DOI 10.17480/psk.2020.64.2.156
Comparative Study of Carboplatin Dosing in Lung Cancer Patients Using the Calvert Formula and Four Equations for
Estimating Glomerular Filtration Rate
Seo Won Kim*
,†, Young-Mo Yang**
,†, and Eun Joo Choi***
,#*Department of Pharmacy, Chonnam National University Hospital, Gwangju, Republic of Korea
**Department of Biomedical Informatics, Ajou University School of Medicine, Suwon, Republic of Korea
***Department of Pharmacy, College of Pharmacy, Chosun University, Gwangju, Republic of Korea
(Received February 13, 2020; Revised April 9, 2020; Accepted April 10, 2020)
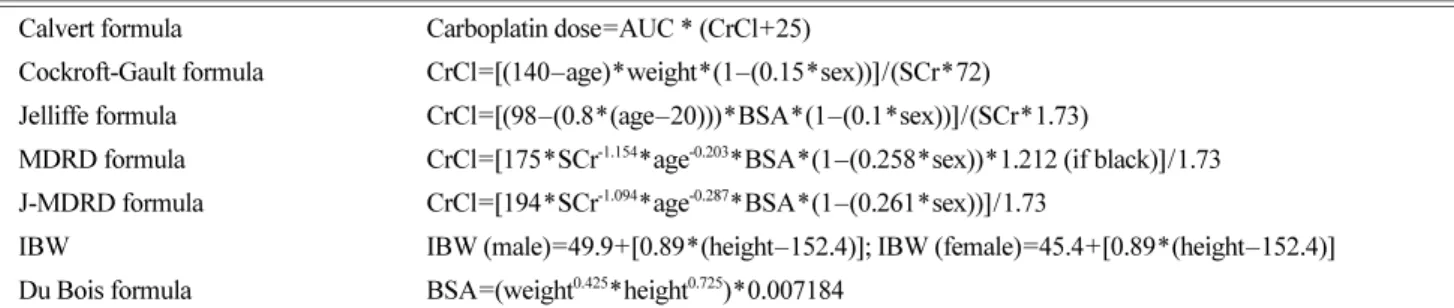
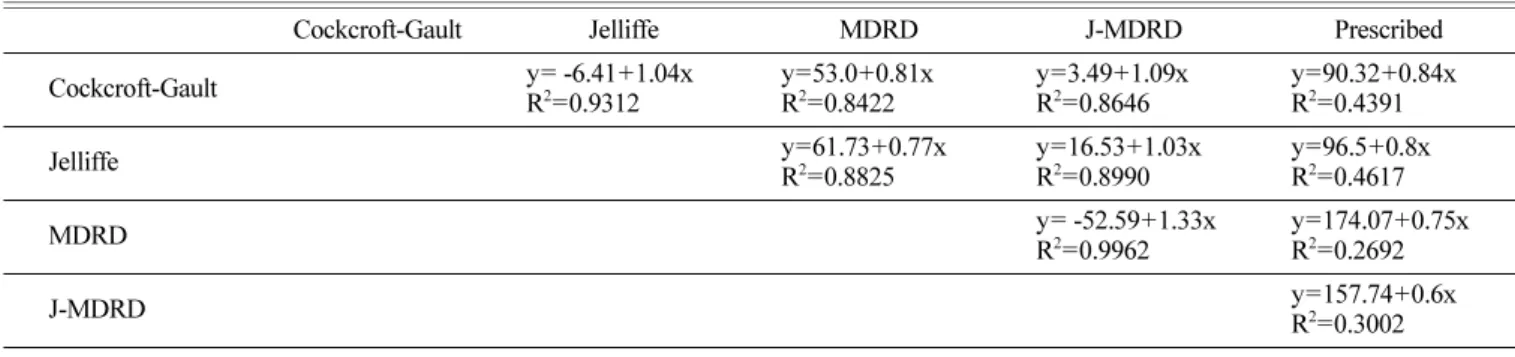
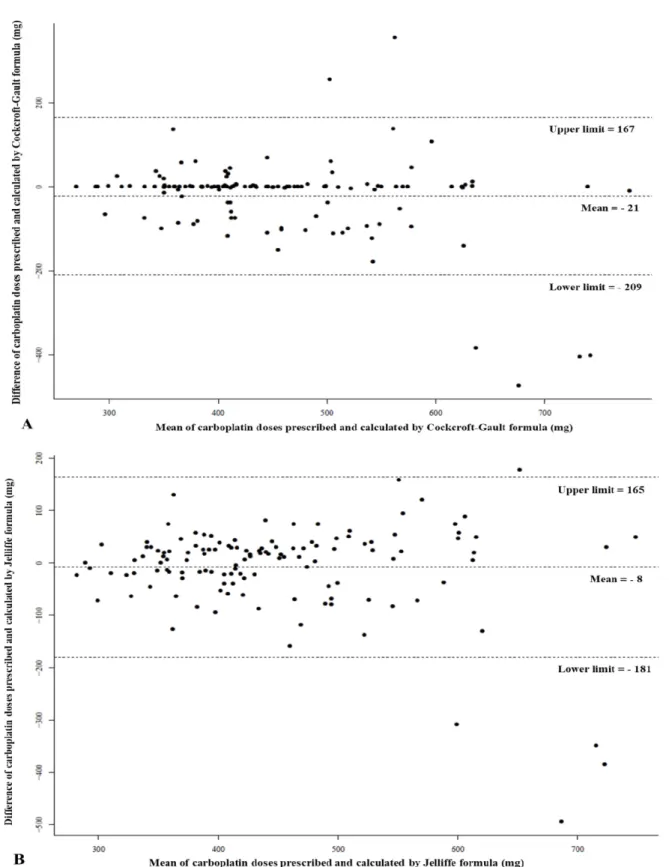
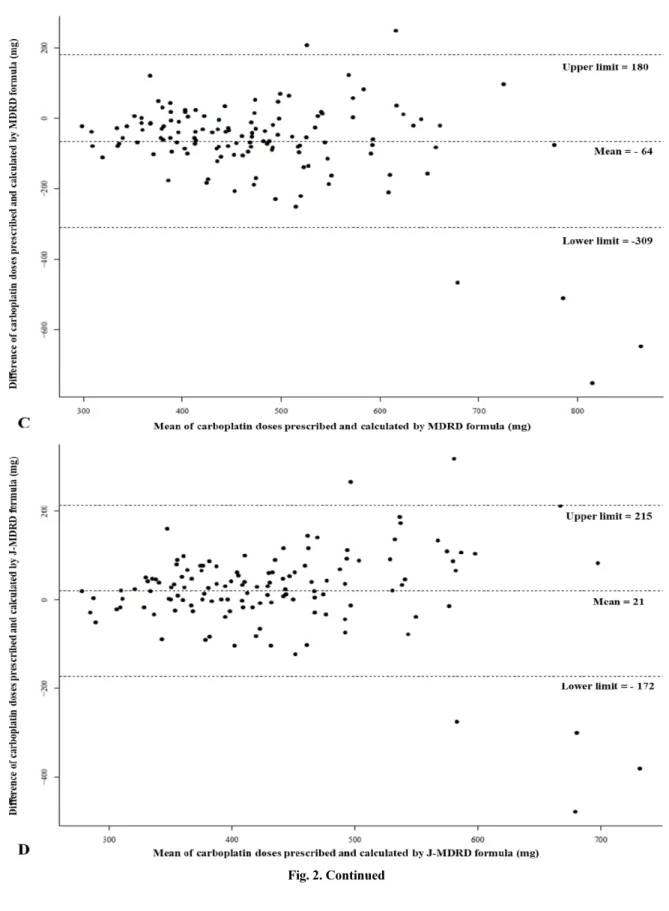
Abstract Several studies have been conducted to estimate more accurate and precise glomerular filtration rate (GFR) in cancer patients; however, studies on determining carboplatin doses by the renal functions of Korean cancer patients have been rarely implemented. The aim of this study was to compare carboplatin doses calculated by the Calvert formula based on estimated GFRs with various equations with its dose prescribed by the physicians. This study was retrospectively conducted in patients (≥18 years) with lung cancer who had received carboplatin between September 2011 and August 2013. Data were collected by reviewing the electronic medical records (EMRs). Among 129 patients with lung cancer, 95 were males. Mean age was 65.0 years, and mean estimated GFRs of Cockcroft-Gault, Jelliffe, Modification of Diet in Renal Disease (MDRD), and MDRD for Japanese (J-MDRD) formulae were 65.7, 63.2, 74.1, and 57.5 mL/min, respectively. Compared with mean prescribed carboplatin dose (444.4 mg), its mean estimated doses by Cockcroft-Gault, Jelliffe, MDRD, and J-MDRD formulae were 465.8, 452.5, 508.6, and 423.3 mg, respectively. The carboplatin doses estimated by Cockcroft-Gault and Jelliffe formulae showed relatively smaller bias and better precision than those estimated by MDRD and J-MDRD formulae. The carboplatin dose calculated based on estimated GFR with MDRD formula showed the biggest bias and lowest precision. When the characteristics of patients in this study were considered, the J-MDRD formula may estimate more accurate GFRs than other formulae originated from Western patients. Further related studies are needed for Korean cancer patients.
Keywords Carboplatin dosing, Calvert formula, lung cancer, glomerular filtration rate estimation
Introduction
Carboplatin derived from cisplatin is the second generation of a platinum-containing anticancer drug which was approved by the Food and Drug Administration (FDA) for the treatment of ovarian cancer, and is used to treat reproductive cancers (e.g. cervical cancer and endometrial cancer), as well as solid cancers (e.g. lung cancer, head and neck cancer, and bladder cancer).
1,2)The frequency of platinum-containing anticancer drug use has been low in the treatment of non-small-cell lung cancer (NSCLC), but the survival rate of NSCLC patients was increased after
carboplatin use.
3)In employing a combination of carboplatin and docetaxel for the treatment of NSCLC, overall response rate and median overall survival time were 30.2% and 340 days, respectively.
4)Since carboplatin has relatively a lower incidence rate of adverse reactions (ARs) (e.g. nausea, vomiting, nephrotoxicity, and neurotoxicity) than cisplatin, carboplatin is used as a substitute for cisplatin.
5)In one study of NSCLC treatment, carboplatin was less effective than cisplatin, but displayed a lower incidence rate of serious ARs.
3)In the treatment of small-cell lung cancer (SCLC), carboplatin caused more hematologic ARs (e.g.
anaemia, thrombocytopenia, leukopenia, and neutropenia) than cisplatin, but its use led to fewer gastrointestinal ARs, nephrotoxicity, and ototoxicity.
6)In addition, when administered to elderly patients, carboplatin had a low incidence rate of non- hematologic ARs, such as nausea, vomiting, dizziness, and loss of appetite.
7)†
Seo Won Kim and Young-Mo Yang are co-first authors and contrib- uted equally to the writing of this article.
#