Vol. 17, No. 2, November, 2009 □ 종 설 □
1)
서 론
,
, (hypnagogic) (hypnapompic) ,
: 2009 10 20 , : 2009 10 28
: , CHA
Tel : 031)780-5229, Fax : 031)780-5239 Email : barnabas@cha.ac.kr
. (excessive daytime sleepiness)
,
.
. 2 (International Clas-
소아 기면증의 진단과 치료
, CHA *
방 양 원 채 규 영*․
= Abstract =
Pediatric Narcolepsy - Diagnosis and Treatment
Yang Weon Bang, M.D. and Kyu Young Chae, M.D., Ph.D.
Division of Child and Adolescent Psychiatry, Department of Psychiatry, Keyo Hospital Division of Pediatric Neurology, Department of Pediatrics, CHA University
Narcolepsy is chronic devastating disease that characterized by excessive daytime slee- piness, cataplexy, which often precipitated by intense emotion or excitement, hypnagogic, or hypnapompic hallucinations, sleep paralysis and nocturnal disrupted sleep. In child onset narcolepsy, the presentations of narcolepsy can be very variable, making misdiagnosis as seizure disorders or delaying diagnosis as much as several years after disease onset. For the diagnosis of narcolepsy, overnight polysomnography(PSG) and multiple sleep latency test(MSLT) should be evaluated. Test for Cerebrospinal fluid hypocretin(orexin) concentra- tion and human leukocyte antigens(HLA) would be great helpful to confirm the narcolepsy with cataplexy even in early stage of disease in children. The mainstays of treatment are that reducing the excessive daytime sleepiness, preventing the intrusion of the REM related phenomena including cataplexy and consolidating the nighttime sleep. Central nervous sys- tem stimulators such as methylphenidate or amphetamine decrease excessive daytime slee- piness and tricyclic antidepressant(TCA) or selective serotonin reuptake inhibitors(SSRI) can prevent cataplexy. Recently, new therapeutic agents such as modafinil and sodium oxybate are emerging in clinical practice with much effectiveness. Counseling for poor school performance, social isolation and depression should be provided. Early diagnosis and treatment can greatly improve the quality of life. Awareness of excessive daytime sleepi- ness in children or adolescent will allow pediatricians to effectively identify hypersomnia such as narcolepsy.
Key Words : Narcolepsy, Diagnosis, Treatment, Children, Adolescents
sification of Sleep Disorder, ICSD-2)
1) , 2)
, 3)
4)
1).
.
본 론
기면증의 임상적인 특징 1.
과다 졸음증
1) (Excessive sleepiness)
2)
.
.
.
, 10-30
.
. 5 ,
. 탈력발작
2) (Cataplexy)
3)
. ,
.
.
.
. . (status cataplec-
ticus) .
10-20%
4)
. 5
(atonic seizure)
5, 6)
.
, . 수면마비
3) (Sleep paralysis)
.
. 40-80%
7)
.
.
4) 입면 출면시 / 환각(Hypnagogic/hypnapo mpic hallucination)
40-80%
8).
(cenesthopathic feeling)
4)
.
. 기타 증상
5)
(sleep frag-
mentation)
.
.
(ex- cessive twitching),
9)
.
(REM sleep behavior disorder,
RBD)
10).
,
10-12)
. 유병률
6)
.
0.05%, 0.18%
0.02%
8, 13).
1/4 .
0.04%
14)
.
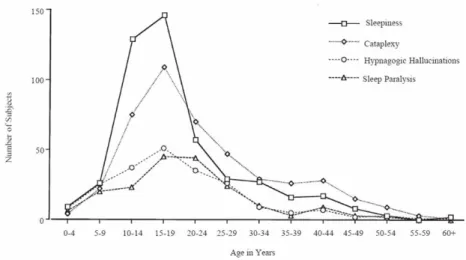
. 10
20 30 10
(Fig. 1)
15, 16). 14.7 35
, 23.5 24.5
17). 원 인
7)
1990 hypocretin(orexin)
18)
4)
. Hypocretin
19)
. Hypocretin hypocretin-1 hypo-
cretin-2 pre-
prohypocretin
20).
(dorsolateral
hypothalamus) (locus coeru-
leus), (dorsal raphe), (amygdale), (basal forebrain), (suprachias-
Fig. 1. Age of onset of sleepiness, cataplexy, hypnagogic hallucinations, and sleep paralysis in 469, 438, 210 and 189 patients, respectively. The number of subjects with onset at each age range is plotted. Note that sleepiness onset is generally earlier than the other symptoms(Cited from Okun ML, Sleep 2002).
matic nucleus), (cholinergic brain- stem nuclei)
21)
. Hypocretin
serotonin, histamine, acetylcholine, dopamine, GABA(gamma-aminobutyric acid)
(glutamate)
22, 23)
. Hypocretin
/ hypo-
cretin-2
hypocretin
24, 25)
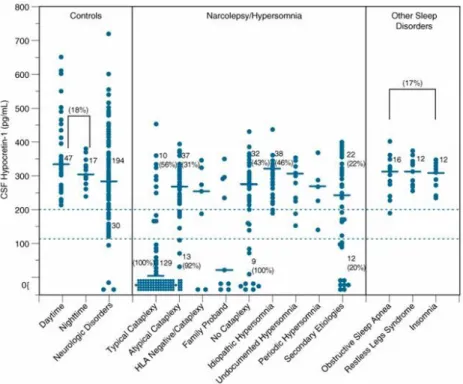
. 2001
hy-
pocretin-1
26)hypocretin- 1 110 pg/mL
27)
.
200 pg/mL (Fig.
2)
27).
(sleep-onset REM periods, SOREMPs)
26)
. hypocretin-1 88.5%, 99.1%
27).
(idiopathic hypersomnolence), Klein-Levin
28)
. Hypocretin-1
27)
. Hypocretin
(Fig.
3)
29, 30),
Fig. 2. Cerebrospinal fluid(CSF) hypocretin-1(Hcrt-1) concentrations are plot- ted for individuals across various control and sleep disorders. Each point represents the crude concentration of Hcrt-1 in a single person. The cutoffs for normal(>200 pg/mL) and low(<110 pg/mL) Hcrt-1 concentrations are shown. The median value in each group is shown as a
horizontal bar
(Cited from Mignot E, Arch Neurol 2002).31)
hy- pocretin
32)
.
(human leukocyte antigen: HLA)
, HLA
DQB1*0602
33). 40%
24%
33)
. HLA DQB1*0602 Hcrt-1
.
.
10-40
34)
. 25-31%
35)
. 진 단
8)
, (fragmented sleep), .
, (circadian rhythm sleep disor-
ders), .
(sleep-onset association disorders),
( ,
), (parasomnia),
( , ),
.
,
. 6
10 2
4-5 (multiple
sleep latency test, MSLT)
. 15
(Fig. 4).
60-90 .
15-20 8
36)
.
8
(Table 1). 5
70%, 97%
36, 37).
36, 38)
.
hypocretin-1 HLA
. DQB1*
0602 76-90
% DQB1*0602
hypocretin-1 110 pg/mL
(Fig. 5)
26).
Fig. 3. Preprohypocretin messenger RNA staining(in situ hybridization) in a narcoleptic human brain hypothalamus (A) contrasted with control (B). Each dot in the control represents a hypo- cretin-producing cell. Note that most of these cells are located close to the fornix area, a white matter tract (f). The dramatic loss of the hypo- cretin signal is evident in the narcoleptic brain (Cited from Peyron C, brains. Nat Med 2000).
1/5-1/3 . 6
1/4 (status cataplecticus)
39)
.
(Prader Willi , Niemann Pick C , Myotonic dystrophy type I, Norrie ,
Coffin-Lowry ), ( ,
),
40)
.
.
.
Kleine-
Levin
41).
50%
42)
.
. Klein-Levin
, ,
41)
. 치 료
2.
비약물 치료 1)
. ,
. ,
.
4-5 15
.
,
, .
.
43)
. 2) 약물치료
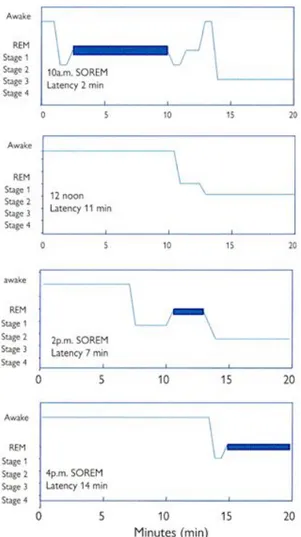
Fig. 4. Example of a multiple sleep latency test in narcolepsy. At the 10 a.m., 2 p.m., and 4 p.m.
sleep opportunities, the patient had a period of REM sleep(thick line) near sleep onset(SOREM).
Mean sleep latency is 8 min(Cited from Wilson S: Narcolepsy. In: Sleep Disorders. 2008).
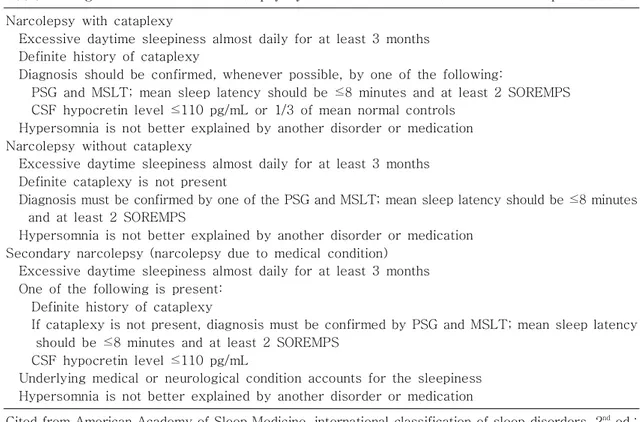
Table 1. Diagnostic Criteria for Narcolepsy by the International Classification of Sleep Disorders Narcolepsy with cataplexy
Excessive daytime sleepiness almost daily for at least 3 months Definite history of cataplexy
Diagnosis should be confirmed, whenever possible, by one of the following:
PSG and MSLT; mean sleep latency should be ≤8 minutes and at least 2 SOREMPS CSF hypocretin level ≤110 pg/mL or 1/3 of mean normal controls
Hypersomnia is not better explained by another disorder or medication Narcolepsy without cataplexy
Excessive daytime sleepiness almost daily for at least 3 months Definite cataplexy is not present
Diagnosis must be confirmed by one of the PSG and MSLT; mean sleep latency should be≤8 minutes and at least 2 SOREMPS
Hypersomnia is not better explained by another disorder or medication Secondary narcolepsy (narcolepsy due to medical condition)
Excessive daytime sleepiness almost daily for at least 3 months One of the following is present:
Definite history of cataplexy
If cataplexy is not present, diagnosis must be confirmed by PSG and MSLT; mean sleep latency should be ≤8 minutes and at least 2 SOREMPS
CSF hypocretin level ≤110 pg/mL
Underlying medical or neurological condition accounts for the sleepiness Hypersomnia is not better explained by another disorder or medication
Cited from American Academy of Sleep Medicine, international classification of sleep disorders, 2nded.:
diagnostic and coding manual. 2005
Fig. 5. Diagnostic flow chart for clinical evaluation of hypersomnia.
.
, , ,
,
.
, . . methylphenidate amphe- tamine
. Ampheta- mine
methylpheni-
date . Methylphenidate
5 mg
5-10 mg 60 mg
. 25 kg
45 mg
44).
, , ,
, .
Modafinil
45)
. Modafinil
(mo-
noamine) (amygdale)
histamine
. 100
mg 100-200 mg
(200-400 mg/day) .
2
. , ,
. Stevens-Johnson .
.
(Tricyclic antidepressant)
. norepine-
phrine serotonin
. Clomipramine
. 25 mg
200 mg 3 mg/kg
. desipramine, imi- pramine, protryptylin
46).
, , , ,
, ,
5)
.
(selective serotonin reuptake in- hibitor)
. Fluoxetine
10 mg 20 mg
. , , ,
, . Venlafaxine serotonin norepinephrine
. 37.5 mg
75-300 mg
46). atomoxetine
47)
. modafinil
serotonin
9)
. Sodium oxybate 16
GABA(gamma-aminobutyric
acid) B .
.
. seroto-
nin, dopamine, opioid
48)
. 0.5-1 2.5-4
. 4.5 g
6-9 g .
49)
.
.
50)
.
결 론
, ,
,
. 15
. 10
. ,
. 90%
HLA DQB1 0602 hypocretin
(Hypocretin-1) 110 pg/mL .
.
.
.
.
References
1) Medicine AAoS. International Classification of Sleep Disorders, 2nd ed.: Diagnostic and coding manual 2005.
2) Wise MS, Lynch J. Narcolepsy in children.
Semin Pediatr Neurol 2001;8:198-206.
3) Serra L, Montagna P, Mignot E, Lugaresi E, Plazzi G. Cataplexy features in childhood nar- colepsy. Mov Disord 2008;23:858-65.
4) Nishino S. Clinical and neurobiological aspects of narcolepsy. Sleep Med 2007;8:373-99.
5) Stores G. The protean manifestations of child- hood narcolepsy and their misinterpretation.
Dev Med Child Neurol 2006;48:307-10.
6) Thorpy M. Current concepts in the etiology, diagnosis and treatment of narcolepsy. Sleep Med 2001;2:5-17.
7) Guilleminault C, Fromherz S. Narcolepsy: diag- nosis and management. In: Kryger MH, Roth T, Dement WC, editors. Principles and practice of sleep medicine. 4th ed. Philadelphia, Else- vier/Saunders, 2005:780-90.
8) Overeem S, Mignot E, van Dijk JG, Lammers GJ. Narcolepsy: clinical features, new pathophy- siologic insights, and future perspectives. J Clin Neurophysiol 2001;18:78-105.
9) Vendrame M, Havaligi N, Matadeen-Ali C, Adams R, Kothare SV. Narcolepsy in children:
a single-center clinical experience. Pediatr Ne- urol 2008;38:314-20.
10) Nevsimalova S, Prihodova I, Kemlink D, Lin L, Mignot E. REM behavior disorder (RBD) can be one of the first symptoms of childhood narcolepsy. Sleep Med 2007;8:784-6.
11) Gagnon JF, Postuma RB, Mazza S, Doyon J, Montplaisir J. Rapid-eye-movement sleep be- haviour disorder and neurodegenerative dis- eases. Lancet Neurol 2006;5:424-32.
12) Mosko SS, Shampain DS, Sassin JF. Nocturnal REM latency and sleep disturbance in narcole- psy. Sleep 1984;7:115-25.
13) Mignot E. Genetic and familial aspects of nar- colepsy. Neurology 1998;50:S16-22.
14) Han F, Chen E, Wei H, Dong X, He Q, Ding D, et al. Childhood narcolepsy in North China.
Sleep 2001;24:321-4.
15) Silber MH, Krahn LE, Olson EJ, Pankratz VS.
The epidemiology of narcolepsy in Olmsted County, Minnesota: a population-based study.
Sleep 2002;25:197-202.
16) Okun ML, Lin L, Pelin Z, Hong S, Mignot E.
Clinical aspects of narcolepsy-cataplexy across ethnic groups. Sleep 2002;25:27-35.
17) Dauvilliers Y, Montplaisir J, Molinari N, Car- lander B, Ondze B, Besset A, et al. Age at onset of narcolepsy in two large populations of patients in France and Quebec. Neurology 2001;57:2029-33.
18) Nishino S, Ripley B, Overeem S, Lammers GJ, Mignot E. Hypocretin (orexin) deficiency in human narcolepsy. Lancet 2000;355:39-40.
19) Sutcliffe JG, de Lecea L. The hypocretins: ex- citatory neuromodulatory peptides for multiple homeostatic systems, including sleep and fee- ding. J Neurosci Res 2000;62:161-8.
20) Sakurai T, Amemiya A, Ishii M, Matsuzaki I, Chemelli RM, Tanaka H, et al. Orexins and orexin receptors: a family of hypothalamic neuropeptides and G protein-coupled receptors that regulate feeding behavior. Cell 1998;92:
573-85.
21) Peyron C, Tighe DK, van den Pol AN, de Lecea L, Heller HC, Sutcliffe JG, et al. Neur- ons containing hypocretin (orexin) project to multiple neuronal systems. J Neurosci 1998;18:
9996-10015.
22) Willie JT, Chemelli RM, Sinton CM, Yanagisa- wa M. To eat or to sleep? Orexin in the re- gulation of feeding and wakefulness. Annu Rev Neurosci 2001;24:429-58.
23) Taheri S, Zeitzer JM, Mignot E. The role of hypocretins (orexins) in sleep regulation and narcolepsy. Annu Rev Neurosci 2002;25:283- 313.
24) Lin L, Faraco J, Li R, Kadotani H, Rogers W, Lin X, et al. The sleep disorder canine narco- lepsy is caused by a mutation in the hypocre- tin (orexin) receptor 2 gene. Cell 1999;98:365- 76.
25) Chemelli RM, Willie JT, Sinton CM, Elmquist
JK, Scammell T, Lee C, et al. Narcolepsy in orexin knockout mice: molecular genetics of sleep regulation. Cell 1999;98:437-51.
26) Nishino S, Ripley B, Overeem S, Nevsimalova S, Lammers GJ, Vankova J, et al. Low cere- brospinal fluid hypocretin (Orexin) and altered energy homeostasis in human narcolepsy. Ann Neurol 2001;50:381-8.
27) Mignot E, Lammers GJ, Ripley B, Okun M, Nevsimalova S, Overeem S, et al. The role of cerebrospinal fluid hypocretin measurement in the diagnosis of narcolepsy and other hyper- somnias. Arch Neurol 2002;59:1553-62.
28) Dauvilliers Y, Baumann CR, Carlander B, Bis- chof M, Blatter T, Lecendreux M, et al. CSF hypocretin-1 levels in narcolepsy, Kleine-Levin syndrome, and other hypersomnias and neuro- logical conditions. J Neurol Neurosurg Psy- chiatry 2003;74: 1667-73.
29) Mignot E. Sleep, sleep disorders and hypocre- tin (orexin). Sleep Med 2004;5 Suppl 1:S2-8.
30) Peyron C, Faraco J, Rogers W, Ripley B, Overeem S, Charnay Y, et al. A mutation in a case of early onset narcolepsy and a gene- ralized absence of hypocretin peptides in hu- man narcoleptic brains. Nat Med 2000;6:991-7.
31) Dauvilliers Y, Carlander B, Rivier F, Touchon J, Tafti M. Successful management of cataple- xy with intravenous immunoglobulins at nar- colepsy onset. Ann Neurol 2004;56:905-8.
32) Black JL, 3rd, Krahn LE, Pankratz VS, Silber M. Search for neuron-specific and nonneuron- specific antibodies in narcoleptic patients with and without HLA DQB1*0602. Sleep 2002;25:
719-23.
33) Mignot E. Genetics of narcolepsy and other sleep disorders. Am J Hum Genet 1997;60:
1289-302.
34) Nishino S, Okura M, Mignot E. Narcolepsy:
genetic predisposition and neuropharmacological mechanisms. Sleep Med Rev 2000;4:57-99.
35) Maret S, Tafti M. Genetics of narcolepsy and other major sleep disorders. Swiss Med Wkly 2005;135:662-5.
36) Littner MR, Kushida C, Wise M, Davila DG, Morgenthaler T, Lee-Chiong T, et al. Practice parameters for clinical use of the multiple sleep latency test and the maintenance of wakeful- ness test. Sleep 2005;28:113-21.
37) Arand D, Bonnet M, Hurwitz T, Mitler M, Rosa R, Sangal RB. The clinical use of the MSLT and MWT. Sleep 2005;28:123-44.
38) Aldrich MS, Chervin RD, Malow BA. Value of the multiple sleep latency test (MSLT) for the diagnosis of narcolepsy. Sleep 1997;20:620-9.
39) Challamel MJ, Mazzola ME, Nevsimalova S, Cannard C, Louis J, Revol M. Narcolepsy in children. Sleep 1994;17:S17-20.
40) Nishino S, Kanbayashi T. Symptomatic narco- lepsy, cataplexy and hypersomnia, and their implications in the hypothalamic hypocretin/
orexin system. Sleep Med Rev 2005;9:269-310.
41) Guilleminault C, Brooks SN. Excessive day- time sleepiness: a challenge for the practising neurologist. Brain 2001;124:1482-91.
42) Broughton R, Ghanem Q, Hishikawa Y, Sugita Y, Nevsimalova S, Roth B. Life effects of nar- colepsy in 180 patients from North America, Asia and Europe compared to matched con- trols. Can J Neurol Sci 1981;8:299-304.
43) Morgenthaler TI, Kapur VK, Brown T, Swick TJ, Alessi C, Aurora RN, et al. Practice para- meters for the treatment of narcolepsy and other hypersomnias of central origin. Sleep 2007;30:1705-11.
44) Greenhill LL, Pliszka S, Dulcan MK, Bernet
W, Arnold V, Beitchman J, et al. Practice pa- rameter for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry 2002;41:26S-49S.
45) Littner M, Johnson SF, McCall WV, Anderson WM, Davila D, Hartse SK, et al. Practice parameters for the treatment of narcolepsy:
an update for 2000. Sleep 2001;24:451-66.
46) Dauvilliers Y, Arnulf I, Mignot E. Narcolepsy with cataplexy. Lancet 2007;369:499-511.
47) Kratochvil CJ, Vaughan BS, Harrington MJ, Burke WJ. Atomoxetine: a selective noradrena- line reuptake inhibitor for the treatment of attention-deficit/hyperactivity disorder. Expert Opin Pharmacother 2003;4:1165-74.
48) Thorpy M. Therapeutic advances in narcolepsy.
Sleep Med 2007;8:427-40.
49) Lammers GJ, Arends J, Declerck AC, Ferrari MD, Schouwink G, Troost J. Gammahydroxy- butyrate and narcolepsy: a double-blind place- bo-controlled study. Sleep 1993;16:216-20.
50) Hecht M, Lin L, Kushida CA, Umetsu DT, Taheri S, Einen M, et al. Report of a case of immunosuppression with prednisone in an 8- year-old boy with an acute onset of hypocre- tin-deficiency narcolepsy. Sleep 2003;26:809-10.