허혈시신경병
박지윤
서남대학교 전주예수병원 신경과
Ischemic Optic Neuropathy
Ji-Yun Park, MD
Department of Neurology, University of Seonam College of Medicine, Presbyterian Medical Center, Jeonju, Korea
Ischemic optic neuropathy may be classified into two types: anterior ischemic optic neuropathy (AION) presenting pale edema of the optic disc and posterior ischemic optic neuropathy (PION) manifesting no remarkable changes on the optic disc during the acute stage. AION results from ischemic damage to the anterior portion of the optic nerve, which is primarily supplied by the poste- rior ciliary artery circulation. AION is generally divided into two types: arteritic AION (AAION), resulting from ischemia secondary to vasculitis (usually from giant cell arteritis, GCA), and non arteritic AION (NAION), resulting from noninflammatory small-vessel infarc- tion of anterior optic nerve. PION is much less common than AION and also is divided into arteritic and nonarteritic conditions. PION generally occurs in either the perioperative setting or in the setting of GCA or other vasculitides and should be differentiated from any retrobular optic nerve pathology including compressive, inflammatory, and infiltrative optic neuropathies. While the manage- ment of arteritic ischemic optic neuropathy is relatively straight forward with steroids, various therapeutic trials for nonarteritic type has been applied but not established yet.
Keywords: ISchemic optic neuropathy; Optic nerve disease; Giant cell arteritis
서 론
허헐시신경병은 시신경염과 더불어 성인에서 신경성 시력상실의 가장 흔한 원인 중 하나이다. 두 질환은 치료방침과 예후가 달라 임상 적으로 두 질환을 감별하는 것은 중요하기 때문에 임상적인 특징을 숙지하고 있어야 한다(Table 1). 허혈시신경병증은 거대세포동맥염 (gaint cell arteritis, GCA)을 제외하면 대부분 급성으로 통증 없이 발 생하여 일측의 시신경을 침범하고 색각(color vision)이 보존되는 것이 특징이다. 허혈시신경병은 시신경유두의 부종에 따라 앞허혈시신경 병(anterior ischemic optic neuropathy, AION)과 뒤허혈시신경병(pos- terior ischemic optic neuropathy, PION)으로 나뉘며, 발생원인에 따라 동맥염성(arteritic)과 비동맥염성(non-arteritic)으로 다시 세분된다. 본
고에서는 안구의 혈류공급에 대한 해부학적 지식 및 허혈시신경병을 분류하여 살펴보고자 한다.
시신경의 혈관분포
눈동맥(ophthalmic artery)은 내경동맥(internal carotid artery)의 경 막내분지(intradural branch) 중 가장 먼저 분리되어 앞으로 진행한 후 시신경관(optic canal)으로 들어와 시신경의 아래에 분포한다(Fig. 1).
1눈동맥은 눈확내부위(intraobitalportion)에서 시신경과 교차하며 망 막중심동맥(central retinal artery, CRA)과 외측후섬모체동맥(lateral posterior ciliary artery)으로 분지하고 이 후 눈물샘동맥(lacrimal ar- tery), 내측후섬모체동맥(medial posterior ciliary artery), 후벌집동맥
Correspondence to: Ji-Yun Park, MD
Department of Neurology, Presbyterian Medical Center, 365 Seowon-ro, Wansan-gu, Jeonju 560-750, Korea Tel: +82-63-230-1572, Fax: +82-63-230-1578, E-mail: [email protected]
Received: Sep. 26, 2014 / Accepted: Oct. 13, 2014
REVIEW
(posterior ethmoid artery), 눈확위동맥(supraorbital artery), 앞벌집동 맥(anterior ethmoid artery), 내측눈꺼풀동맥(medial palpebral artery) 으로 분지된 후 앞으로 진행하여 등쪽코분지(dorsal nasal branch)와 도르래위동맥(supratrochlear artery)으로 나뉘게 된다. 시신경과의 교
차는 80%가 신경아래에서 20%가 신경의 윗부분에서 이루어지고, CRA는 신경집(nerve sheath)을 뚫고 지주막하공간(subarachnoid space)에서 1-3 mm 정도 진행한 후 시신경으로 들어가 시신경의 중앙 으로 진행하여 시신경유두에서 위측두쪽(superior temporal), 위코쪽
Table 1. Clinical characteristics of common optic neuropathies
Optic neuritis NAION AAION K-PION K-Heredity Papilledema
Age Younger 60 (mean) 70 (mean) Any age Younger Any age
Laterality Unilateral Unilateral Uni or bilateral Uni or bilateral Bilateral Bilateral
Visual loss Rapidly progressive Acute, up to 61%> 20/200 Acute, up to 76%< 20/200 Acute Subacute (LHON);
progressive (DOA) Acuity preserved until late
Pain Orbital pain frequent
with eye movement Infrequent Headache, scalp tender
ness, jaw claudication Infrequent Absent Headache (raised ICP)
Color vision Abnormal Variably spared Variably spared Variably spared Abnormal Preserved until late
Visual field Central defect Altitudinal defect (inferior) Altitudinal defect Altitudinal defect Cecocentral scotoma Peripheral constriction Optic disc (acute) Normal or disc edema Disc edema +/- small
cup-to-disc ratio Chalky-white optic disc
swelling Normal disc Pseudoedema in LHON Disk edema
(late) Temporal pallor Segmental pallor Pallor Pallor Pallor Pale swelling
Visual prognosis Good Improvement in up to 43%,
fellow eye in < 30% Improvement rare, fellow
eye in up to 95% Improvement up to 34%,
fellow eye in 50-55% Poor Reversible if treated early
Systemic disease Risk of multiple sclerosis Vascular risk factors: DM,
HTN GCA, elevated ESR,CRP Vascular risk factor, GCA Mitochondrial disease,
DIDMOAD syndrome Any cause of raised ICP
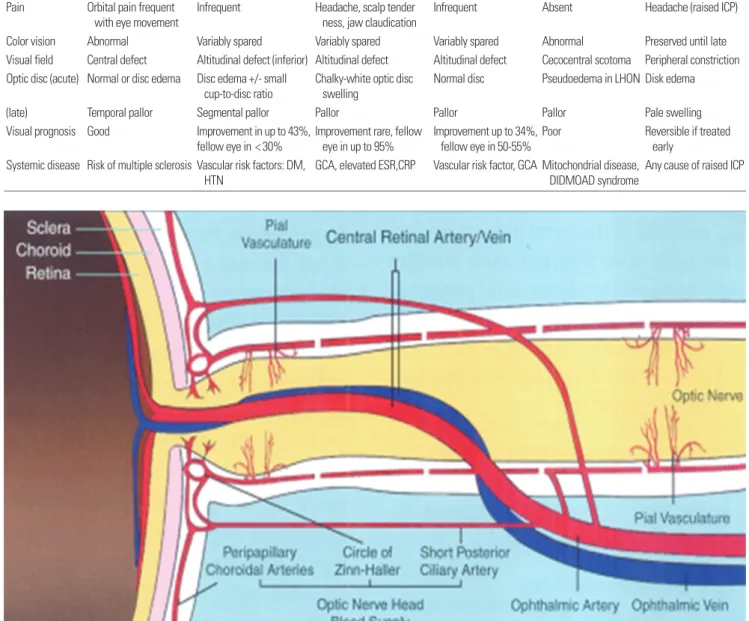
Fig. 1. Schematic drawings of the blood supply of the optic nerve. The ophthalmic artery provides major blood supply to the optic nerve. In the optic canal, the oph- thalmic artery gives rise to the pial vasculature and pierces the optic nerve sheath becoming the central retinal artery. The central retinal artery does not contribute di- rectly to the circulation of the optic nerve head. Instead, the major blood flow to the optic nerve head is derived from short posterior ciliary arteries, peripapillarycho- roidal arteries and circle of Zinn-Haller. The short posterior ciliary arteries send branches to the circle of Zinn-Haller, peripapillarychoroidal arteries, and the pial vascu- lature. The central retinal vein parallels the course of the central retinal artery (Reproduced from Saden AA., Wang MY., 2011).
(superior nasal), 아래측두쪽(inferior temporal), 아래코쪽(inferior na- sal) 등 네 개의 분지를 낸다. 후섬모체동맥은 다양하게 분포하는데 주 로 2-3개 정도 주요 분지를 낸 후 다시 여러 개의 분지로 나뉜 후 공막 (sclera)을 뚫고 시신경주위에서 진씨고리(circle of Zinn-Haller)라는 연 결고리(anastomotic ring)를 형성하는 짧은후섬모체동맥(short poste- rior ciliary artery)과 공막내에 서안와의 내부구조들의 혈류를 공급하 는 긴후섬모체동맥(long posterior ciliary artery)으로 나뉘게 된다. 시 신경유두는 CRA에 의해서 직접적으로 혈액공급을 받는 것이 아니라 짧은후섬모체동맥에 의해 형성되는 진씨고리에 의해 혈액을 공급 받 는다. 정상적으로 안저검사상시신경유두 주위에서 4개의 CRA분지 가 관찰되고, 50%에서는 짧은 섬모체동맥에서 분지된 섬모체막망동 맥(cilioretinal artery)이 관찰되기도 한다.
비동맥염성앞허혈시신경병(Nonarteritic Anterior Ischemic Optic Neuropathy, NAION)
NAION은 50대 이후 발생하는 시신경병증의 가장 흔한 원인이다.
남녀의 차이는 없고, 발생 평균연령은 57-67세로 고령에 많이 분포되 어 있으나 11세에서 90세까지 다양한 연령에서 발생할 수 있으므로 주의가 필요하다.
2-4대부분 통증 없이 급격한 시력저하를 호소하고 10% 정도에서 안구 주위의 둔통을 호소하나 전형적인 시신경염에서 호소하는 눈을 움직일 때 발생하는 통증과는 구분된다.
3또한 isch- emic optic neuropathy decompression trial research group (IONDT)에 따르면 42%는 기상 후 2시간 이내, 42%는 오후에 발생한다고 알려져 있어 특정시간과의 연관성은 적다. 고혈압과 당뇨병이 NAION의 위험 인자로 잘 알려져 있으나 흡연, 고지혈증, 과트리글리세라이드혈증 (hypertriglyceridemia), 고호모시스틴혈증(hyperhomocysteinemia), 야간저혈압(nocturnal hypotension), 백내장 수술 등도 위험인자로 알 려져 있다. 백인종은 흑인종이나 라틴계에 비해 NAION의 빈도가 높
은 것으로 알려져 있으며 이는 시신경이 눈으로 빠져 나오는 공막입 구(scleral opening)가 작아(작은 cup-to-disc ratio), 즉 시신경의 밀도가 높아 시신경이 쉽게 손상받기 때문으로 추측된다. NAION의 색각이 상은 상대적으로 심한 시신경염과 달리 시력소실과 비례하여 손상되 므로 비교적 색각기능이 보존되어 있다.
555-80%에서 특징적인 수평 반맹(altitudinal field defect)이 보고되고 있으며 특히 아래쪽이 더 많 다고 알려져 있으나 시신경이상과 관련된 어떤 시야결손에서도 같은 양상으로 발생할 수 있다.
6급성기안저검사에서는 유두부종(disc ede- ma), 유두주위 화염상망막출혈(peripapillary flame-shaped retinal hemorrhage)이 관찰될 수 있으며 4-6주 후에는 이차적 시신경 위축을 동반한 광범위 혹은 부분적 창백(diffuse or segmental pallor with sec- ondary atrophy)이 관찰될 수 있다(Fig. 2). NAION은 AAION보다 시력 소실이 심하지 않아 58-66%에서 0.1 이상으로 시력이 유지되고 대부 분 시력악화가 진행하지 않는다. 특별한 치료를 하지 않아도 시력은 41%에서, 시야는 25%에서 6개월까지 회복을 기대할 수 있으나 그 이 후에는 더 이상의 호전을 기대하기 어렵다.
7아직까지 NAION의 확립 된 치료는 없으나 시도되었던 치료들은 다음과 같다.
3,8이전에 시신경 초감압술(optic nerve sheath decompression)이 시신경 주위의 조직을 느슨하게 하여 압력을 줄여줌으로써 시력을 호전시킨다는 주장이 있 었으나,
9최근에는 시신경초감압술이 효과적이지 않을 뿐 아니라 위 험할 수 있다고 알려져 있다.
10증상발생 2주 이내 심한 시각소실(시력 20/70 이하, 초기에 심한 시야장애)을 보이는 경우 2주간 prednisolone 80 mg 경구 치료를 통해 6개월, 12개월 후 시력, 시야를 호전시킨다는 보고가 있다.
7이는 급성기 스테로이드 치료가 유두부종을 감소시켜 시신경 앞쪽(optic nerve head)의 모세혈관의 혈액순환을 호전시키기 때문이라고 추측하고 있으나 아직까지 무작위 통제된 연구결과가 없 고 스테로이드의 부작용을 고려해야 하므로 효과를 판단하기 어렵 다. 반면에 아스피린 경구투여는 NAION 발생 이후 시력의 회복에 영 향을 미치지 못한다고 알려져 있으나,
11정상눈의 NAION 발생을 예
A B C
Fig. 2. Fundus photographs and Goldman visual field (GVF) of the nonarteritic anterior ischemic optic neuropathy (NAAION). (A) The hyperemetic disc edema is more prominent superiorly. Focal surface telangiectasia of disc vessels is seen superotemporally (arrows). (B) The disc, 2 months after onset, is segmentally atrophic superi- orly (arrows), with sparing and resolving edema inferiorly. (C) GVF shows inferior altitudinal visual field defect (Reproduced from Arnold AC.,2009).45
방하기 위해 고려해 볼 수 있다.
12431명의 NAION 환자의 후향적코호 트 연구 결과 2년 후 정상눈의 NAION 발생을 효과적으로 감소시켰 으나, 5년 후는 큰 차이 없는 결과를 보였는데
12향후 효과적인 예방법 을 찾기 위한 연구가 필요하다. 최근 동물실험에서 신경보호 효과를 가지고 있는 topialbrimonidine이 효과가 있다고 알려졌으나,
13임상시 험에서 0.2% brimonidine tartrate가 효과가 없는 것으로 밝혀졌다.
14,15그 외에 bevacizumab유리체강내 주입이 신생혈관생성을 억제하여 부종을 호전시켜 효과가 있다는 연구가 있으나 아직까지 치료가 확립 되지 못했다.
16그 외 항응고제,
17diphenylhydantoin,
18레보도파(le- vodopa),
19노르에피네프린 정맥주입,
20,21헤파린유발저밀도지단백/섬 유소원 침전 혹은 혈액희석(heparin-induced low-density lipoprotein/
fibrinogen precipitation or hemodilution)
22등이 시도되었으나 뚜렷한 효과를 입증하지 못했다. 결론적으로 NAION의 확립된 치료는 없지 만, 급성기 심한 시각소실과 심한 유두부종이 관찰된다면 경구 스테 로이드 치료를 고려해 볼 수 있고, 장기적으로 정상측 눈에 재발을 방 지하기 위해 항혈소판제의 복용을 고려하고, 혈관위험인자를 조절하 는 것이 무엇보다 중요하다.
동맥염성허혈시신경병(Arteritic Anterior Ischemic Optic Neuropathy, AAION)
AAION의 대부분의 원인인 거대세포동맥염(gaint cell arteritis, GCA)은 50대 이상에서 새롭게 발생하거나 두통의 양상이 바뀌었을 때 의심해야 하며 특징적으로 적혈구 침강속도(erythrocyte sedimen- tation rate, ESR)와 C반응단백(C-reactive protein, CRP) 수치가 크게 증 가되어 있다. 50세 이후에 연령이 증가하면서 발생 빈도도 현저히 증 가하여 60대에 비해 70대에서 약 9배, 90대에서 22배나 증가한다.
GCA는 백인종에서 흔하게 발생하나, 아프리카계 아메리카인(Africa- American)과 라틴계, 아시안에서는 드물다고 알려져 있다. ICHD-II의 진단기준은 Table 2와 같으며 가장 흔한 증상인 두통은 70% 이상에서
동반되고 그 외 전신증상으로 이마관자부위 통증, 체중감소, 몸살, 식 은땀 등이 동반되거나 씹거나 턱을 많이 움직일 때 허혈로 인한 통증 이 유발되는 턱파행(jaw claudication) 및 시신경에 혈액을 공급하는 혈관들이 침범되어 시력소실이 발생할 수 있다. 시력소실은 대부분 처음에 일측으로 발생하지만, 치료하지 않으면 수일 내에 30%까지 양 측으로 발생할 수 있으므로 빠른 진단과 치료가 중요하다.
23영구적인 시력소실은 일시적인 시력소실이나 턱파행의기왕력이 있는 경우 증 가하고 간기능수치의 상승이나 열, 체중감소 등 전신증상이 있는 경 우 감소한다.
24-26AAION은 안저검사에서 백묵같이 흰 유두부종(chalky-white optic disc swelling), 양측침범, 면모반(cotton-wool spots)이나 망막경색(reti- nal infarction) 같은 동반된 망막 혹은 맥락막 동맥 허혈(concurrent signs of retinal or choroidal circulation ischemia) 등이 관찰될 수 있다 (Fig. 3). 잘 알려진 대로 대부분의 GCA에서 ESR의 상승이 관찰된다.
ESR의 정상범위를 정확히 알 수 없으나 일반적으로 남성의 경우 나이 를 절반으로 나눈 값을, 여성의 경우 나이에 10을 더한 후 절반으로 나 눈 값을 최대 정상범위로 정하여 사용하고 있다.
27생검으로 진단된 GCA의 8%에서 22%까지 ESR이 정상범위일 수 있으므로 ESR이 정상 범위이더라도 강력히 GCA가 의심된다면 관자동맥생검을 시행해야
한다.
28,29CRP의 민감도는 ESR (민감도 92%)에 비해 높아 100%까지 보
고되기도 한다.
30또한 급성기에 ESR보다 빠르게 상승하고 효과적인 치료에 빠르게 감소하므로 임상에서 유용하게 사용될 수 있다.
30이
Fig. 3. Fundus photograph of the arteritic anterior ischemic optic neuropathy (AAION). The optic disc demonstrates diffuse chalky white optic disc edema during the initial stages (Reproduced from Hayreh et al., 2009).46
Table 2. Gaint cell arteritis – International Headache Society Diagnostic criteria Headache attributed to giant cell arteritis
A. Any new persisting headache fulfilling criteria C and D B. At least one of the following
1. Swollen tender scalp artery with elevated erythrocyte sedimentation rate (ESR) and/or C reactive protein (CRP)
2. Temporal artery biopsy demonstration giant cell arteritis
C. Headache develops in close temporal relation to other symptoms and signs of giant cell arteritis
D. Headache resolves or greatly improve within 3 days of high-dose steroid treatment
ICHD_II. Cephalagia 2004;24(Supp 1).
외에 혈소판증가나 interleukin-6 의 상승이 관찰될 수 있다.
GCA의 확진을 위해 얕은관자동맥(superficial temporal artery)의 생검이 필요한데 생검 시 짧은 길이를 체취하면 비연속적으로 동맥염 이 침범(skip lesion)되어 있을 경우 위음성(false negative)으로 나올 수 있으므로 최소한 3 cm 이상을 채취하여야 한다.
31GCA의 전형적인 병 리학적 소견은 혈관내막의 비후(intimal thickening), 내탄력판의 분절 (fragmentation of the internal elastic lamina), 다수의 다핵 거대세포 (macrophages in the elastic lamina)가 있는 육아종성 염증이다.
32,33GCA가 강력히 의심되는데 관자동맥생검에서 위음성이 나오는 경우 반대편 관자동맥 생검을 시도하거나, 경험이 많은 병리학자에게 재의 뢰하는 것을 고려할 수 있다. 반드시 필요한 검사는 아니지만 색도플 러영상(color doppler imaging)은 혈류의 이상, 혈관벽의 부종 등을 관 찰하여 생검부위를 확인할 때,
34MRI, MRA는 시신경의 조영증강, 얕 은관자동맥 주변 조영증강이나 협착 등을 관찰하기 위해 유용하게
사용될 수 있다.
35-37조기 스테로이드 치료가 대부분 환자의 시력소실을 막는 데 효과 적이므로 GCA가 의심되는 경우 고용량의 스테로이드치료가 되도록 빨리 시작되어야 한다.
38스테로이드 치료 후 최소 2주 동안 GCA의 병 리학적 소견이 지속적으로 관찰되므로 생검을 위해 치료를 미루어서 는 안 된다.
39,40Prednisolone 1 g/day 정맥투여를 3-5일간 유지한 후 고 용량의 경구 prednisolone 1-2 mg/kg/day 치료를 최소 4주 이상 유지해 야 하며 증상의 소실, ESR, CRP의 감소를 고려하여 치료 기간을 결정 한다. 스테로이드의 장기간 사용이 골다공증, 당뇨병, 쿠싱증후군 등 부작용을 일으킬 수 있으므로 이에 대한 주의가 필요하다. 최근에는 스테로이드의 용량을 줄이기 위해 혹은 스테로이드 저항성 GCA인 경우 cyclophosphamide, dapsone, methotrexate, azathioprine, inflix- imab, 저용량 aspirin의 단독 혹은 추가적 치료를 고려할 수 있다.
8GCA는 안전수지(count finger) 이하의 시력소실이 54%정도로 26% 정
A B
C D
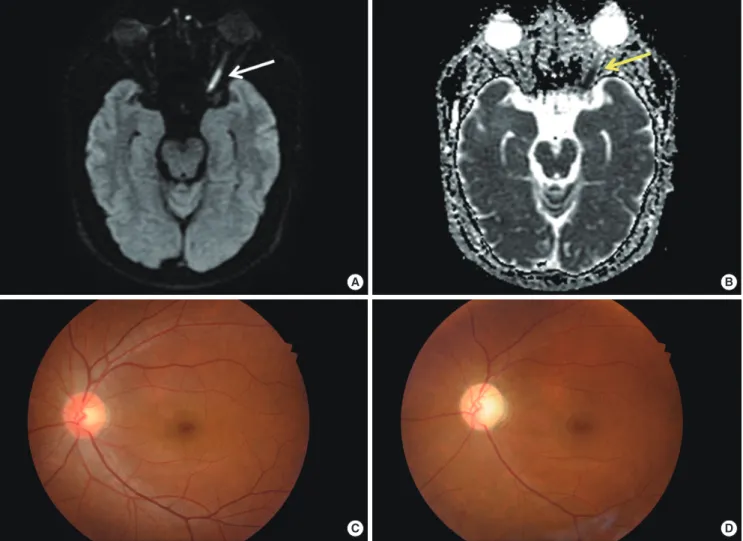
Fig. 4. Diffusion weighted MRI (A), apparent diffusion coefficient (ADC, B) and fundus views (C, D) of the posterior ischemic optic neuropathy (PION). Diffusion weight- ed MRI of orbit (A) can reveal abnormal hyperintensity in left optic nerve (white arrow) with the reduced ADC (B, yellow arrow). The optic disc in PION (C) appeared normal in acute stage, but the optic disc becomes pale after 2 months.
도인 NAION에 비해 심한 시력소실이 관찰된다.
23또한 적절한 치료에 도 불구하고 시력의 회복은 15% 정도밖에 되지 않는다. 그러나 증상 발생 24시간 이내 치료를 시작하는 경우 58%까지 시력회복을 기대할 수 있으므로 무엇보다 조기 스테로이드 치료가 중요하다.
뒤허혈시신경병(PION)
PION은 시신경유두의 부종을 동반하지 않고 갑자기 발생한 시신 경병증의 경우 의심해 볼 수 있으나 압박시신경병증, 침윤시신경병증, 유전시신경병증, 독성시신경병증, 외상시신경병증 등을 먼저 배제해 야 한다. 초기안저검사는 정상소견을 보이나 후에 시신경위축(optic atrophy)이 발생할 수 있다. PION은 수술 후 혈류 공급이 저하되거나 거대세포염을 포함한 혈관성 질환 등에 의해 발생할 수 있으므로 PION이 의심된다면 이에 대한 검사가 필요하다.
41PION에서 뇌 MRI 는 다른 질환을 배제하기 위해 시행하는데, 때때로 확산강조영상MRI 에서 시신경의 이상소견이 관찰되기도 한다(Fig. 4).
42GCA가 원인인 경우를 제외하고 PION의 정립된 치료는 아직까지 없으며 빈혈, 저혈 압 등 위험인자를 빨리 확인하여 교정시키는 것이 중요하다.
결 론
허혈시신경병은 원인에 따라 치료 및 예후가 다르고 때로는 응급 을 요하므로 빠르고 정확하게 원인을 찾고자 노력해야 한다. NAION 는 약반이상에서 0.1 이상의 시력을 유지하고 있으며 6개월 내 시력회 복을 기대해 볼 수 있다. 또한, 동측 눈의 재발은 적으나 정상 눈의 재 발이 발생할 수 있으므로 혈관위험인자를 조절해야 한다. GCA는 발 생빈도가 드물지만 심각한 시력저하를 초래하고 조기에 치료하지 않 으면 수일 내에 정상 눈을 침범할 수 있으므로 의심된다면 빠른 시간 내에고용량의 스테로이드 치료를 시작해야 한다. CRAO는 대부분 심 각한 실명에 이르지만 급성기동맥내혈전용해술로 시력회복을 기대 해 볼 수 있으므로 숙련된 중재시술팀이 있다면 시술을 고려해 보아 야 한다.
REFERENCES
1. Hayreh SS. Acute retinal arterial occlusive disorders. Prog Retin Eye Res 2011;30:359-394.
2. Boghen DR, Glaser JS. Ischaemic optic neuropathy. The clinical profile and history. Brain 1975;98:689-708.
3. Characteristics of patients with nonarteritic anterior ischemic optic neu- ropathy eligible for the Ischemic Optic Neuropathy Decompression Trial.
Arch Ophthalmol 1996;114:1366-1374.
4. Preechawat P, Bruce BB, Newman NJ, Biousse V. Anterior ischemic optic
neuropathy in patients younger than 50 years. Am J Ophthalmol 2007;
144:953-960.
5. Repka MX, Savino PJ, Schatz NJ, Sergott RC. Clinical profile and long- term implications of anterior ischemic optic neuropathy. Am J Ophthal-
mol 1983;96:478-483.
6. Hayreh SS, Zimmerman B. Visual field abnormalities in nonarteritic an- terior ischemic optic neuropathy: their pattern and prevalence at initial examination. Arch Ophthalmol 2005;123:1554-1562.
7. Hayreh SS, Zimmerman MB. Non-arteritic anterior ischemic optic neu- ropathy: role of systemic corticosteroid therapy. Graefes Arch Clin Exp
Ophthalmol 2008;246:1029-1046.
8. Hayreh SS. Management of ischemic optic neuropathies. Indian J Oph-
thalmol 2011;59:123-136.
9. Sergott RC, Cohen MS, Bosley TM, Savino PJ. Optic nerve decompres- sion may improve the progressive form of nonarteritic ischemic optic neuropathy. Arch Ophthalmol 1989;107:1743-1754.
10. Optic nerve decompression surgery for nonarteritic anterior ischemic op- tic neuropathy (NAION) is not effective and may be harmful. The Isch- emic Optic Neuropathy Decompression Trial Research Group. JAMA 1995;273:625-632.
11. Botelho PJ, Johnson LN, Arnold AC. The effect of aspirin on the visual outcome of nonarteritic anterior ischemic optic neuropathy. Am J Oph-
thalmol 1996;121:450-451.
12. Beck RW, Hayreh SS, Podhajsky PA, Tan ES, Moke PS. Aspirin therapy in nonarteritic anterior ischemic optic neuropathy. Am J Ophthalmol 1997;
123:212-217.
13. Danylkova NO, Alcala SR, Pomeranz HD, McLoon LK. Neuroprotective effects of brimonidine treatment in a rodent model of ischemic optic neu- ropathy. Exp Eye Res 2007;84:293-301.
14. Wilhelm B, Ludtke H, Wilhelm H. Efficacy and tolerability of 0.2% brimo- nidine tartrate for the treatment of acute non-arteritic anterior ischemic optic neuropathy (NAION): a 3-month, double-masked, randomised, pla- cebo-controlled trial. Graefes Arch Clin Exp Ophthalmol 2006;244:551-558.
15. Saylor M, McLoon LK, Harrison AR, Lee MS. Experimental and clinical evidence for brimonidine as an optic nerve and retinal neuroprotective agent: an evidence-based review. Arch Ophthalmol 2009;127:402-406.
16. Huang JY, Ozaki H, Hayashi H, Uchio E. Anterior ischemic optic neu- ropathy following intravitreal bevacizumab. Jpn J Ophthalmol 2010;54:
252-254.
17. Saraux H, Murat JP. Pseudopapillitis of vascular origin. Ann Ocul (Paris) 1967;200:1-19.
18. Keltner JL, Becker B, Gay AJ, Podos SM. Effect of diphenylhydantoin in ischemic optic neuritis. Trans Am Ophthalmol Soc 1972;70:113-130.
19. Johnson LN, Gould TJ, Krohel GB. Effect of levodopa and carbidopa on recovery of visual function in patients with nonarteritic anterior ischemic optic neuropathy of longer than six months’ duration. Am J Ophthalmol 1996;121:77-83.
20. Smith JL. Norepinephrine therapy of ischemic optic neuropathy. J Clin
Neuroophthalmol 1981;1:289-290.
21. Kollarits CR, McCarthy RW, Corrie WS, Swann ER. Norepinephrine therapy of ischemic optic neuropathy. J Clin Neuroophthalmol 1981;1:
283-288.
22. Haas A, Walzl M, Jesenik F, Walzl B, Berghold A, Bergloff J, et al. Applica- tion of HELP in nonarteritic anterior ischemic optic neuropathy: a pro- spective, randomized, controlled study. Graefes Arch Clin Exp Ophthalmol 1997;235:14-19.
23. Hayreh SS, Podhajsky PA, Zimmerman B. Occult giant cell arteritis: ocu- lar manifestations. Am J Ophthalmol 1998;125:521-526.
24. Gonzalez-Gay MA, Lopez-Diaz MJ, Barros S, Garcia-Porrua C, Sanchez-
Andrade A, Paz-Carreira J, et al. Giant cell arteritis: laboratory tests at the time of diagnosis in a series of 240 patients. Medicine (Baltimore) 2005;
84:277-290.
25. Gonzalez-Gay MA, Garcia-Porrua C, Miranda-Filloy JA. Giant cell arte- ritis: diagnosis and therapeutic management. Curr Rheumatol Rep 2006;
8:299-302.
26. Gonzalez-Gay MA, Barros S, Lopez-Diaz MJ, Garcia-Porrua C, Sanchez- Andrade A, Llorca J. Giant cell arteritis: disease patterns of clinical presen- tation in a series of 240 patients. Medicine (Baltimore) 2005;84:269-276.
27. Miller A, Green M, Robinson D. Simple rule for calculating normal erythrocyte sedimentation rate. Br Med J (Clin Res Ed) 1983;286:266.
28. Jundt JW, Mock D. Temporal arteritis with normal erythrocyte sedimen- tation rates presenting as occipital neuralgia. Arthritis Rheum 1991;34:
217-219.
29. Salvarani C, Hunder GG. Giant cell arteritis with low erythrocyte sedi- mentation rate: frequency of occurence in a population-based study. Ar-
thritis Rheum 2001;45:140-145.
30. Hayreh SS, Podhajsky PA, Raman R, Zimmerman B. Giant cell arteritis:
validity and reliability of various diagnostic criteria. Am J Ophthalmol 1997;123:285-296.
31. Lui GT, Volpe NJ, Galetta SL.Neuroophthalmology: diagnosis and man- agement. Philadelphia: Saunder; 2001.
32. Rentsch JL, Liedel JL, Bayley NB, Buchanan MR, Goldblatt JC, Warren RJ, et al. Giant cell arteritis (GCA) presenting with severe aortic regurgi- tation and a normal ESR. Aust N Z J Med 1998;28:70-71.
33. Ghanchi FD, Dutton GN. Current concepts in giant cell (temporal) arte- ritis. Surv Ophthalmol 1997;42:99-123.
34. Salvarani C, Silingardi M, Ghirarduzzi A, Lo Scocco G, Macchioni P, Ba- jocchi G, et al. Is duplex ultrasonography useful for the diagnosis of gi- ant-cell arteritis? Ann Intern Med 2002;137:232-238.
35. Morgenstern KE, Ellis BD, Schochet SS, Linberg JV. Bilateral optic nerve sheath enhancement from giant cell arteritis. J Rheumatol 2003;30:625-627.
36. Mitomo T, Funyu T, Takahashi Y, Murakami K, Koyama K, Kamio K.
Giant cell arteritis and magnetic resonance angiography. Arthritis Rheum 1998;41:1702.
37. Stanson AW. Imaging findings in extracranial (giant cell) temporal arte- ritis. Clin Exp Rheumatol 2000;18:S43-48.
38. Hayreh SS, Zimmerman B. Visual deterioration in giant cell arteritis pa- tients while on high doses of corticosteroid therapy. Ophthalmology 2003;
110:1204-1215.
39. Melson MR, Weyand CM, Newman NJ, Biousse V. The diagnosis of giant cell arteritis. Rev Neurol Dis 2007;4:128-142.
40. Guevara RA, Newman NJ, Grossniklaus HE. Positive temporal artery bi- opsy 6 months after prednisone treatment. Arch Ophthalmol 1998;116:
1252-1253.
41. Newman NJ. Perioperative visual loss after nonocular surgeries. Am J Oph-
thalmol 2008;145:604-610.
42. Verma A, Jain KK, Mohan S, Phadke RV. Diffusion-weighted MR imag- ing in posterior ischemic optic neuropathy. AJNR Am J Neuroradiol 2007;
28:1839-1840.