Klippel-Trenaunay-Weber syndrome (KTWS) is a rare congenital disorder characterized by cutaneous heman- giomas, hypertrophy of bone and soft tissue, varicose veins, and clinically significant arteriovenous malforma- tion (AVM) (1, 2, 3). AVMs associated with KTWS are lo- cated in the extremities, visceral organs, or spinal canal (1, 3). Most AVMs in the extremities are intramuscular or cutaneous. There is a paucity of data on AVMs in the suprapatellar fat pad associated with KTWS. We report imaging findings of a case with AVM in the suprapatel- lar fat pad of the right knee associated with KTWS.
Case Report
A 25-year-old man presented with a three-month-long
history of painful swelling in the right knee. There was knee joint swelling but change in skin color or bruising.
Aspirated fluid from the knee joint was bloody. There was no specific family history of congenital disease.
Physical examination revealed a brown spot on the right leg, which was apparent at birth, and a cutaneous he- mangioma in the right shin and ankle.
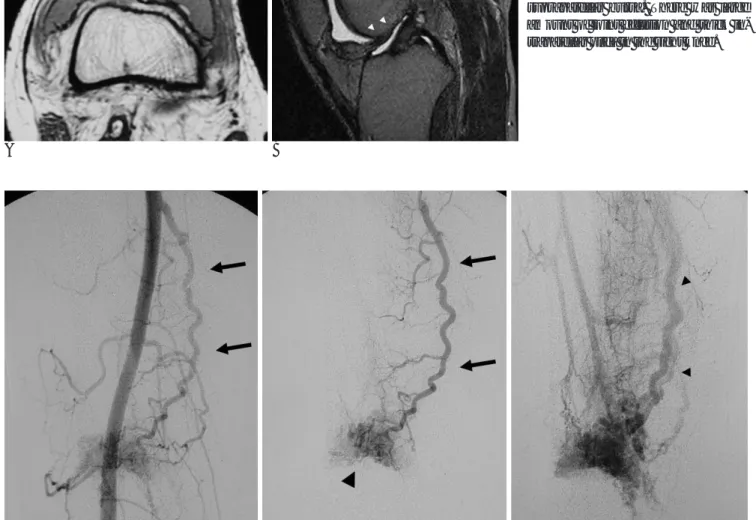
The right leg was slightly longer than the left on physi- cal examination and the plain radiograph of lower ex- tremity (Fig. 1). The right iliac and femoral artery was al- so greater in diameter than the left on femoral arteri- ogram (Fig. 2). A lower extremity venogram showed di- lated and tortuous superficial varicose veins in the right ankle and leg (Fig. 3). There was no thrombosis in the venous system based on both venography and ultra- sonography. A venous Doppler sonogram showed se- vere venous reflux in the right superficial femoral vein, as well as a popliteal vein due to valvular incompetence.
There were multiple dilated tortuous vascular chan- nels in the supra-patellar fat pad on gray-scale and color Doppler sonograms (Fig. 4). We obtained an arterial Doppler spectral waveform within a vessel with spectral
An Arteriovenous Malformation in the Suprapatellar Fat Pad of the Knee associated with Klippel-Trenaunay-
Weber Syndrome: A Case Report1
Mi Hyun Park, M.D., Soon Tae Kwon, M.D., Byung Seok Shin, M.D., Young Mo Kim, M.D.2
1Department of Diagnostic Radiology, Chungnam National University Hospital
2Department of Orthopedic Sugery, Chungnam National University Hospital
Received July 11, 2005 ; Accepted September 7, 2005
Address reprint requests to : Soon Tae Kwon, M.D., Department of Diagnostic Radiology, Chungnam National University Hospital, 640, Daesa-dong, Jung-gu, Taejon 301-040, Korea.
Tel. 82-42-220-7333. Fax. 82-42-253-0061
Klippel-Trenaunay-Weber syndrome (KTWS) is a vascular disorder that has signifi- cant arteriovenous malformation (AVM). We report a case of an AVM in the suprap- atellar fat pad of the knee in a patient with the characteristic manifestations of KTWS, including cutaneous hemangioma, limb hypertrophy, and varicose veins. Magnetic resonance imaging, color Doppler sonography, and subsequent angiography demon- strated an AVM in the supra-patellar fat pad of the right knee causing painful swelling of the knee.
Index words :Extremity, arteriovenous malformation Arteriovenous malformation, MR Arteriovenous malformation Angiography
analysis.
MR imaging showed numerous signal voids in the supra-patellar fat pad, in axial T1, sagittal proton densi- ty, and T2 weighted spin-echo images (Fig. 5). MR imag- ing also demonstrated large amounts of joint effusion and thick intrapatellar plica (Fig. 5).
A selective femoral arteriogram showed a dilated tor- tuous feeding artery and early enhancement of an en- larged draining vein and nidus, indicating AVM (Fig. 6).
Discussion
Klippel-Trenaunay syndrome is characterized by cuta- neous hemangiomas, hypertrophy of bone and soft tis- sue, and varicose veins. When a clinically significant AVM is noted in addition to this triad, the syndrome is termed Klippel-Trenaunay- Weber syndrome (1-3).
Klippel-Trenaunay syndrome is usually unilateral and
most frequently affects the lower extremities, but can affect the upper limb, trunk, and head (2, 4).
The cause of KTWS is still not clear. One hypothesis proposed an intrauterine insult during vascular differen- tiation, with subsequent invasion of the developing limb bud, and other proposed a congenital mesodermal ab-
Fig. 1. Plain anterior posterior radiograph of the leg shows that the right leg is longer than the left.
A B
Fig. 2. Femoral arteriogram showing greater diameter of the right iliac (A) and femoral artery (B) than the left.
Fig. 3. Venogram in the distal leg shows diffuse dilatation of the deep venous system, including distal tibial vein.
Note.- varicosity of the distal posterior tibial vein (arrows)
A B
Fig. 4. A. Longitudinal US image at the suprapatellar area of the right knee demonstrates several anechoic tortu- ous vascular channels in and around the suprapatellar fat pad (asterisk), mainly projecting into the suprapatel- lar bursa.
B. The same scan of a color Doppler US image reveals numerous enlarged vessels.
A B
Fig. 5. Axial T1 weighted SE image (A) (TR/TE, 700/12) and T2 weighted spin- echo image (B) (TR/TE, 2000/20, 2000/80) shows numerous signal voids (arrows) in the suprapatellar fat pad, mainly projecting into the distended suprapatellar bursa. There was large amount of joint effusion and thick in- trapatellar plica in the right knee.
A B C
Fig. 6. A. Femoral angiogram shows an abnormal dilated feeding artery (arrows) originating from the right femoral artery.
B. Superselective arteriogram shows a dilated and tortuous feeding artery (arrows) and nidus (arrow heads) in the early arterial phase.
C. Superselective arteriogram shows early draining vein (arrows) with dilated and tortuous feeding artery and nidus in arterial phase.
normality (1, 4). Recently Berry et al proposed the in- volvement of a somatic mutation for a factor critical to vasculogenesis and angiogenesis in embryologic devel- opment (2).
Hemangioma in KTWS are usually located in the skin of the lower extremity, but it can extend deeper to sub- cutaneous tissue, muscle, bone, and visceral organs, which may lead to internal hemorrhage (3, 5).
Limb hypertrophy develops later in life. It is usually due to subcutaneous tissue hypertrophy, but can associ- ate with bone hypertrophy, which results in leg length discrepancy. A leg length discrepancy of over 1.5 cen- timeters requires orthopedic correction (2). KTWS has several other osseous manifestations, such as syndactly, polydactly, and congenital hip dislocation (1).
A superficial varicosity of the affected limb is a charac- teristic finding in KTWS. KTWS patients often have deep venous malformations, such as aplasia, hypopla- sia, duplication, or abnormal venous valve formation.
There is also significant reflux in normal veins. Deep ve- nous malformation is an important factor in deciding to operate on a superficial varicosity. An operation for su- perficial varicosities is contraindicated in patients with abnormalities of the deep venous system, so venogra- phy and Doppler sonography are performed to evaluate the deep venous system (1, 2, 4, 5). In our case, no deep venous malformation was observed, but there was sig- nificant reflux in the deep venous system.
AVMs are rare congenital vascular lesions character- ized by an abnormal connection between arteries and veins. Arterial blood is shunted to the venous system in a central confluence of tortuous vessels, called a nidus.
The AVMs are congenital and they do not involute (6, 7). Clinically significant AVMs are an essential finding for KTWS diagnosis (1-3, 5).
In KTWS, the AVMs are located in the extremities, visceral organs, or spinal canal (3). The AVMs associated with KTWS may be single or multifocal in the extremi- ty, or they may be diffuse and involve the entire extrem- ity and adjacent trunk (1, 3). AVMs in the extremities are usually intramuscular or cutaneous. This is the first report of KTWS-associated AVMs in the suprapatellar fat pad that caused painful swelling of the knee joint and hemarthrosis (1-7).
AVMs are usually diagnosed with multiple imaging modalities, which demonstrates a hypervascular lesion with a large feeding arterial vessel (7). Non-invasive imaging modalities such as MR imaging and Doppler sonography can be used for diagnosis of AVMs. On MR
imaging, the AVMs appear as a tangle of multiple signal voids, usually without focal discrete soft-tissue mass.
The lesions can also be associated with surrounding ede- ma or fibrofatty stroma (7). Doppler sonography of AVMs shows a high velocity, low resistance waveform (6, 7). Arteriography demonstrates a dilated tortuous feeding artery, nidus, and an early draining vein (6, 7).
We confirmed the presence of AVMs by MR imaging, duplex ultrasonography, and angiography. MR imaging showed multiple signal voids around the suprapatellar fat pad, and a Doppler sonogram with spectral analysis demonstrated vessels with arterial waveform, high ve- locity, and a decreased resistive index in the knee joint.
Femoral angiography showed a typical AVM in the knee joint.
Most complications of KTWS are related to the under- lying vascular pathology, such as pain, bleeding, throm- bosis, or pulmonary thromboembolism. Abnormal ves- sels in gut, kidney, or genitalia can cause severe bleed- ing (2).
In particular, the AVMs dilate progressively with age and can result in both local and systemic complications.
Local complications are pain, bleeding, tissue ulcera- tion, and impairment of limb function. AVMs can also cause cardiac overload, resulting in heart failure (6, 7).
In our case, the chief complication of AVM was painful swelling of the knee joint. There was no color change or bruising, which is usually noted in extremity AVMs. We did not suspect vascular malformation after physical ex- amination because of its location in the suprapatellar fat pad. Repeated aspirations of knee joint fluid during fol- low up were bloody, so we hypothesized that AVM caused a hemarthrosis.
Treatment of KTWS is conservative and symptomatic (1-3). For AVMs, surgery is extremely difficult and total removal is rarely possible. Superselective transarterial embolization is the most effective treatment for AVMs (6, 7).
In summary, an AVM associated with KTWS, al- though rarely located in the suprapatellar fat pad, may cause joint pain and hemarthrosis.
References
1. RY Kanterman, PD Witt, PS Hsieh, D Picus. Klippel-Trenaunay syndrome: imaging findings and percutaneous intervention. AJR Am J Roentgenol 1996;167:989-995
2. Berry SA, Peterson C, Mize W, Bloom K, Zachary C, Blasco P, et al. Klippel-Trenaunay syndrome. Am J Med Genet 1998;79:319 3. Amy Beth Goldman. Heritable disease of connective tissue, ephiphy-
seal dysplasia, and related condition. In Resnick D, Niwayama G.
Diagnosis of bone and joint disorders. 3rd ed. Philadelphia. W.B.
Sounders Company 1995;4153-4156
4. Al-Salman MM. Klippel-Trenaunay syndrome: clinical features, complications, and management. Surg Today 1997;27:735 5. GN Phillips, DH Gordon, EC Martin, JO Haller, W Casarella. The
Klippel-Trenaunay Syndrome: clinical and radiological aspects.
Radiology 1978:128:429-434
6. Yakes WF, Rossi P, Odink H. Arteriovenous malformation man- agement. Cardiovasc Intervent Radiol 1996;19:65-71
7. K. T. Tan, M. E. Simons, D. K. Rajan, K. Terbrugge. Peripheral High-Flow Arteriovenous Vascular Malformations: a Single-Center Experience. J Vasc Interv Radiol 2004;15:1071-1080
대한영상의학회지 2006;54:27-31
Klippel-Trenaunay-Weber 증후군에서 슬개골상의 지방대에서 발생한 동정맥기형: 증례 보고1
1충남대학교병원 진단방사선과
2충남대학교병원 정형외과
박미현・권순태・신병석・김영모2
Klippel-Trenaunay-Weber 증후군은 동정맥 기형을 동반한 혈관 질환이다. 피부의 혈관종, 사지 비대, 그리고 정맥 류를 보이는 Klippel-Trenaunay-Weber증후군 환자에서, 슬개골상의 지방대에 동정맥 기형이 위치한 증례를 보고하 고자 한다. 자기공명영상, 색도플러 초음파, 혈관 조영술에서 우측 슬개골상의 지방대에 위치한 동정맥 기형을 확인하 였다.