- 5 -
Rhinologic Headache
Seok-Hyun Cho, M.D. and Kyung-Rae Kim, M.D.
INTRODUCTION
Each year, 10% to 20% of the general population consult physicians with headaches of various etiolo- gies.1) In an assessment of the lifetime prevalence of headache disorders in a cross-sectional epidemiologic survey of 1000 men and women, 25 to 64 years old, Rasmussen and Olesen noted a 15% incidence of headaches associated with disorders of the nose and sinuses.2) Of 100 consecutive patients presenting to an otolaryngology clinic with symptoms of sinusitis, 48 (48%) complained of severe headaches.3)
Although headaches and facial pains are common symptoms in patients with inflammatory conditions within the nasal cavities or paranasal sinuses, they occasionally may be the major presenting symptom without associated symptoms suggestive of an infec- tion. In a patient initially seen primarily with headaches or facial pain, the following need to be ruled out as part of the differential diagnosis:migraines, ophth- almic disorders, temporomandibular joint disorders, vascular diseases, neurological causes, and cervical spine disorders. However, a rhinologic source should also be included in the differential diagnosis and ap- propriately evaluated.4)
HEADACHE :OVERVIEW AND CLASSIFICATION
Headache is a common symptom that is usually
handled, and handled well, by general practitioners. It is a test of the clinical art, as a working diagnosis can usually be established after taking the history.5) The physical examination is guided by the history and pain description. Routine examination for headache should include assessment of head, neck, and jaw range of movement, extraocular movement, pupillary reaction to light and accommodation, ocular fundus, mouth, tongue, dentition, and lymphatics, in addition to the usual ear, nose and throat structures. A straightforward and long history of migraine or tension-type headache does not require investigation. A CT scan should always be considered for patients with cluster headache, as the syndrome has been reported secondary to tumors ar- ound the cavernous sinus or craniospinal junction.6)
The pain generally associated with headaches is of intracranial origin.7) This pain appears to originate form one of three structures:tissue covering the cranium, cranial periosteum, and certain intracranial structures.
These structures include the trigeminal neve, the first three cervical nerves, cerebral arteries, dural arteries, parts of the dura at the base of the brain, and the great venous sinuses and their tributaries from the surface of the brain. Because of the gray matter and the dura are insensitive to pain but the pia and the dural vessels are sensitive, it is theorized that the vast majority of headaches are vascular in nature.
In 1988, the International Headache Society (IHS) developed criteria for headache and facial pain dis- orders (Table 1).8) These guidelines have proved inva- luable in organizing headache research, and they form the basis for the category of headache in the Inter- national Classification of Diseases.9)
Headache can be broadly categorized into primary headaches and secondary headaches due to an under- lying medical condition. The diagnosis of primary headache is a proactive process that necessitates a Department of Otorhinolaryngology, College of Medicine, Ha-
nyang University, Seoul, Korea
Address correspondences and reprint requests to Seok-Hyun Cho, M.D., Department of Otorhinolaryngology, Hanyang Uni- versity, 17 Haedang-Dong, Sungdong-Gu, Seoul 133-792, Korea Tel:82-2-2290-8580, Fax:82-2-2293-3335
E-mail:[email protected]
Accepted for publication on September 11, 2002
thorough history and physical examination, including focused neurologic examination. Several historical fac- tors can suggest primary headache, including 1) onset in adolescence or early adulthood, 2) stable pattern of similar headaches over a period of more than 6 months, 3) family history, 4) menstrual association, and 5) va- riable site of headache from attack to attack or within the same attack. In addition, several “red flags” can increase the index of suspicion for secondary headache disorders:1) headache that begins suddenly, 2) onset after age 40 years, 3) onset of new headache type, 4) new level of pain, 5) accelerating headache intensity or frequency (gradual or acute), 6) headache initiated with exertion or Valsalva maneuver, 7) headache asso- ciated with neurologic changes, 8) headache in patients with a history of human immunodeficiency virus or an underlying malignancy, and 9) history of headache that interrupts sleep.10)11)
Primary headache conditions include migraine and tension-type headache, the latter being the most com- mon headache experienced by the general population but not necessarily in patients seeking medical evalua- tion. Individuals are unlikely to seek medical attention for episodic tension-type headache or other mild non- disabling headache conditions. Usually, these types of headaches are effectively managed with lifestyle modifications or nonprescription analgesics. Patients with clinically relevant migraine often experience
several clinical presentations of headache, including migraine, migrainous headache, and tension-type he- adache. This entire spectrum of headache activity responds equally well to migraine-specific (eg, tri- ptans) medications, suggesting that these different clinical presentations of headaches in patients with migraine have a similar underlying biology.12) Patients with serious headache syndromes such as suspected subarachnoid haemorrhage or meningitis should be referred urgently to a neurological or neurosurgical center. Most common headache syndromes are best handled by a knowledgeable general practitioner.
RNINOLOGIC HEADACHE
The enormous amount of knowledge that has been accumulated during the last 3 decades on vascular and neurologic causes of headache has eclipsed the impor- tance of chronic sinonasal pathology as a significant cause of headache. Wespi and Stojan share the view that headache can be of nasal origin.13) They are of the opinion that chronic irritation of the mucosa or direct contact between the septum and the mucosa of the turbinates are the main causes of nasal headache. They pointed out that small ostia leading to the paranasal sinuses may easily be closed and bring about defective sinus ventilation, contributing to the patient’s complaints.
Pain in the frontonasal region (rhinologic headache) may be caused by acute or chronic sinusitis, septal spur, contact pressure of bullar ethmoidalis and middle turbinate, nasofrontal duct mucosal disease, agger nasi cell pneumatization, presence of Haller’s cell, primary and secondary mucocele of the ethmoid, or sphenoid sinus.14-17)
Patients complaining of headache can be divided into the following groups.3) 1) Patients whose he- adaches are clearly related to sinus problems such as inflammatory disease, neoplasm, barotrauma, or ano- ther identifiable pathology. 2) Patients with headaches clearly connected to non-sinus causes, including mig- raine, neuralgias, cervical spine disorders, low or high blood pressure or other vascular disorders, allergy, or temporomandibular joint or ophthalmic problems. 3) Those who cannot be classified because of uniden- tifiable etiological factors. It is this third group that presents a challenge to the otolaryngologist.
Indeed, it is not always possible to distinguish he-
Table 1. Categories of the international headache society cl- assification system
01. Migraine
02. Tension-type headache
03. Cluster headache and chronic paroxysmal hemicrania 04. Miscellaneous headache not associated with structural
lesions
05. Headache associated with head trauma 06. Headache associated with vascular disorders 07. Headache associated with nonvascular intracranial
disorders
08. Headache associated with substance use or withdrawal 09. Headache associated with noncephalic infection 10. Headache associated with metabolic disorders
11. Headache or facial pain associated with disorders of the cranium, neck, eyes, nose, sinuses, teeth, mouth, or other facial or cranial structure
12. Cranial neuralgias, nerve trunk pain, and deafferentation pain
13. Headache not classifiable
adaches caused by the sinonasal abnormalities from headaches caused by the multitude of other possible etiologic factors when attempting to define patients with sinusitis and headaches. Nasal and sinus-related pain can mimic primary headache syndromes, inclu- ding migraine, tension-type headache, and cluster, and coexistence of common conditions like migraine, tension-type headaches, and sinusitis remind us that finding one cause for headache does not exclude other simultaneous headache disorders.18)
When should the patient with headache be referred to the rhinologist (otolaryngologist)?19) An otolaryngo- logist consultation should be considered under the following two circumstances :1) If acute frontal or sphenoid sinusitis is suspected (both represent medical emergencies) 2) If the result of a complete headache workup is unremarkable. For example, the patient has been seen and evaluated by the neurologist, ophthal- mologist, internist, and dentist, with no abnormalities found. An imaging evaluation of the brain and cervical spine is normal. An electroencephalogram (EEG) is within normal limits. In the latter circumstance, an office nasal and sinus endoscopic examination with a rigid endoscope can be performed, and coronal CT scans of the sinus can be evaluated by the rhinologist to determined a possible etiology for the patient’s headache. But, there is no correlation between the severity or site of pain and the extent or location of the mucosal disease.20) The combination of theses studies can provide maximum information, allowing a nasal or sinus cause for the patient’s symptoms to be confirmed or excluded.
In conclusion, a rhinologic origin of a headache must be considered in a patient initially seen with a headache or facial pain. Medical or surgical therapy can be beneficial in the treatment of these patients with headaches or facial pains of rhinologic origin.
CONTACT POINT HEADACHE
Those patients who complain of headache without any clear etiology related to sinus or non-sinus disease must be evaluated for contact point headache.21)22) The recognition of contact points as a cause for this ir- ritating, sometimes even incapacitating problem has lead to relieving these anatomic abnormalities when surgical procedures are undertaken in the sinonasal
tract. A recent review of contact point headaches focuses on surgical treatment but, surprisingly, fails to describe the most common clinical features which should lead the clinician to suspect this diagnosis.23) It is not easy to find the primary cause in all cases.
Routine ear, nose, and throat studies and examinations by other related specialists may not define the origin of the headache. These patient must be evaluated for contact point headache.
Tosun et al., proposed criteria to diagnose contact point headaches21):1) History of chronic headache 2) Lack of acute or chronic inflammatory findings on the ear, nose and throat examination (anterior and posterior rhinoscopy, routine sinus radiographs, and CT scan 3) Absence of any other obvious cause of headaches after a thorough evaluation by a neurologist, ophthalmologist, dentist, internist, and other related specialist 4) Presence of contact points as documented by nasal endoscopy or CT scan, or both 5) Failure of medical therapy for headache 6) Relief of headache after applying topical anesthesia to the contact points 7) Contact points that still remain after mucosal de- congestion
Plain paranasal sinus radiology may help in screening the presence of paranasal sinus inflammatory disease, or any bony abnormalities;however, it rarely helps in the diagnosis of contact point rhinologic headache.
Computed tomography scan may be required only when routine measures fail to disclose the cause of pain.24) Coronal CT scan allows for the best interpre- tation of narrow compartments of the lateral nasal wall.
Septal spur, medially or laterally deviated or pneuma- tized turbinates, a large ethmoid bulla, or agger nasi cells that press on opposing mucosal surfaces must be detected carefully (Table 2).3) Septal spurs and ana- tomical variations of the middle turbinate were known to the major causes of the mucosal contact points.
Diagnostic endoscopy is the best method of evaluating pathological changes such as retention of secretion, mucosal hypertrophy, and polypoid degenerations of the soft tissues at the contact points. In conclusion, computed tomography and nasal endoscopy are the best methods for evaluating theses patients. If doubts about the surgical indication exist, local anesthesia of the contact point by cocaine- or Pontocaine -emb- edded cotton tipped probes may help the decision making.25)26)
After the localization of the pathology, a limited surgical intervention under local anesthesia is gene- rally sufficient treatment. After excision of the septal spurs, turbinoplasty and ethmoidectomy can be per- formed under endoscopic guidance. While resecting only the bony lateral half of the bullous middle turbinate to prevent contact point, the mucosa of the turbinate must be preserved, otherwise crusting in this area may cause secondary obstruction and impaction causing headache.27)28) A large ethmoid bulla, agger nasi cells, or Haller’s cell can be resected by a limited ethmoidectomy procedure.21)
In conclusion, intranasal contact point must be con- sidered in patients who have no other obvious cause of headache. Significant relief of headache can be ob- tained by surgery in selected cases. Satisfactory results were achieved by endonasal surgery in about 90% of patients in whom intranasal contact points were be- lieved to be the cause of their headaches.21)
SINUS HEADACHE
In 1943 McAuliffe et al., reported the results of an interesting experiment in which they stimulated various
areas within the nasal cavity and paranasal sinuses with a variety of noxious stimuli.29) As a result of their experiment, they determined that the mucos a around the sinus ostia were most sensitive to noxious stimuli.
The mucosa of the turbinates were less sensitive, and the mucosal of sinuses were least sensitive. Most important, they found that the pain was rarely felt at the affected sites, but rather referred to other areas of the head. Since then, various authors have reported on the association between various nasal and paranasal sinus pathologies and headaches or facial pains.30-35)
Diseases in the sinuses may present with frontal pain or pain radiating behind the eyes or to the vertex (frontal sinus), over the antral area or temporal area (maxillary), between and behind the eyes or to the temporal area (ethmoid), or between or behind the eyes or to the vertex (sphenoid).36) Sinus-related pain or headache usually described by patients as pressure- like or dull bilateral periorbital pain, usually radiating to the ears, usually worse in the morning and better as the day progresses, associated with nasal obstruction, not necessarily responsive to decongestants and antihi- stamine, described by patients as lasting days at a time, and not usually associated with nausea or visual dis- turbance. Sinus pain caused by inflammation induced by allergens or by infection occurs when exudate in inflamed, blocked sinuses exerts pressure that stimu- lates local trigeminal nerve fibers.37-39)
Headache is the main symptom in sphenoid sinus diseases, and cranial nerve symptoms are also north- worthy. Sphenoid sinus diseases are mostly inflam- matory in origin, and treatment cons ists of antibiotics drug administration:however, surgery might be ne- eded if drainage of the sinus cannot otherwise be guaranteed, the patient does not promptly respond to medical therapy, or if there are imminent complications.
Transnasal endoscopic sphenoidotomy is primarily recommended as a treatment for isolated sphenoid sinusitis.40-43)
The International Headache Society (IHS) diagnostic criteria for acute sinus headache include 1) purulent discharge, 2) pathologic sinus findings in tests inclu- ding X-ray, CT or MRI, and/or transillumination, 3) simultaneous onset of headache and sinusitis, and 4) headache localized to specific facial and cranial areas near the sinuses.8) Chronic sinusitis is not validated as a causes of headache unless relapsing into an acute
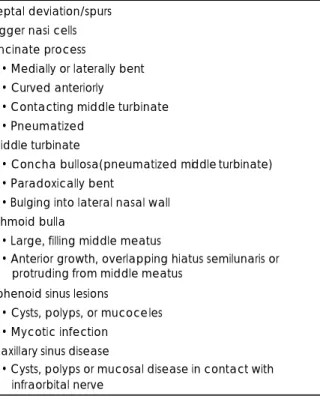
Table 2. Anatomic variations in nose and paranasal sinuses predisposing to headaches (seen on endoscopic examination, CT scan or both)
Septal deviation/spurs Agger nasi cells Uncinate process
• Medially or laterally bent
• Curved anteriorly
• Contacting middle turbinate
• Pneumatized Middle turbinate
• Concha bullosa(pneumatized middle turbinate)
• Paradoxically bent
• Bulging into lateral nasal wall Ethmoid bulla
• Large, filling middle meatus
• Anterior growth, overlapping hiatus semilunaris or protruding from middle meatus
Sphenoid sinus lesions
• Cysts, polyps, or mucoceles
• Mycotic infection Maxillary sinus disease
• Cysts, polyps or mucosal disease in contact with infraorbital nerve
phase.44) But, a negative sinus X-ray cannot rule out the possibility that a headache is of nasal origin, and that careful rhinologic examination is essential.45) Migraine and tension type headache are often confused with true sinus headache because of its similarity in location. Parasympathetic activation, as well as the hypothesized mechanism of neurogenic or immunoge- nic switching (i.e., crossover interactions of neurogenic and immunogenic inflammation), may account for both the frequent occurrence of nasal symptoms in migraine and the possibility that sinus inflammation can sometimes act as a migraine trigger.46-48) The differential diagnosis of migrain and sinus headache is crucial in determining the appropriate course of treat- ment.
There are many issues that obscure the distinction between primary headache disorders and sinusitis-re- lated pain. Changes in weather, seasons, and humidity levels are known precipitating factors in primary headache disorders and do not necessarily indicate a sinonasal cause of pain.49) Also, response of the headache to treatment directed to sinus pathology or the application of a local anesthetics to the nose should not be taken as diagnostic of sinus-related headache for the following reasons. 1) medications used to treat sinus pathology or to identify sinus causes of headache could have an affect on primary headache disorders.
The application of lidocaine to the nose has long been shown to relieve cluster headache.50) 2) regression to the mean can occur;simply stated, a headache suf- ferer has headaches with intensity around a certain mean, which he or she manages without consulting a physician.
The optimal treatments for sinus headache differ from those for migraine headache. Whereas treatment of true sinus headaches caused by allergy or micorbio- logic inflammation is directed at treating the underlying pathology, treatment of migraine headaches is directed at reducing craniovascular inflammation.
REFERENCES
1) Bathes R, Stephen Fogelson MH. Headache. In: Paparella, Schum- rich, Gluckman, Meyerhoff, editors. Otolaryngology. Philadelphia:
WB Saunders;1991. p.841-7.
2) Rasmussen BK, Olessen J. Symptomatic and nonsymptomatic headaches in a general population. Neurology 1992;42:1225-31.
3) Stammberger H, Wolf G. Headaches and sinus disease: the endo- scopic approach. Ann Otol Rhinol Laryngol Suppl 1988;134:3-23.
4) Chow JM. Rhinologic headaches. Otolaryngol Head Neck Surg 1944;111:211-8.
5) Landrigan GP, Kirkpatrick DA. Intranasal xylocaine: a prognostic aid for pre-operative assessment of facial pain of nasal origin. J Otolaryngol 1992;21:126-8.
6) Lance JW, Goadsby PJ. Mechanism and management of headache.
6th ed. Oxford: Butterworth-Heinemann;1988.
7) Moore GF, Massey JD, Emanuel JM, Hueter JV, Roh LH, Jones DT, et al. Head pain secondary to nasal allergy. Ear Nose Throat J 1987;66:502-11.
8) Headache Classification Committee of the International Headache Society. Classification of headaches disorders, cranial neuralgias and facial pain. Cephalagia 1988;8:1-96.
9) Silberstein SD. Practice parameter: evidence-based guidelines for migraine headache (an evidence-based review): report of the quality standards subcommittee of the american academy of neurology.
Neurology 2000;55:754-62.
10) Cady RK. Diagnosis of headache. In: Cady RK, Fox AW editor.
Treating the headache patient. New York NY: Marcel Decker;1995.
p.101-22.
11) Capobianco DJ, Cheshire WP, Campell JK. An overview of the di- agnosis and pharmacologic treatment of migraine. Mayo Clin Proc 1996;71:1055-66.
12) Lipton RB, Stewart WP, Cady RK. 2000 Wlofe Award: sumatrip- tan for the range of headaches in migraine sufferers: results of the spectrum study. Headache 2000;40:783-91.
13) Wespi HH, Stojan V. Kopschmerz bei deformation der nasen- scheidewand und bei beluftungsstorungen der nasennebenhohlen.
Schweiz Mschr Zahnheilk 1979;89:467-74.
14) Margenstein KM, Krieger MK. Experiences in middle turbinectomy.
Laryngoscope 1980;90:1596-603.
15) Brunner E, Jacobs JB, Shpizner BA, Lebowitz RA, Holliday RA.
Role of the agger nasi cell in chronic frontal sinusitis. Ann Otol Rhinol Laryngol 1996;105:694-700.
16) Wanamaker HH. Role of Haller’s cell in headache and sinus dis- ease: a case report. Otolaryngol Head Neck Surg 1996;114:324-7.
17) Moriyama H, Nakajima T, Honda Y. Studies on mucoceles of the ethmoid and sphenoid sinuses: analysis of 47 cases. J Laryngol Otol 1992;106:23-7.
18) Clerico DM. Sinus headaches reconsidered: referred cephalgia of rhinologic origin masquerading as refractory primary headaches.
Headache 1995;35:185-92.
19) Lanny GC, Jonathan A. Headaches and disease of the nose and paranasal sinuses. Semin Neurol 1997;17:351-4.
20) Tarabichi M. Characteristics of sinus-realted pain. Otolaryngol Head Neck Surg 2000;122:842-7.
21) Tosun F, Gerek M, Ozkaptan Y. Nasal surgery for contact point headache. Headache 2000;40:237-40.
22) Pinto A, De Rossi SS, McQuone S, Sollecito TP. Nasal mucosal headache presenting as orofacial pain : a review of the literature and a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;92:180-3.
23) Harvey JB. Headaches and sinus disease. Headache 2001;41:883-8.
24) Kunachak S. Middle turbinate lateralization: a simple treatment for rhinologic headache. Laryngoscope 2002;112:870-2.
25) Parsons DS, Batra PS. Functional endoscopic sinus surgical outco- mes for contact point headaches. Laryngoscope 1998;108:696-702.
26) Kamal SA. Experience with the xylocaine test as a prognostic aid for surgery in Sluder’s neuralgia. J Laryngol Otol 1995;109:193-5.
27) Anselmo-Lima WT, de Olivaira JA, Speciali JG, Bordini C, dos Santos AC, Rocha KV, et al. Middle turbinate headache syndrome.
Headache 1997;37:102-6.
28) Osama ES. The place of endonasal endoscopy in the relief of mi- ddle turbinate sinonasal headache syndrome. Rhinology 1995;33:
244-5.
29) McAuliffe GW, Goodell H, Wolff HG. Experimental studies on headache pain from the nasal and paranasal structures. Am Res Nerve and Ment Dis Proc 1942;23:185-208.
30) Hansen RM. Pain of nasal origin. Laryngoscope 1968;78:1164-71.
31) Masing H. Functional aspects in septal plasty. Rhinology 1977;15:
167-72.
32) Ryan SE Sr, Ryan RE Jr. Headache of nasal origin. Headache 1979;
19:173-9.
33) Koch-Henriksen N, Gammelgaard N, Hvidegaard T, Stoksted P.
Chronic headache: the role of deformity of the nasal septum. BMJ 1984;288:434-5.
34) Gerbe RW, Fry TL, Fischer ND. Headache of nasal spur origin: an easily diagnosed and surgical correctable cause of facial pain. Hea- dache 1984;24:329-30.
35) Whittet HB. Infraorbital nerve dehiscence: the anatomic cause of maxillary sinus “vacuum headache”? Otolaryngol Head Neck Surg 1992;107:21-8.
36) Lederer FL. Otolaryngolo gic aspects of headache and head pains.
Headache 1977;11:19.
37) Couch JR. Sinus headache: a neurologist’s viewpoint. Semin Neu- rol 1988;8:298-302.
38) Schuller DE, Cadman TE, Jeffreys WH. Recurrence headaches:
what every allergist should know. Ann Allergy Asthma Immunol 1996;76:219-30.
39) Close LG, Aviv J. Headaches and disease of the nose and parana- sal sinuses. Semin Neurol 1997;17:351-4.
40) Goldman GE, Fontanarosa PB, Anderson JM. Isolated sphenoid sinusitis. Am J Emerg Med 1993;11:235-8.
41) Silberstein SD. Intractable headache: aseptic meningitis and sphe- noid sinusitis. Cephalagia 1994;14:376-8.
42) Postma GN, Chole RA, Nemzek WR. Reversible blindness seco- ndary to acute sphenoid sinusitis. Otolaryngol Head Neck Surg 1995;112:742-6.
43) Seiden AM. Isolated sphenoid sinusitis: problems in diagnosis and therapy. Am J Rhinol 1995;9:229-35.
44) Williams H. Vasotonic headache associated with chronic maxillary sinusitis. Headache 1968;7:156-62.
45) Schonsted MU, Stoksted P, Christensen PH, Koch HN. Chronic headache related to nasal obstruction. J Laryngol Otol 1986;100:
165-70.
46) Roger KC, Curtis P, Schreiber. Sinus headache or migraine?: con- siderations in making a differential diagnosis. Neurology 2002;14 (suppl 6):S10-4.
47) Buzzi MG, Bonamini M, Cerbo R. The anatomy and biochemistry of headache. Funct Neurol 1933;8:395-402.
48) Meggs WJ. Neurogenic switching: a hypothesis for a mechanism for shifting the site of inflammation in allergy and chemical sen- sitivity. Environ Health Perspect 1995;103:54-6.
49) Robbins L. Precipitating factors in migraine: retrospective review of 494 patients. Headache 1994;34:214-6.
50) Kittrelle JP, Grouse DS. Cluster headache: local anesthetic abortive agents. Arch Neurol 1985;42:496-8.