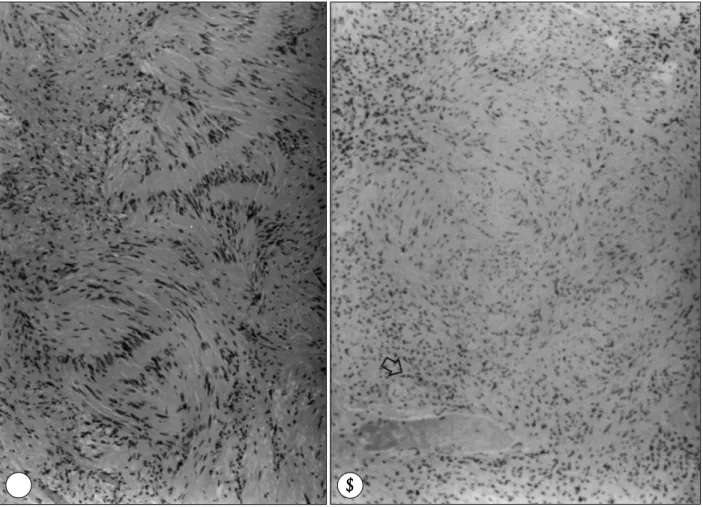
조직병리 소견에서 세포핵은 난원형으로 호산성으로 염색 이 되는 색화체를 가지고 있었고 Antoni A형과 Antoni B 형을 모두 포함하고있는 신경초종으로 진단되었다(Fig. 4).
수술후 환자는 특별한 합병증 및 신경학적 후유증없이 퇴 원하였고 10개월 후 시행한 추적 자기 공명영상에서 잔존 종양이나 종양의 재발은 없었다(Fig. 1).
고 찰
대부분의 다발성 신경초종은 신경섬유종증 Type 2와 함
Fig. 4. Light microscopic exam showing typical arrangement of spindle cells of neurilemmoma. Compact cellular Antoni A area(A) and hypocellular zone of Antoni B(B) area also seen(H & E). Antoni A containing focal nodular pallisading nuclei and central resions of Schwann cell cytoplasm(Verocay body)(H & E). Antoni B containing thickened blood vessels with hyalinized necrosis and hemosiderin raden macrophages(arrow)(H & E).
Fig. 3. Intraoperative findings under operating microscope showing numerous nodular yellowish masses attac- hed to the nerve roots along the rootlets.
A A
A A B B B B
께 발생되며 신경섬유종증 Type 1에서 신경초종이 발생되 는 경우는 극히 드물다
2-4)7)10)14).
신경초종증은 매우 드문 질환으로 1995년에 Honda 등
5)에 의해 이 질환의 종양세포 및 주변 백혈구에서 신경섬유 종증 Type 2 유전자의 germline mutation이 발견되어 신 경섬유종증 Type 2의 불완전 형태라고 보고하였다
11).
신경섬유종증은 출생인구 4만명당 1명에서 발병하는 비 교적 흔한 상염색체 우성유전질환의 하나로 임상적, 유전학 적으로 2개의 형태로 발현되는데 첫째는 17번 염색체에 유 전자가 위치한 신경섬유종증 Type 1이며 둘째는 22번 염 색체에 유전자를 가진 신경섬유종증 Type 2이다. 이 유전 자들은 종양억제인자로 이들의 기능상실로 neurofibromin 과 merlin이라는 단백질을 만들어낸다
1)4-8).
전형적인 신경섬유종증 Type 2는 양측성 청신경 종양이 발생한 환자나, 신경섬유종증 환자가있는 직계가족에서 발 생되는데 이 질환의 증상은 대부분 청신경종양에 의해 발생 하며 척추종양에 의해 발현되는 경우는 드물다
14). 신경섬유 종증 Type 2는 특징적 피부병변 및 안과적 질환을 동반하 며 두개, 척추, 말초신경 등의 신경초종과 두개강, 척추강내 수막종이 동반되기도 한다. 본 환자는 가족력상 직계가족에 서 신경섬유종증의 기왕력은 없었으며 뇌 자기공명영상 소 견상 청신경종양 및 다른 두개강내 종양을 동반하지 않았으 며 처음 증상은 척추병변에 의해 발생하였다. 신경섬유종증 Type 2에서 발견되는 안과적 질환인 retinal astrocyto- mas, posterior subcapsular cataracts의 소견은 없었으며 피부의 탈색, 색소침착, 결절 등의 소견 또한 보이지 않았다.
조직병리학적으로 신경초종은 방추상핵을 갖고있는 양극 방추형 세포가 조밀하게 결합배열되고 은친화성 원섬유가 관찰되며 종양세포가 규칙적인 단을 형성하여 책상배열을하 는 Antoni A형과 다형태세포가 소성배열을 하며 단형성이 나 책상배열은 볼 수 없는 Antoni B형으로 구분된다. 신경 섬유종은 조직병리학적으로 말초신경의 세포성분 즉 축삭돌 기, 섬유모세포, schwann 세포가 다양하게 증식되어 있는 소성구조를 보이고 길고 점차 가늘어져 끝이 뾰족한 세포가 파상배열을 하고 있다
9)12)13).
보고에 따르면 신경초종증은 신경섬유종증 Type 2의 불 완전한 변형으로 임상적, 유전적 표현형이 각기 다른 질환 으로 생각되어지고 있다
4)7)9).
결 론
신경섬유종증 Type 2를 동반하지 않는 척추내에 발생한 다발성 신경초종은 매우 드문 질환으로, 본 교실에서는 신
경섬유종증, 신경초종의 가족력이 없는 요추와 천추부위에 다발성으로 발생된 신경초종을 문헌고찰과 함께 보고하고자 한다.
•
논문접수일:1998년 12월 3일•
심사완료일:1998년 11월 4일•
책임저자:김 정 태330-715 충남 천안시 안서동 산16-5 단국대학교 의과대학 신경외과학교실
전화:041) 550-6369, 전송:041) 552-6870 E-mail:[email protected]
References
1) Bijlsma EK, Brouwer MR, Bosch DA, et al:Molecular
characterization of chromosome 22 deletion in schwannomas.
Genes Chromosomes Cancer 5
:201-205, 1992
2) Cho TH, Park YK, Chung YK, et al:Intramedullary neurile-
mmoma in conus medullaris. J Korean Neurosurg 19
:725- 729, 1990
3) Daras M, Koppel BS, Heise CW, et al:Multiple spinal in-
tradural schwannomas in the absence of von Recklinghau- sen’s disease. Spine 18
:2556-2559, 1993
4) Evans DG, Mason S, Huson SM, et al:Spinal and cutaneous
schwannomatosis is a variant form of type 2 neurofibroma- tosis
:A clinical and molecular study. J Neurol Neurosurg Psychiatry 62
:361-366, 1997
5) Honda M, Arai E, Sawada S, et al:Neurofibromatosis 2 and
neurilemmomatosis gene are identical. J Invest Dermatol 104
:74-77, 1995
6) Ishida T, Kuroda M, Motoi T, et al:Phenotypic diversity of
neurofibromatosis 2
:association with plexiform schwannoma.
Histopathology 32
:264-270, 1998
7) Jacoby LB, Jones D, Davis K, et al:Molecular analysis of
the NF2 tumor suppressor gene in schwannomatosis. Am J Hum Genet 61
:1293-1302, 1997
8) Kehrer Sawatzki H, Udart M, Krone W, et al:Mutational
analysis and expression studies of the neurofibromatosis type 2
(NF2
)gene in a patient with a ring chromosome 22 and NF2.
Hum genet 100
:67-74, 1997
9) MacCollin M, Woodfin W, Kronn D, et al:Schwannoma-
tosis
:A clinical and pathologic study. Neurology 46
:1072- 1079, 1996
10) Park SW, Kim YS, Yoon DH, et al:Intramedullary neu-
rilemmoma of the spine. J Korean Neurosurg 22
:1141-1147, 1993
11) Pulst SM, Riccardi V, Mautner V:Spinal schwannomatosis
[letter
;Comment]. Neurology 48
:787-788, 1997
12) Reith JD, Goldblum JR:Multiple cutaneous plexiform sch-
wannomas. Report of a case and review of the literature with
particular reference to the association with type1 and 2 neu-
rofibromatosis and schwannomatosis. Arch Pathol Lab Med
120
:399-401, 1996
13) Reznik M:Cutaneous neuropathology:
Neurofibroma, sch- wannomas and other neural neoplasms with cutaneous and ex- tracutaneous expression. Clin-Neuropathol 10
:225-231, 1991
14) Seppala MT, Sainio MA, Haltia MJ, et al:Multiple schwan-