Thoracic surgery is generally performed in the lateral posi- tion with the non-dependent lung collapsed to improve surgi- cal exposure, and one-lung ventilation (OLV) is applied to the dependent lung [1]. During OLV, more of the pulmonary blood flow is distributed to the dependent ventilated lung, improving
the match of ventilation with perfusion and oxygenation [2].
Conversely, if OLV is applied to the non-dependent lung, even though it is clinically rare, the increased perfusion to the depen- dent non-ventilated lung might cause severe hypoxemia. There- fore, the strategy to reduce shunt flow is required for treatment of the hypoxemia. We report a case of severe hypoxemia during carinal resection in the lateral position under non-dependent OLV and its management by ligating the pulmonary artery of the dependent lung.
Case Report
A 39-year-old female (height 155 cm, weight 44.5 kg) with mild dyspnea was scheduled for carinal resection and recon- struction because of an adenoid cystic carcinoma in the carina.
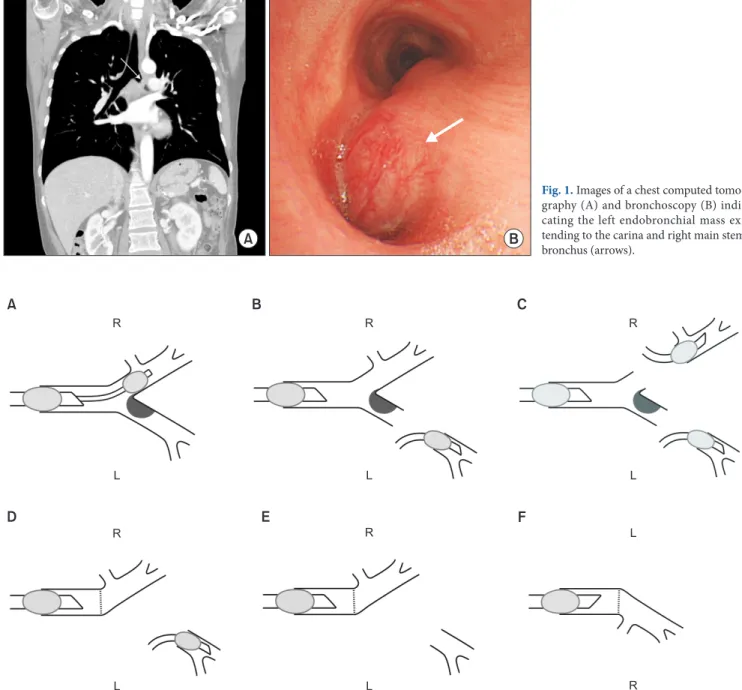
The chest computed tomography and bronchoscopy showed that
Case Report
During one-lung ventilation (OLV) in the lateral position, the dependent, ventilated lung receives more blood flow than the non-dependent, non-ventilated lung owing to gravity, improving the match of ventilation and perfusion. Conversely, in the rare clinical situations when OLV is applied to the non-dependent lung, arterial oxygenation can get worse due to considerable shunt flow to the dependent non-ventilated lung. We report a case of severe hypoxemia during carinal re- section under OLV of a non-dependent lung. In this case, OLV had to be applied to the non-dependent lung in the lateral position because the bronchus of the non-dependent lung was anastomosed with the trachea, whereas the bronchus of the dependent lung had already been resected for carinal resection. The subsequent hypoxemia resulting from the shunt flow to the dependent non-ventilated lung was treated successfully by ligating the pulmonary artery of the dependent lung.
Key Words: One lung ventilation, Perfusion, Thoracic surgery.
Severe hypoxemia during carinal resection in the lateral position under one-lung ventilation of a non-dependent lung
-a case report-
Chang-Hoon Koo 1 , Yoo Sun Jung 1 , Yong-Hun Lee 2 , Hyun-Chang Kim 3 , Jae-Hyon Bahk 1 , and Jeong-Hwa Seo 1
Department of Anesthesiology and Pain Medicine,
1Seoul National University Hospital,
2Asan Medical Center, Seoul,
3Keimyung University Dongsan Medical Center, Daegu, Korea
CC
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/
licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright ⓒ the Korean Society of Anesthesiologists, 2016 Online access in http://ekja.org
pISSN 2005-6419
•eISSN 2005-7563
Korean Journal of Anesthesiology
KJA
Corresponding author: Jeong-Hwa Seo, M.D., Ph.D.
Department of Anesthesiology and Pain Medicine, Seoul National University Hospital, 101, Daehak-ro, Jongno-gu, Seoul 03080, Korea Tel: 82-2-2072-2467, Fax: 82-2-747-5639
E-mail: [email protected] Received: March 19, 2015.
Revised: April 7, 2015.
Accepted: April 14, 2015.
Korean J Anesthesiol 2016 June 69(3): 279-282
http://dx.doi.org/10.4097/kjae.2016.69.3.279
280 Online access in http://ekja.org
VOL. 69, NO. 3, JuNe 2016 Non-dependent one-lung ventilation
the mass almost totally obstructed the left mainstem bronchus (LMB) and extended to the carina and right mainstem bronchus (RMB) (Fig. 1). Measuring on the chest computed tomography, the internal diameter (ID) and length of the RMB were 11 and 12 mm, respectively; the length of the distal LMB not involved by the mass was about 20 mm. She had no underlying diseases and her preoperative examinations were normal findings except
moderate obstructive pattern of the pulmonary function test: A forced expiratory volume in one second of 1.88 liter (73% of pre- dicted value), forced vital capacity of 2.81 liter (86% of predicted value) and their ratio of 67%.
General anesthesia was induced using target-controlled infusion of propofol (4 μg/ml) and remifentanil (4 ng/ml); ro- curonium 40 mg was administered for neuromuscular blockade.
A B
Fig. 1. Images of a chest computed tomo- graphy (A) and bronchoscopy (B) indi- cating the left endobronchial mass ex- tending to the carina and right main stem bronchus (arrows).
R
L
A B C
D E F
R R
L L
R R
L R L
L