Abstract : Accurate assessment of kidney function is necessary for patients with malignancies who are given renally clearing chemotherapy or nephrotoxic drugs. Creatinine clearance (CrCl) as a parameter to evaluate the glomerular filtration rate (GFR) of the kidney can be measured using a 24 hour urine collection (24hr-CrCl) or estimated by several predictive formulas using serum creatinine (Scr). Since these all have their limitations, this study was performed to find a more accurate formula for estimating renal function in malignancy.
Patients with a malignancy who had their 24hr-CrCl done at Samsung Medical Center from January 2008 to May 2012 were reviewed retrospectively.
Four hundred and fifty one patients were evaluated: males were 268 and female 183, the median age was 52 years (range 20-82), and Scr was 1.0 mg/dL (range 0.26-7.51) and mean 24hr-CrCl 103.6 mL/min. The estimation of all formulas was not different from the 24hr-CrCl, with the
악성종양 환자에서의 사구체 여과율 평가법 비교
삼성서울병원 약제부
Evaluation of a Predictive Formula for Glomerular Filtration Rate in Malignancy
Ji Yeun Woo , Hyun Jeung Im, Yong Won In, Young Mee Lee
Department of Pharmacy, Samsung Medical Center, 50 Irwon-dong, Gangnam-gu, Seoul, 135-710, Korea
회원학술보고
투고일자 2013. 8. 15; 심사완료일자 2013. 8. 29; 게재확정일자 2013. 10. 1
�교신저자 우지연 Tel:010-9079-5971 E-mail:[email protected]
exception of the Wright formula (p<0.001). The absolute Modification of Diet in Renal Disease (MDRD) was less biased and more precise than the MDRD however, the proximate estimation of both formulas was limited to patients with a 24hr-CrCl of <50 mL/min (p=0.21, p=0.33). The Cockcroft-Gault (CG) estimation was the most accurate, and it was not different from the 24hr- CrCl over a broad range of renal function (bias 1.91, 2.45, -0.48% in 24hr-CrCl<50, 50-100, >100 mL/min).
It is difficult to estimate the individual GFR over a broad range accurately with only one formu- la, however, these observations suggest that the CG provides a relatively good estimate of the 24hr-CrCl in general. Additionally, the use of the absolute MDRD can be considered in patients whose renal function has decreased, however, the Wright formula which significantly overesti- mated the 24hr-CrCl by 13.80%, showed limited applicability.
[Key words] Glomerular filtration rate, Malignancy, Cockcroft-Gault formula, Modification of Diet in Renal Disease (MDRD) formula, Wright formula
항암제를 투여 받는 악성종양환자에서 정확한 신기 능의 평가는 항암제의 독성을 최소화하고 치료 효과를 극대화시키기 위하여 필수적이다. 즉, 신장으로 배설 되는 항암제의 용량 설정 시 환자의 신기능을 과대평 가할 경우 항암제의 과용량 투여로 인한 부작용 발생 위험이 있고, 반대로 과소평가할 경우 투여량 부족으 로 인한 미흡한 항암효과가 우려된다. 사구체 여과율 (Glomerular filtration rate, GFR)은 신장의 배설 기능을 나타내는 지표로서 사구체에서 여과된 뒤 재흡 수 되지 않는 inulin이나 121I-iothalamate, 51Cr- EDTA 또는 Tc99m-DTPA와 같은 방사성 동위원소 를 이용하여 측정할 수 있다.
1),2)그러나 해당 marker 를 정맥 주사해야 하며 정확한 요수집을 위한 도뇨관 삽입이 필요할 수 있다는 번거로움이 있어 연구목적 외로는 사용되지 않는다.
1),2)일반적으로 임상에서는 GFR을 예측하는 방법으로 근육의 대사산물인 크레아 티닌의 청소율 (Creatinine Clearance, CrCl)을 사용
한다.
1),2)크레아티닌(Creatinine, Cr)은 대부분 사구체
여과로 배설되고, 검출이 편리하여 신배설 기능 평가 의 표준 물질로 사용되어 왔다.
1),2)그러나 Cr은 일부 세뇨관에서 분비되기 때문에 CrCl는 GFR보다 약 10% 정도 높게 측정될 수 있으며, 신기능이 감소함에 따라 사구체 여과가 감소하더라도 Cr의 세뇨관 분비 율은 증가할 수 있다.
2)-4)또한 근육량, 성별, 나이, 인 종, 병용약물, 실험실 분석법, 또는 단백 식이 등에 영 향을 받을 수 있는 점이 제한점이라고 할 수 있다.
CrCl을 구하는 한 방법은 24시간 요를 수집하여 혈청
으로부터 요로 배설된 Cr의 양을 직접 측정하는 방법
(24hr-CrCl)이다.
1),2)하지만 요수집 과정이 번거롭고
완벽한 요 수집이 어렵기 때문에, 혈청 Cr 농도에 기
초하여 CrCl를 예측하는 여러 가지 식(예, Cockcroft-
Gault (CG)식, Modification of Diet in Renal
Disease (MDRD)식, Wright식, Jelliffe식, Salazar-
Corcoran식, 그리고 Martin식 등)이 개발되어 사용
되고 있다.
CrCl 예측에 가장 많이 사용되는 CG식
5)은 오랜 임 상 사용경험을 바탕으로 신배설 약물의 용량 조절 기 준으로 쓰이고 있으나, 한 가지 식으로 다양한 환자의 신기능을 정확히 예측하는데 한계가 있다는 지적이 있 다. 실제로 신기능이 저하된 환자에서는 예측값이 과 대평가되고 신기능이 좋은 경우에는 과소평가되는 경 향이 있음이 보고된 바 있다.
6)-8)MDRD식
9),10)은 만성 신부전 환자에서 유도된 것으로, 신기능이 저하된 환 자에서는 CG식에 비해 신기능 평가면에서 더 우수하
고,
6),11)-13)신기능이 정상인 비 암질환 환자에서도 유사
하거나 우수한 결과를 보인 연구가 다수 보고되었
다.
7),14)이러한 연구를 바탕으로 미국 식품의약품안전
청(US Food and Drug Administration, FDA)에서 는 CG식과 함께 MDRD식을 신기능이 저하된 환자에 서의 약물용량 조절 기준으로 사용할 것을 추천하고 있다.
15)하지만 악성종양 환자에서의 임상적 유용성에 대해서는 추가적인 평가가 필요하다.
16),17)악액질(Cachexia) 또는 영양부족으로 인해 체중당 근육이 차지하는 비중이 적은 악성종양 환자는 근육의 대사산물인 혈청 Cr과 체중을 변수로 예측된 CrCl결 과를 그대로 신뢰하기 어렵다.
18)Wright 등
19)은 이런 환자군의 특성을 반영하고자 2001년에 암환자를 대상 으로 CrCl 예측식을 유도했으며, 임상적 유용성에 대 해서는 평가가 필요하다.
20)-23)본 연구는 악성종양 환자에게 가장 적합한 신기능 평 가 방법을 모색하여 최적의 항암 치료효과를 기대할 수 있도록 24시간 요수집을 통해 측정한 CrCl를 기준 으로 CG식, MDRD식, absolute MDRD식, Wright 식에 의한 예측값을 각각 비교하고 상관관계를 평가하 였다.
연구방법
1. 연구대상 및 제외기준
2008년 1월부터 2012년 5월까지 삼성서울병원 혈 액종양내과에 입원하여 24시간 요수집을 통해 CrCl 을 검사 (24hr-CrCl)한 631명의 악성종양환자를 대 상으로 하였다. 이중 혈액투석을 병행한 환자 11명을
제외하였고, 부적절한 요수집의 기준은 뇨에서 측정 된 체중 당 24시간 Cr 량이 각 연령군 별 평균에서 1 표준편차 이상 차이가 나는 것으로 정의하여
24)169명 을 제외하고 총 451명에 대하여 연구를 시행했다.
2. CrCl 측정값 및 예측값 계산
(1) 환자 정보
대상 환자 451명의 전자의무기록(Electronic medical record, EMR)을 후향적으로 검토하여, 24 시간 요수집 시행일의 검사결과, 나이 및 신체 계측 치를 수집하였다.
(2) 24시간 요수집을 통한 크레아티닌 청소율 (24hr-CrCl) 측정
24hr-CrCl은 다음의 식으로 계산하였으며, 혈청 및 뇨의 Cr 농도는 alkaline picrate-kinetic assay (Jaffe) 법으로 측정되었다. 본원 혈청 Cr 농 도 참고치의 상한값은 남자 1.3 mg/dL, 여자 1.1 mg/dL이며, 뇨 Cr 농도 참고치의 상한값은 남자 259 mg/dL, 여자 217 mg/dL이다.
Ucr : Urine concentration of creatinine Scr : Serum concentration of creatinine V : Urine volume
T : Duration of urine collection (1440 min)
(3) CrCl 예측값 계산
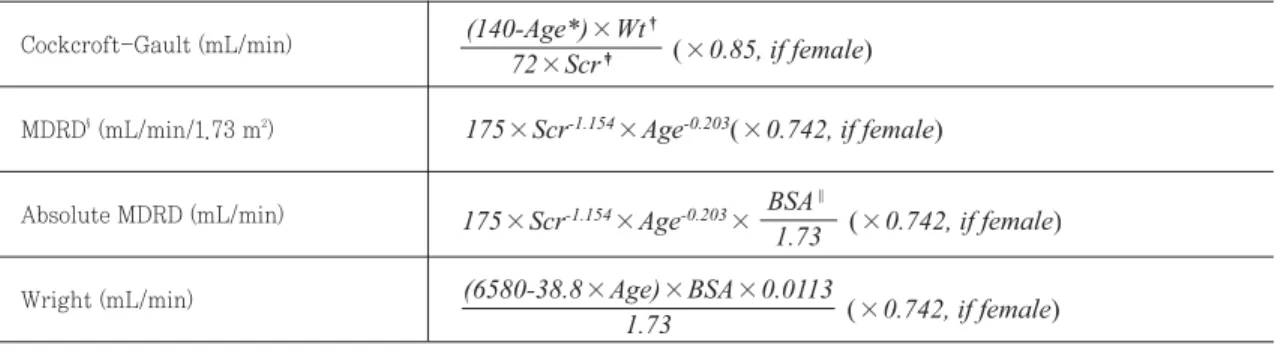
환자의 연령, 성별, 키 및 실체중을 이용하여 Table 1의 CrCl 예측식으로 계산하였고, 체표면적(Body surface area, BSA)는 DuBois and DuBois 식
25)으 로 구했다.
3. 통계 분석
24시간 요수집을 통해 측정한 24hr-CrCl과 4가지
식으로 예측한 CrCl의 상관관계를 분석하였다. 측정 값과 각 예측값의 통계학적 차이는 Shapiro-Wilks test로 정규성을 검정하여 두 변수간 차이가 정규성 분포를 따를 경우 paired t-test, 정규성 분포를 따 르지 않을 경우 Wilcoxon's signed rank test로 비 교하였다. 통계학적인 유의성은 p 값이 0.05 미만일 경우로 간주하였다. 24hr-CrCl에 대한 각 식으로부 터 계산된 예측값의 bias는 mean percentage error (MPE)로 평가하였고, 그 값이 0에 가까울수록 bias가 적은 것으로 해석할 수 있다. Precision은 mean absolute percentage error (MAPE)로 평가 하였고, 그 값이 작을수록 절대 백분율 오차가 적어 24hr-CrCl에 가깝게 예측한 것으로 해석할 수 있 다. 각 계산식은 다음과 같다.
또한 신기능 구간별 (24hr-CrCl<50 mL/min, 24hr-CrCl 50-100 mL/min, 24hr-CrCl>100 mL/min)로 상관관계를 분석하여 각 CrCl 예측식에 대한 이해를 돕고자 했다. 24hr-CrCl과 각 예측값 의 일치도는 concordance correlation coefficient (r
c)로 나타냈다.
연구결과
1. 연구대상의 특성
대상환자 451명(남성 268명, 여성 183명)의 나이 중간값은 52세(20-82), 체중은 62.3 kg (41.3-109.2), 그리고 혈청 Cr 농도는 1.0 mg/dL (0.26-7.51) 이 었다. 진단명으로는 림프종(30.8%), 다발성 골수종 (30.6%), 백혈병(25.9%)이 대부분을 차지하였고, 24 시간 요수집을 통해 측정한 환자의 평균 CrCl은 103.6 ± 46.2 mL/min이었다(Table 2).
2. 상관관계 분석
(1) 전체 대상환자의 CrCl 상관관계 분석 (n=451) 24hr-CrCl과 각 식에 의한 예측값을 Paired Student's t-test로 비교한 결과, CG에 의한 예측값 은 24hr-CrCl와 차이가 없었고(p=0.35) MDRD, absolute MDRD, Wright식에 비해 일치도가 가장 좋았다.(r
c=0.92) 반면에 Wright식에 의한 CrCl 예 측값은 13.8%의 bias로 차이가 있었다(p<0.001) (Fig. 1, Table 3).
(2) 신기능 구간별 상관관계 분석
환자의 신기능에 따라 세 그룹(24hr-CrCl<50 mL/min, 24hr-CrCl 50-100 mL/min, 24hr-
Cockcroft-Gault (mL/min)
MDRD§(mL/min/1.73 m2)
Absolute MDRD (mL/min)
Table 1. Formulas for the estimation of creatinine clearance
*Age : age in years
�Wt : weight in kilograms
�Scr : serum creatinine in mg/dL
§MDRD : modification of diet in renal disease
‖BSA : body surface area in m2 Wright (mL/min)
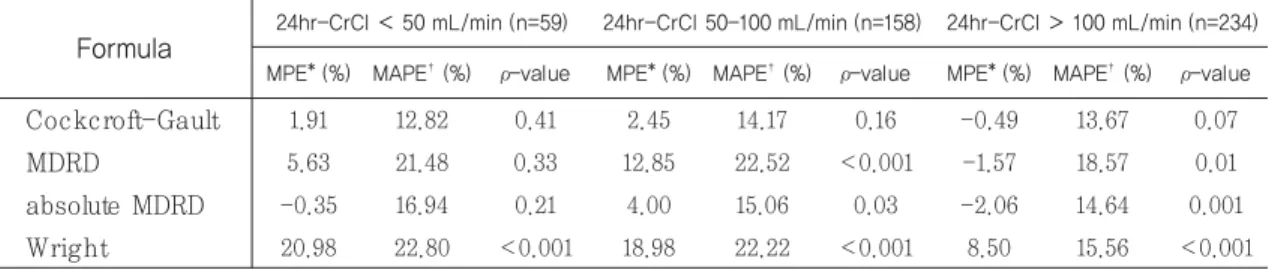
CrCl>100 mL/min)으로 나누어 분석한 결과 (Table 4), CG에 의한 예측값은 모든 그룹에서 24hr-CrCl과 차이가 없었고(p=0.41, 0.16, 0.07),
precision면에서도 MAPE가 각각 12.82%, 14.17%, 13.67%로 본 연구에서 비교한 예측식 가운데 가장 우수하였다. 반대로 Wright식에 의한 예측값은 모든
Age (year), median (range)Variables
52 (20-82) Gender, n (%)
Male 268 (59.4%)
Female 183 (40.6%)
Weight (kg), median (range) 62.3 (41.3-109.2)
Body surface area (m2), median (range) 1.68 (1.31-2.24)
Serum creatinine level (mg/dL) 1.00 (0.26-7.51)
Primary malignancy, n (%)
Lymphoma 139 (30.8%)
Multiple myeloma 138 (30.6%)
Leukemia 117 (25.9%)
Carcinoma 42 (9.3%)
Sarcoma 3 (0.7%)
Other hematologic disease 12 (2.7%)
CrCl, mean±SD*
24hr-CrCl (mL/min) 103.6 ± 46.2
CG (mL/min) 103.5 ± 47.0
MDRD (mL/min/1.73 m2) 105.1 ± 46.8
Absolute MDRD (mL/min) 102.4 ± 46.2
Wright (mL/min) 114.7 ± 48.7
Variables Table 2. Characteristics of study population (n=451)
*SD : Standard deviation
Cockcroft-Gault MDRD
Formula
0.92
r
c*
0.85
MPE
�(%)
13.73
MAPE
�(%)
0.35
0.82 4.42 20.34 0.37
Absolute MDRD
0.90 -0.14 15.09 0.06Wright
0.88 13.80 18.84 <0.001ρ -value Table 3. Correlation and comparison of the predicting formulas to the measured 24hr-CrCl
*rc: : Concordance correlation coefficient
�MPE : Mean pearcentage error
�MAPE : Mean absolute percentage error
그룹에서 24hr-CrCl과 차이를 보였고(p<0.001,
<0.001, <0.001), 다른 식에 비해 가장 큰 편차의 bias (20.98%, 18.98%, 8.5%)로 신기능을 과대평가 하는 것으로 나타났다. MDRD 및 absolute MDRD
에 의한 예측값은 신기능이 저하된 그룹(24hr-CrCl
<50 mL/min)에서만 24hr-CrCl와 차이를 보이지 않았고(p=0.33, p=0.21), MDRD보다 환자의 BSA 를 반영한 absolute MDRD에 의한 예측편차가 더 Formula
Cockcroft-Gault
24hr-CrCl < 50 mL/min (n=59) MPE* (%) MAPE�(%) ρ-value
1.91 12.82 0.41 2.45 14.17 0.16 -0.49 13.67 0.07
MDRD
5.63 21.48 0.33 12.85 22.52 <0.001 -1.57 18.57 0.01absolute MDRD
-0.35 16.94 0.21 4.00 15.06 0.03 -2.06 14.64 0.001Wright
20.98 22.80 <0.001 18.98 22.22 <0.001 8.50 15.56 <0.00124hr-CrCl 50-100 mL/min (n=158) MPE* (%) MAPE�(%) ρ-value
24hr-CrCl > 100 mL/min (n=234) MPE* (%) MAPE�(%) ρ-value
Table 4. Percentage prediction errors of the formulas in classified patients based on renal function
*MPE : Mean pearcentage error
�MAPE : Mean absolute percentage error
Fig. 1 Correlation between measured and estimated CrCl
(A) Cockcroft-Gault formula (B) MDRD formula
(C) Absolute MDRD formula (D) Wright formula
적었다.(bias 5.63%, -0.35%) 고찰
Carboplatin, cytarabine, etoposide, methotrex- ate 등과 같이 주로 신장으로 배설되는 항암제를 신 기능이 저하된 환자에게 투여할 때는 정확한 신기능 평가를 통해 적절한 항암제 용량을 설정하는 것이 필 수적이다. 임상에서 24시간 요를 수집하여 CrCl을 측정하는 방법은 번거롭고 완벽한 요수집도 어려워 사용이 제한적이므로, 실제 사구체 여과율 즉 신장의 배설기능 평가는 일반적으로 혈청 Cr 농도를 이용하 여 신기능을 예측하는 식을 이용하게 된다.
전체 대상환자의 24hr-CrCl 측정값을 가장 근접 하게 예측한 식은 CG와 absolute MDRD었다. CG 식은 24hr-CrCl<50, 50-100, >100 mL/min의
신기능 구간별 비교에서도 각각 1.91%, 2.45%, - 0.49%의 bias로 유사하게 24hr-CrCl을 예측했다.
단, 신기능이 저하된 군에서는 24hr-CrCl을 1.91%
높게 예측했고, 신기능이 좋은 군에서는 0.49% 낮게 예측하여 이전에 발표된 연구
6)-8)와 유사한 결과를 보 였으나 신기능 구간별 예측값의 편차가 크게 관찰되 지는 않았다. Absolute MDRD식은 환자의 BSA를 1.73 m
2로 표준화한 MDRD식에 다시 환자의 BSA 를 반영한 값을 구하고자 한 것으로 CG, Wright식 과 같이 mL/min으로 CrCl을 나타낸다. Absolute MDRD식은 MDRD식에 비해 적은 bias (각 - 0.14%, 4.42%)와 향상된 precision (15.09%, 20.34%)을 보였다(Fig. 2). 이는 MDRD식이 환자 의 BSA를 1.73 m
2로 표준화하여 예측한 GFR 값을 나타내기 때문에 환자의 체격이 작거나 큰 환자에서 의 오차가 환자의 BSA를 반영함으로써 예측도가 향 Fig. 2 Percentage difference between measured and estimated CrCl
(A) Cockcroft-Gault formula (B) MDRD formula
(C) Absolute MDRD formula (D) Wright formula
상되었을 것으로 추측된다. 신기능 구간별 비교에서 MDRD와 absolute MDRD식으로 구한 예측값은 신 기능이 저하된 군(24hr-CrCl<50 mL/min)에서는 24hr-CrCl와 차이를 보이지 않았지만, 그 외 군에 서는 차이가 있어 신기능이 저하된 환자에서의 예측 도가 더 정확함을 확인했다. 이는 MDRD식이 유도 된 환자군이 평균 GFR 40 mL/min/1.73 m
2미만 의 만성신부전 환자였음을 고려할 때 예상된 결과이 며, 이러한 경향은 여러 국외 논문에서도 발표된 바 있다.
6),8),11)-13),26),27)Wright 등
19)은 기존의 신기능 예측식이 대부분 환 자의 체격, 혈청 Cr을 변수로 하기 때문에 체중당 근 육량이 적을 수 있는 암환자의 특성을 반영하고자 102명의 고형 악성종양 환자를 대상으로 신기능 예 측식을 유도했다. 본 연구에서는 90%가 혈액종양 환 자였던 점이 다르긴 하나 Wright식에 의한 예측값 이 13.8%의 가장 큰 bias로 24hr-CrCl와 차이를 보였고, 신기능 구간별 분석에서도 각각 20.98, 18.98, 8.5%의 bias로 모두 24hr-CrCl을 과대평가 하였다. 이는, 예를들어 Calvert formula
3)에 의해 CrCl 30 mL/min인 환자의 carboplatin의 용량설 정시(Area under the curve, AUC=5.5) 최대 약 33 mg (11%)의 용량차이를 나타낼 수 있는 범위로 임상에 적용하는데 한계가 있을 것으로 판단된다.
Wright식에 대한 평가는 악성종양 환자를 대상으로 한 여러 국외논문에서 서로 상반된 결과가 보고
20)-23),28),29)