심방중격결손과
5
0
0
전체 글
(2) 외 혈청 전해질검사, 뇨검사, 일반생화학검사는 모두 정. 어 내원하였다. 과거력:내원 5개월전에 고혈압을 진단받고 항고혈 압제를 복용하였다. 당뇨병이나 고지혈증의 과거력은 없. 상이었다. 흉부 X-선 소견:심흉곽비(cardiothoracic ratio; CT ratio)가 0.74로 커진 심장음영과 폐부종, 양측 흉. 었으며, 50년갑의 흡연력이 있었다.. 막삼출소견이 보였다(Figs. 1 and 2).. 가족력:어머니가 고혈압이 있었다. 이학적 소견:비교적 건강해 보였고 혈압은 140/80 mmHg, 심박동은 분당 68회로 규칙적이었다. 심잡음이. 심전도 소견:분당 54회의 동성서맥과 우축편위의 소견을 보였다.. 주로 수축기시에 좌측상방흉골연에서 들리고 있었으며. 경흉부 심초음파:좌심방에서 우심방으로의 단락혈류. (GII/IV) 양측폐첨부를 제외한 전폐영역에서 거칠은 수. 가(Figs. 3 and 4) 보이는 이차공 심방중격결손이 있었. 포음이 들리고 있었다. Thrill은 촉지되지 않았고 heaving. 고, 우심실이 49 mm으로 확장되어 있었으며 최고 삼. 은 없었다. 사지에서 함요부종이 있었다.. 천판 역류속도(peak TR velocity)가 3.1 m/sec이었으. 검사실 소견:혈액검사상 혈색소 12.1 g/dL, 백혈구 3. 3. 며 좌심실 구출율은 60%정도였다.. 7000/mm 이었으며 혈소판 242,000/mm , CK 143 U/L. 심도자 소견:상대정맥, 하대정맥, 우심실, 우심방, 주. (정상치 55~170), CK-MB 15ng/ml(정상치 0~16). 폐동맥의 산소 포화도는 각각 67.8%, 75.2%, 86.4%,. 이었다. 혈청지질 검사상 Total cholesterol 79 mg/dL,. 84.2%, 85.3%로 혼합정맥혈과 우심실사이의 산소포화. HDL-cholesterol 23 mg/dL, LDL-cholesterol 40. 도 상승이 있었으며, 우심실과 폐동맥 사이에 유의한 산. mg/dL, Triglyceride 78 mg/dL으로 정상범위였다. 그. Fig. 3. Initial Doppler transthoracic echocardiogram revealed shunt flow from left atrium to right atrium. Fig. 1. Initial chest PA revealed severe cardiomegaly and pulmonary edema and bilateral pleural effusion.. Fig. 2. Postoperative chest PA revealed decreased cardiomegaly relative to initial chest PA.. 768. Fig. 4. Postoperative doppler transthoracic echocardiogram revealed disappearance of shunt flow from left atrium to right atrium.. Korean Circulation J 2000;30(6):767-771.
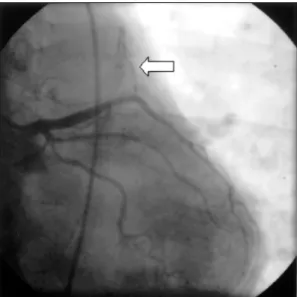
(3) Fig. 5A. Angiogram revealed coronary AV fistula (arrow) draining from left coronary artery to main pulmonary artery (LAO 8° Caudal 26°projection of left coronary artery).. Fig. 5B. LAO 3°Caudal 23°projection of left coronary artery.. Fig. 5C. LAO 49°Cranial 35°projection of left coronary artery.. Fig. 5D. RAO 43°Cranial 41°projection of left coronary artery.. 동맥과 분지 혈관은 정상이었다. 소포화도의 차이는 없었다. 주폐동맥의 수축기시 압력. 경과 및 치료:개흉 수술을 시행하였으며 이차공 심. 이 34 mmHg(정상치 15~30), 이완기시 압력이 29. 방중격결손이 2.0×2.5 cm 크기로 있었으며 자가 심막. mmHg(정상치 5~12)로 상승되어 있었고 또한 우심. 을 이용하여 이를 페쇄시켰다. 그리고 주폐동맥의 폐동. 실 유출로에서의 압력이 41.3 mmHg(정상치 15~30). 맥판 직상방 좌측벽 부위의 내막으로 연결되는 혈관을. 으로 증가되어 있었다. Qp/Qs ratio는 1.96이었다.. 발견하였으며 수술장에서 그 혈관의 기시부는 확인하. 관상동맥 조영술:좌전하행지의 중간부위에 주폐동맥. 지 못하였고 개폐동맥(pulmonary arteriotomy)을 실. 으로의 동정맥루가 관찰되었다(Fig. 5). 그 외 주요 관. 시하여 관동정맥루의 개구부를 막아주었다. 수술후 환 769.
(4) 자는 합병증 없이 증상의 호전이 있었으며, 현재 외래. 적으로 막힌 경우도 보고된 바 있으나18) 드물다. 치료. 에서 추적관찰 중이다.. 는 증상이 있는 경우에만 수술을 하는 것이 전통적이었 으나 나이가 들어감에 따라 때로는 치명적인 여러 합병. 고. 찰. 증에 의한 증상을 일으킬 수 있고 젊을 때 일찍 수술하 는 것이 나이가 들어 증상이 나타났을 때 수술하는 것. 발생학적으로 관동정루는 원시심근 동양혈관(primitive. 보다 수술 사망유과 합병증이 적으므로 모든 경우에 있. myocardial sinusoids)의 불완전한 폐쇄로 인해 성숙. 어서 진단후 가능한한 빠른 시간내에 수술로써 교정하. 된 관동맥과 심방실 또는 심혈관 사이의 연결지속으로. 는 것이 바람직하겠다.4)17). 8-10). 형성되게 된다.. 대부분의 경우 선천성이지만 심근 10). Koumai 등은 관동정맥루(관동맥-좌심실)와 정맥동. 선. 심방중격결손이 있는 환자에서 좌측 심부전이 있는 증. 천성 관동정맥루는 흔치 않은 기형으로 선택적인 관상. 례를 보고한 바 있고15) Hijazi 등은 관동정맥루(우관동. 동맥 조영술을 시행한 모든 환자들의 약 0.1~0.2%에. 맥-우심방)와 이차공 심방중격 결손이 결합된 증례를. 경색후에 이차적으로 발생한 것도 보고되고 있다.. 11)12). 서 관찰된다.. 선천성 관동정맥루는 약 20%에서 여 9). 러 다른 심질환을 동반한다고 한다.. 보고하였다.13). 그 중 승모판 역. 본 증례에서는 좌전하행지의 중간부위에서 기시하여. 류나 삼천판 폐쇄 등의 판막질환, 동맥관 개존증, 동맥. 주폐동맥으로 연결되는 관동정맥루와 이에 동반되는 이. 경화성 관상동맥 질환, 폐동맥 협착과 같은 대혈관의 기. 차공 심방중격결손을 수술로써 교정하였다. 본 환자는. 형, 확장성 또는 비후성 심근질환, 지속적 좌상대정맥. 관동정맥루와 심방중격결손의 두가지 기형이 모두 좌우. 13-15). 과 같은. 단락을 야기해서 심실에 용적 과부하를 유도하여 울혈. 선천성 심질환 등이 보고되어 왔다. 관상동맥과 심방실. 성 심부전에 의한 호흡곤란을 일으켰으며 이러한 증상. 혹은 대혈관사이의 비정상적인 교통은 대개 우심방이. 은 수술후에 호전되었다.. 이나 Follot 3징, 심방 또는 심실중격결손. 나 우심실, 폐동맥과 연결되어 있지만 드물게는 좌심방. 요. 이나 좌심실로 연결되어 체순환계 내에서의 교통을 형. 약. 성하게 된다.16) 임상적으로 관동정맥루는 약 반수의 경우에서는 아무. 저자들은 운동시 호흡곤란을 주소로 내원한 환자에서. 증상도 일으키지 않으나 나머지 반수에서는 울혈성 심. 심방중격결손과 동반된 관동정맥루 1예를 수술적으로 치. 부전, 심근허헐, 심내막염 등에 의한 증상을 일으키게. 료하여 증상의 호전을 경험하였기에 이를 문헌고찰과 함. 된다. 운동시 호흡곤란, 피로 협심증, 반복되는 호흡기. 께 보고하는 바이다.. 계 감염, 그리고 심내막염에 의한 증상이 가장 흔하고 이러한 증상들은 어릴 때보다는 대개 나이가 들어가면. 중심 단어:심방중격결손・동반된 선천성 관동정맥루.. 서 나타나게 된다.4) 선천성 관동정맥루의 진단에는 경. REFERENCES. 흉부 또는 경식도 심초음파와 자기공명영상(MRI)이 도. 1) Levine DC, Fellows KE, Abrams HL. Hemodynamically. 움을 줄 수 있으나 관상동맥 조영술이 가장 정확한 진. significant primary anomalies of the coronary arteries. Angiographic aspects. Circulation 1978;58:25-34. 2) Ha JW, Lee HJ, Lee JY, Kim HY, Yoon J, Choe KH. Bilateral coronary arteriovenous fistula coexistent with atrial septal defect and pulmonary stenosis. Yonsei Med J 1997 Jun;38:190-2. 3) Tai YT, Fong PC, Chow WH. Bilateral coronary-arteryto-pulmonary artery fistula coexistent with apical hypertrophic cardiomyopathy- a case report. Angiology 1992; 43:72-5. 4) Liberthson RR, Sagar K, Berkoben JP, et al. Congenital coronary arteriovenous fistula : Report of 13 patients, review of the literature and delineation of management. Circulation 1979;59:849-54.. 단방법이다. 특징적인 이학적 소견으로 거칠은 연속성 의 심잡음이 오른쪽 혹은 왼쪽의 두 번째에서 네 번째 의 늑간에서 들리며 이런 연속성 잡음을 일으킬 수 있 는 다른 심질환, 즉 동맥관 개존증이나 Valsalva의 대 동맥동파열, 흉벽의 동정맥루, 폐혈관 동정맥루나 대동 맥 폐동맥 중격결손, 또는 대동맥 역류를 동반한 심실 중격결손 등과 감별을 요한다.16) 관동정맥루의 예후는 단락양과 환자의 나이, 그리고 다른 합병증의 유무에 달려 있다.16) 관동정맥루가 자연 770. Korean Circulation J 2000;30(6):767-771.
(5) 5) Bilumental’ AL, Nekrutman EA, Pomerantsev EV, Liaki-. 6). 7). 8). 9) 10) 11) 12). shev AA. Association of coronary atherosclerosis, congenital coronary fistulas and Fallot’s triad in a middle-aged man. Kardiologiia 1990 Jun;30:108-10. Egami J, Sudo K, Ikeda K, Ide H, Kokubo J, Koishizawa T, et al. Surgical management of coronary artery fistula with tricuspid stenosis in a three-month-old infant. Kyobu Geka 1994 Sep;47:854-7. Branco L, Agapito A, Ramos JM, Patricio L, Monteiro I, Galrinho A, et al. Coronary fistula-clinical and angiographic review. Rev Port Cardiol 1994 Mar;13:243-52, 193-4. Fredarick LG, Calvin FA, Harold AB, Kurt A, Yang W. Shunts between the coronary artery and pulmonary arteries with normal origin of the coronary arteries. Am J Cardiol 1970;25:655-61. Na BW, Lim SW, Park JW, Cho YK, Kim TY, Cha DH. Bilateral congenital coronary arteriovenous filstulas. Korean Circulation J 1998;28:1630-2. Grant RT. Development of the cardiac coronary vessels in the rabbit. Heart 1926;13:261-71. Said SAM, Landman GHM. Coronary-pulmonary fistlar: Long-term follow-up in operated and non-operated patients. Int J cardiol 1990;27:203-10. Gilbert C, Van Hoof R, Van de Werf f, Piessens J, De. 13). 14) 15) 16). 17). 18). Geest H. Coronary artery fisulas on an adult population. Eur Heart F 1986;7:437-43. Hijazi A, Mazhar R, Hajar R. Coronary artery fistula and atrial septal defect: a case report and brief review of the literature. Ann Thorac Cardiovasc Surg 1998 Oct;4: 286-7. Suzuki T, Ishikawa S, Sekiguchi T, Ono M, Kakita N. Case of coronary arteriovenous fistula with atrial septal defect. Kyobu Geka 1971;24:665-70. Koumi S, Endo T, Hata N, Takayama M, Sugiki Y, Atarashi H, et al. Coronary artery-left ventricular fistulae with atrial septal defect. Cariology 1989;76:461-4. Gasul BM, Arcilla RA, Fell EH, et al. Congenital coronary arteriovenous fistula: Clinical, phonocardiographic, angio-cadiographic and hemodynamic studies in five patients. Pediatrics 1960;25:531-60. Kugelmass AD, Manning WJ, Piana RN, Weintraub RM, Baim DS, Grossman W. Coronary arteriovenous fistula presenting as congestive heart failure. Cathet Cardiovasc Diam 1992 May;26:19-25. Griffiths SP, Euis K, Hordof AJ, Martin E, Levine RO, Gersony WM. Spontaneous complete closure of a congenital coronary artery fistula. J Am Coll Cadio 1983 ;2 : 1169-73.. 771.
(6)
수치

관련 문서
Randomised, double blind, placebo controlled study of fluticasone propionate in patients with moderate to severe chronic obstructive pulmonary disease: the
Small bowel Dieulafoy lesions Vascular ectasias of colon Meckel's diverticulum-distal ileum Aortocolonic or arteriocolonic fistula Solitary colonic ulcers.
GRIPHON Prostacyclin (PGI2) Receptor Agonist In Pulmonary Arterial Hypertension IPAH idiopathic pulmonary arterial hypertension MCTD mixed connective tissue
Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in
Although van der Waals equation is still less accurate at high
Incident major cardiovascular events (coronary artery disease, ischemic stroke, hemorrhagic stroke and cardiovascular mortality) were set as primary end points.
If the resonant frequency w, and the output capa- citor CO are sufficiently greater than the output frequency w, and the resonant capacitor C , , respectively, then
Among the various pulmonary manifestations, interstitial lung disease (ILD) is known to be associated with substantial morbidity and mortality rates in RA patients.. As RA-ILD
