성인 남녀에서 혈장 Vitamin D 농도와 상완-발목 동맥맥파속도의 연관성
건양대학교 의과대학 가정의학교실
박근진․김민우․유병연․강지현
Association between Plasma Vitamin D Level and Brachial-ankle Pulse Wave Velocity
Kun-Jin Park, Min-Woo Kim, Byung-Yeon Yu, Jee-Hyun Kang Department of Family Medicine, Konyang University Hospital, Daejeon, Korea
Objectives: Low 25 (OH) vitamin D increases the risk of cardiovascular disease and mortality. Pulse wave velocity (PWV), which is related with arterial stiffness, can be used evaluate the severity of systemic atherosclerosis. Brachial-ankle PWV (baPWV) is affected by sex, age, systolic blood pressure, body mass index, and waist circumference. We evaluated determinants of PWV in Korean adults andits associationwith the plasma vitamin D level and arterial stiffness.
Materials and Methods: The study was conducted on 178 adults (>age of 20) who visited thehealth promotion center. We investigated medical history, medication, smoking and alcohol use by means of questionnaire. We measuredblood pressure, pulse rate, fasting glucose, fasting insulin, lipid profile, hs-CRP, plasma 25 (OH) vitamin D level, and baPWV. We then analyzed retrospectively the relationship between baPWV and various risk factors.
Results: The mean ages in 97 males and 81 females were 47.9±13 and 43.6±11.4 years, respectively. baPWV is correlated with age, BMI, waist, blood pressure, fasting glucose, HTN, DM, total cholesterol, triglyceride, hs-CRP, and 25 (OH) vitamin D. We found out that age (β=7.49, P<0.001), BMI (β=-10.05, P=0.023), SBP (β=7.69, P<0.001), TG (β=111.41, P=0.039), and fasting glucose (β=1.447, P=0.561) were independent predictors of baPWVafter performing multiple linear regression analysis.
Conclusions: baPWV was affected by age, SBP, BMI, TG, and fasting glucose. Deficiency of 25 (OH) vitamin Dwas not associated with baPWV after adjusting the risk factors of cardiovascular diseases in this study group.
Key Words: 25 (OH) vitamin D, Brachial-ankle pulse wave velocity, Arterial stiffness, Cardiovascular disease
Received: March 5, 2012 Revised: March 9, 2012 Accepted: March 20, 2012
Corresponding Author: Jee-Hyun Kang, Department of Family Medicine, Konyang University Hospital, 158 Gwanjeodong- gil, Seo-gu, Daejeon 302-801, Korea
Tel: +82-42-600-9240, Fax: +82-42-600-9095 E-mail: [email protected]
비타민 D는 칼슘 대사와 뼈의 성장 유지뿐 아니 라 근골격계 기능 및 심혈관 질환, 암
1,2등과 관련 있는 것으로 알려져 있다. 또한 혈관 내피 세포에 작
용, 레닌 촉진 유전자를 억제하여 레닌 생성을 낮출
뿐 아니라, 부갑상선 호르몬 조절, 혈관 석회화에 작
용하여 고혈압, 인슐린 저항성, 좌심실 비대와도 관
련이 있는 것으로 보고되고 있다.
3-9비타민 D 수용
체와 비타민 D를 활성형으로 전환하는 데 필요한
1-hydroxylase는 인체 내 다양한 조직과 세포에서 나
타나는 것으로 알려졌다. 비타민 D는 25-hydroxy-
vitamin D 형태로 체내에서 이용되며,
1030 ng/mL 이
상이면 체내에 충분한 양이 존재하는 것으로 여겨진 다. 최근 우리나라의 경우 폐경 여성의 92%가 30 ng/mL 미만으로 확인되어
11심각한 건강문제로 인식 되고 있다. 상완-발목 맥파속도는 동맥의 죽상동맥 경화증을 측정하기 위해 비침습적으로 동맥의 경직 도를 측정하는 방법으로
12,13맥파속도와 심혈관계 질 환 간의 연관관계에 대해서 여러 연구들이 발표 되
었다.
14,15최근 연구들에 의하면 특히, 상완-발목 맥
파속도는 타당성 및 재현성이 현저하게 높은 것으로 알려져 있다.
16-18비타민 D는 연령 및 죽상경화의 위 험인자와는 독립적으로 심혈관 질환의 강력한 예측 인자이며, 사망률을 예측할 수 있을 것으로 보고 있 다.
19본 연구에서는 20세 이상의 성인남녀를 대상으로 상완-발목 맥파속도에 영향을 주는 요인을 알아보 고, 혈중 비타민 D 농도가 혈관의 경직도와 연관이 있는지 알아보고자 하였다.
대상 및 방법
1. 연구대상
2011년 3월 1일부터 4월 31일까지 대전 일개병원 건강검진센터에 방문한 20세 이상의 남, 여 256명을 대상으로 하였다. 모든 대상자에서 일반적인 신체계 측, 현 병력을 조사하였으며, 공복 상태에서 혈청 지 질검사를 포함한 일반화학검사를 시행하였다. 상완- 발목 맥파속도, 25 (OH) vitamin D 항목이 누락된 78 명을 제외한 178명을 대상으로 분석하였다.
2. 방법
1) 문진, 신체계측
모든 환자에서 연령, 성별, 나이 흡연 유무, 과거 력 및 약물 복용력 등을 조사하였으며, 앙와위에서 5분간 휴식 후에 혈압 및 맥압을 측정하였고, 신장, 체중, 허리둘레 체질량지수를 측정하였다. 체질량 지수는 몸무게(kg)를 키의 제곱(m
2)으로 나누어 계산 하였다. 음주력을 토대로 1주일간의 평균 알코올 섭 취량을 구하였으며, 이는 소주 한 병당 알코올 양을 72 g으로 하여 주당 평균 음주 횟수와 양을 이용하 여 산출하였다. 흡연자는 현재 흡연자와 비흡연자로
나누었고, 6개월 이상 금연한 경우 비흡연자로 분류 하였다. 고혈압은 현재 혈압 강하제를 복용중인 경 우와 수축기 혈압과 이완기 혈압이 140 mmHg, 90 mmHg 이상으로 정의하였다.
2) 생화학적 검사
최소 12시간 이상 공복 후 혈액을 채취하여 고감 도 C-반응단백, 총 콜레스테롤, 중성지방, 고밀도 지 질 콜레스테롤, 저밀도 지질 콜레스테롤을 측정하였 고, 공복혈당, 공복 인슐린을 측정하였다. 이를 이용 해서 homeostasis model assessment of insulin re- sistance (HOMA-IR)를 계산하였다[{공복혈당(mg/dL)/
18×공복 인슐린(μU/mL)}/22.5].
3) 상완-발목 맥파속도의 측정
최소 5분간 누워 휴식을 취한 후 맥파 파형 분석 기(VP-2000, Colin Co, Komaki, Japen)을 이용하여 측 정하였다. 사지의 혈압은 진동방법을 이용하여 측정 하였고, 이를 통해 발목-상완 혈압지수가 자동으로 계산되었으며, 우측 상완-발목 맥파속도, 좌측 상완- 발목 맥파속도 및 평균 상완-발목 맥파속도도 동시 에 측정되었다.
4) 통계분석
통계분석은 SPSS for window version 14.0 (SPSS Inc., Chicago, IL, USA)을 이용하였고, 측정치는 평 균과 표준편차로 표시하였다. 남녀 간의 차이는 T- 검정과 카이제곱을 이용하여 비교하였다. 상완-발목 맥파속도와 혈중 비타민 D 농도를 포함한 다양한 변수들과의 상관관계는 pearson 상관분석을 시행하 였고, 또한 혈중 비타민 D가 상완-발목 맥파속도에 영향을 주는 독립적인 변수로 작용하는지 알아보기 위해 다중 회귀분석을 시행하였다. P<0.05인 경우에 통계적으로 유의성 있는 것으로 판정하였다.
결 과
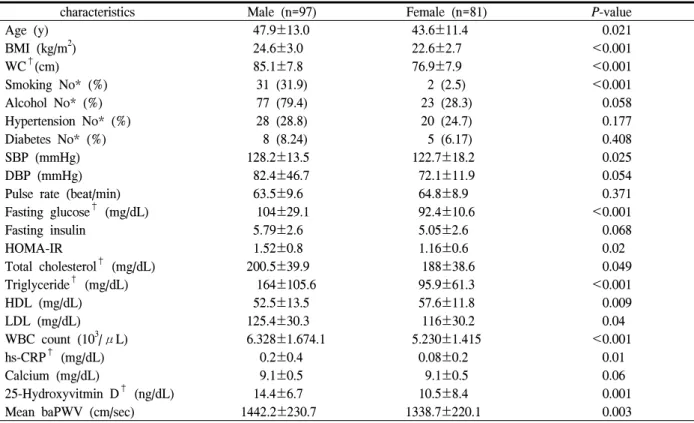
1. 연구 대상자들의 임상적 특징
연구 대상자는 총 178명으로 남자 97명(47.9±13.0
세), 여자 81명(43.6±11.4세)이었으며, 체질량지수 및
characteristics Male (n=97) Female (n=81) P-value
Age (y) 47.9±13.0 43.6±11.4 0.021
BMI (kg/m
2) 24.6±3.0 22.6±2.7 <0.001
WC
†(cm) 85.1±7.8 76.9±7.9 <0.001
Smoking No* (%) 31 (31.9) 2 (2.5) <0.001
Alcohol No* (%) 77 (79.4) 23 (28.3) 0.058
Hypertension No* (%) 28 (28.8) 20 (24.7) 0.177
Diabetes No* (%) 8 (8.24) 5 (6.17) 0.408
SBP (mmHg) 128.2±13.5 122.7±18.2 0.025
DBP (mmHg) 82.4±46.7 72.1±11.9 0.054
Pulse rate (beat/min) 63.5±9.6 64.8±8.9 0.371
Fasting glucose
†(mg/dL) 104±29.1 92.4±10.6 <0.001
Fasting insulin 5.79±2.6 5.05±2.6 0.068
HOMA-IR 1.52±0.8 1.16±0.6 0.02
Total cholesterol
†(mg/dL) 200.5±39.9 188±38.6 0.049
Triglyceride
†(mg/dL) 164±105.6 95.9±61.3 <0.001
HDL (mg/dL) 52.5±13.5 57.6±11.8 0.009
LDL (mg/dL) 125.4±30.3 116±30.2 0.04
WBC count (10
3/μL) 6.328±1.674.1 5.230±1.415 <0.001
hs-CRP
†(mg/dL) 0.2±0.4 0.08±0.2 0.01
Calcium (mg/dL) 9.1±0.5 9.1±0.5 0.06
25-Hydroxyvitmin D
†(ng/dL) 14.4±6.7 10.5±8.4 0.001
Mean baPWV (cm/sec) 1442.2±230.7 1338.7±220.1 0.003
Data are presented as mean (SD) unless otherwise indicated, *Data are presented as number (%).
P–values are calculated by student t-test or chi-square test.
BMI: body mass index; WC: waist circumference; SBP: systolic blood pressure; DBP: diastolic blood pressure; HOMA-IR:
homeostasis model assessment of insulin resistance; HDL: high density lipoprotein cholesterol; LDL: low density lipoprotein cholesterol; WBC: White blood cell; hs-CRP: high sensitive C-reactive protein; baPWV: brachial-ankle pulse wave velocity.
†
Values have been analysed after log-transformation.
Table 1. General characteristics of subjects
허리둘레는 남성에서 더 큰 것으로 나타났다. 수축기 혈압은 남녀 각각 128.2±13.5 mmHg vs 122.7±18.2 mmHg, P-value=0.025로 남자에서 유의하게 높았다.
고혈압 및 당뇨의 기왕력은 남자에서 많았으나 양군 간의 유의한 차이를 보이지 않았다. 혈중 비타민 D농 도는 남녀 14.4±6.7 ng/dL vs 10.5±8.4 ng/dL, P-value=
0.001, 상완-발목 맥파속도는 남녀 1442.2±230.7 cm/sec vs 1338.7±220.1 cm/sec, P=0.003으로 남자에 서 유의하게 높은 것으로 확인되었다(Table 1).
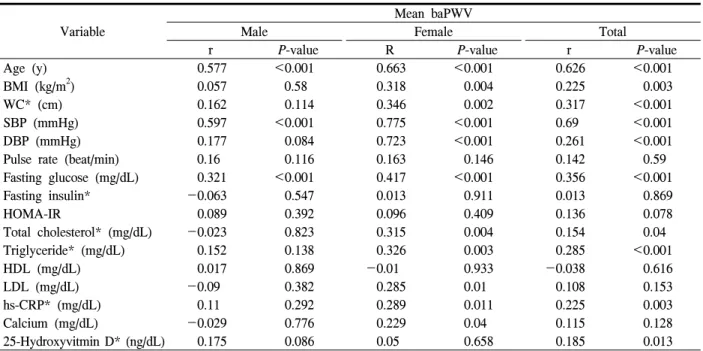
2. 상완-발목 맥파속도와 심혈관계 위험 인자들과 의 상관관계
상완-발목 맥파속도와 관련된 변수를 확인하기 위 해 pearson 상관 분석을 시행한 결과 연령(r=0.626,
P<0.001), 체질량지수(r=0.225, P=0.003), 허리둘레(r=0.317, P<0.001), 수축기혈압(r=0.690, P<0.001), 이완 기 혈압(r=0.261, P<0.001), 공복혈당(r=0.356, P<
0.001), 총콜레스테롤(r=0.154, P=0.040), 중성지방 (r=0.285, P<0.001), 고민감도 C-반응단백(r=0.225 P=
0.003), 비타민 D (r=0.185, P=0.013)는 상완-발목 맥파 속도와 유의한 상관관계를 보았으나 공복 인슐린, HOMA-IR, 고혈압, 고밀도 지질단백, 저밀도 지질단 백, 칼슘과는 상관관계를 보이지 않았다(Table 2).
남자에서는 연령(r=0.577, P<0.001), 수축기혈압(r=
0.597, P<0.001), 공복혈당(r=0.321, P<0.001)과 상완- 발목 맥파속도가 유의한 상관관계를 나타났으며, 여 성에서는 나이(r=0.663, P<0.001), 체질량지수(r=
0.318, P=0.004), 허리둘레(r=0.114, P=0.002), 수축기 혈압(r=0.775, P<0.001), 이완기혈압(r=0.723, P<
0.001), 공복혈당(r=0.417, P<0.001), 고혈압(r=0.312,
Variables Mean baPWV
β S.E P-value
Sex -0.89 26.35 0.973
Age (year) 7.49 1 <0.001
BMI *(kg/m
2) -10.05 4.37 0.023
SBP (mmHg) 7.69 0.89 <0.001
DBP (mmHg) -0.17 0.32 0.602
Smoking -2.62 33.05 0.937
Fasting glucose (mg/dL) 1.45 0.561 0.011
TG* (mg/dL) 111.4 53.54 0.039
LDL (mg/dL) -0.33 0.38 0.396
25-Hydroxyvitmin D* (ng/dL) 3 52.48 0.954
hs-CRP* (mg/dL) 42.14 24.59 0.089
Coefficient (β): parameter estimate, P-values by multiple regression analysis. Adjusted for HTN, DM medication group.
BMI: body mass index; SBP: systolic blood pressure; DBP:
diastolic blood pressure; LDL: low density lipoprotein cholesterol; hs-CRP: high sensitive C-reactive protein.
*values have been analysised after log-transformation Table 3. Multiple regression analysis to assess indepen-
dent relationships between baPWV and clinical variables
Variable
Mean baPWV
Male Female Total
r P-value R P-value r P-value
Age (y) 0.577 <0.001 0.663 <0.001 0.626 <0.001
BMI (kg/m
2) 0.057 0.58 0.318 0.004 0.225 0.003
WC* (cm) 0.162 0.114 0.346 0.002 0.317 <0.001
SBP (mmHg) 0.597 <0.001 0.775 <0.001 0.69 <0.001
DBP (mmHg) 0.177 0.084 0.723 <0.001 0.261 <0.001
Pulse rate (beat/min) 0.16 0.116 0.163 0.146 0.142 0.59
Fasting glucose (mg/dL) 0.321 <0.001 0.417 <0.001 0.356 <0.001
Fasting insulin* -0.063 0.547 0.013 0.911 0.013 0.869
HOMA-IR 0.089 0.392 0.096 0.409 0.136 0.078
Total cholesterol* (mg/dL) -0.023 0.823 0.315 0.004 0.154 0.04
Triglyceride* (mg/dL) 0.152 0.138 0.326 0.003 0.285 <0.001
HDL (mg/dL) 0.017 0.869 -0.01 0.933 -0.038 0.616
LDL (mg/dL) -0.09 0.382 0.285 0.01 0.108 0.153
hs-CRP* (mg/dL) 0.11 0.292 0.289 0.011 0.225 0.003
Calcium (mg/dL) -0.029 0.776 0.229 0.04 0.115 0.128
25-Hydroxyvitmin D* (ng/dL) 0.175 0.086 0.05 0.658 0.185 0.013
Coefficients (r) and P-values were calculated by the Person’s correlation model.
BMI: body mass index; WC: waist circumference; SBP: systolic blood pressure; DBP: diastolic blood pressure; HOMA-IR:
homeostasis model assessment of insulin resistance; HDL: high density lipoprotein cholesterol; LDL: low density lipoprotein cholesterol; hs-CRP: high sensitive C-reactive protein; baPWV: brachial-ankle pulse wave velocity.
*values have been analysed after log-transformation.
Table 2. Correlation between mean baPWV and cardiovascular related variables
P=0.005), 당뇨(r=0.350, P=0.001), 총콜레스테롤(r=
0.315, P=0.004), 중성지방(r=0.326, P=0.003), 저밀도 지질단백(r=0.285, P=0.01), 고민감도 C-반응단백(r=
0.289, P=0.011), 칼슘(r=0.229, P=0.04) 이 상완-발목 맥파속도와 유의성이 없었다(Table 2).
3. 상완-발목 맥파속도와 비타민 D의 연관성
혈중 비타민 D가 상완-발목 맥파속도에 독립적으
로 영향을 주는지 알아보기 위해 성별, 연령, 체질량
지수, 고혈압 유무, 수축기혈압, 중성지방, 지밀도 지
질단백, 흡연, 혈중 비타민 D, 고민감도 C-반응단백을
독립변수로 하여 다중회귀분석을 시행하였다. 그 결
과 연령(β=7.49, P<0.001), 체질량지수(β=-10.05,
P=0.023), 수축기혈압(β=7.69, P<0.001), 중성지방(β=111.41, P=0.039), 공복혈당(β=1.447, P=0.561)이
상완-발목 맥파속도에 독립적으로 영향을 주는 것으
로 나타났으나 혈중 비타민 D는(β=3.00, P=0.954) 유
의한 상관관계를 보이지 않았다(Table 3).
고 찰
미국의 국립 건강 영양 분석자료(National Health and Nutritional Examination Survey)를 분석한 결과에 의하면, 미국성인의 평균 비타민 D 농도는 10년 사 이에 6 ng/ml이 떨어진 24 ng/ml으로 확인되었다.
10우리나라의 경우 폐경 여성의 대부분이 30 ng/mL 미 만으로 확인되어
11비타민 D 부족은 우리나라뿐 아 니라 전 세계적으로 심각한 문제임을 알 수 있다. 본 연구에서는 20세 이상 성인 남녀를 대상으로 남녀 각각에서 비타민 D를 포함한 다양한 심혈관계 위험 인자와 상완-발목 맥파속도의 연관성을 알아보고자 하였다. PWV와 단순 상관관계를 보이는 인자들은 연령, 체질량지수, 허리둘레, 수축기 혈압, 이완기 혈 압, 공복혈당, 총 콜레스테롤, 중성지방, 고민감도 C- 반응단백, 비타민 D 농도였으며, 다중회귀분석에서 는 연령, 체질량지수, 수축기 혈압, 중성지방, 공복 혈당이 맥파속도에 독립적인 영향을 주는 것으로 밝 혀졌다. 혈중 비타민 D는 독립적인 요인으로서 관계 가 없는 것으로 확인되었다.
맥파속도는 동맥의 경직도를 반영하는 지표로서, 동맥경화의 지표가 될 수 있으며,
20상완-발목 맥파 속도의 측정을 통해 비교적 간단하게 혈압과 맥파속 도를 측정할 수 있게 되었다. 이전의 논문들에서 낮 은 비타민 D와 심혈관계 질환의 위험성과 사망률이 연관된 것으로 보고된바 있다.
19-22맥파속도의 증가 는 연령의 증가, 고혈압, 당뇨병 고지질혈증, 흡연, 비만 등과 관련이 있으며,
23,24최근 연구들에 보면 남 녀 모두에서 대사증후군의 요소를 많이 가질수록 상 완-발목 맥파속도가 높아지는 경향을 보였으며, 상 완-발목 맥파속도는 수축기혈압, 나이, 성별, 체질량 지수 및 공복혈당과 유의하게 연관됨을 보고하였 다.
25본 연구에서는 고지질혈증과 상완-동맥 맥파속 도의 상관관계가 나타나지 않았는데 이는 약물 조 사에 있어 고지혈증 약물복용에 대한 조사가 이루어 지지 않았을 것으로 추측된다. 또한 Ibhar
26, Tarcin
27등의 연구에 의하면 23명의 증상 없는 비타민 D 결 핍의 터키인을 대상으로 한 연구에서 상완-동맥 맥 파속도와 비타민 D는 역의 연관성을 보이는 것으로 확인되었으나 본 연구에서는 연관성을 찾지 못하였
다. 이는 본 연구 대상자의 비타민 D의 평균 농도가 남성 14.4±6.7 (ng/dL), 여성 10.5±8.4 (ng/dL)로 성별 의 평균값이 결핍(deficiency) 상태로 확인되었으며, 적정농도에 해당되는 대상자는 2명(sufficiency), 부 족(insufficiency)인 상태는 21명으로 확인되었다. 이 는 혈중 비타민 D를 측정한 기간이 3~4월이었으며, 상대적으로 햇볕노출이 적은 결과라 생각되며, 위 결과는 일반화하기에는 제한이 있다.
현재까지 국내에서 발표된 연구결과들 중에는 건 강한 사람을 대상으로 혈중 비타민 D 농도와 상완- 발목 맥파속도의 연관성을 본 연구는 없다. 이 연구 는 건강한 사람을 대상으로 혈중 비타민 D 농도와 상완-발목 맥파속도의 연관성을 봄으로써, 비타민 D 가 동맥의 경직도에 영향을 미치는 인자로 작용하는 지 알아보고자 하였다. 그러나 이연구의 대상자 역 시 일개 검진 센터를 방문한 특정 성인만은 대상으 로 하였기 때문에 대상자 선별에 있어 선택 치우침 이 작용하였을 가능성이 있다. 또한 단면연구로 진 행되었기 때문에 비타민 D와 동맥의 경직도와의 인 과관계도 알 수 없다. 또한 음주와 흡연에 있어 양에 대한 접근이 이루어지지 않아 음주와 흡연이 상완- 발목 맥파속도와의 연관성에 대해서 밝히지 못하는 것도 제한점이라 할 수 있다. 이에 따라 혈중 비타민 D 농도가 심혈관 질환 이환율이나 사망률에 어떤 영향을 미치는지, 비타민 D 결핍이 있는 대상자에게 햇볕 노출이나 비타민 D 복용 등의 중재가 동맥의 경직도나 심혈관 질환의 이환율이나 사망률에 어떤 효과가 있는지 알아보기 위한 추가 연구가 필요할 것이다.
참 고 문 헌